
Case Report | DOI: https://doi.org/10.31579/IJBR-2021/057
1Third-year medical student, California Northstate University College of Medicine Elk Grove, California USA –
2Emergency Physician, St. Agnes Medical Center, Fresno, California USA
3Professor and clerkship director of Emergency Medicine, California Northstate University, Elk Grove, California, USA
*Corresponding Author: Leonard Ranasinghe PhD MD, Professor and clerkship director of Emergency Medicine, California Northstate University, Elk Grove, California, USA.
Citation: Khanna, Niloufar, Peralta, Samantha, Zhang, Rayven, Thiesen, Jordan DO, Ranasinghe, Leonard (2022) Schistosomiasis of the Cervix: Thyroid Storm: An Elusive but Deadly Diagnosis -- A Case Report. International J. of Biomed Research. 2(3): DOI: 10.31579/IJBR-2021/057
Copyright: © 2022, Leonard, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 November 2021 | Accepted: 15 December 2021 | Published: 14 January 2022
Keywords: thyroidsStorm (TS), propylthiouracil (PTU), methimazole (MMI), propranolol, graves disease; ttrial fibrillation; amphetamines; against medical advice (AMA); counseling
Thyroid Storm is an elusive topic to many researchers and clinicians. It is an emergent medical condition that is challenging to diagnose, is associated with many precipitating factors, and has a mortality rate of 10% with treatment. In this report, we discuss the case of a 37-year- old Asian female brought in by ambulance for right flank pain associated with subjective fever. Of significance in the patient's history is amphetamine abuse and hyperthyroidism for which she is non-compliant with her medication. Laboratory results in the Emergency Department (ED) corroborated a diagnosis of thyroid storm and urinary tract infection (UTI). She was significantly tachycardic with evidence of atrial fibrillation for which direct current (DC) cardioversion was attempted unsuccessfully in the ED. The patient was admitted to the intensive care unit (ICU) for thyroid storm and was then downgraded to the floor later the same evening for observation. The patient was in the hospital for 5 days, after which she left against medical advice (AMA). We discuss the treatment and management of Thyroid Storm as well as the unique and multifaceted implications of our patient’s case and how these factors may have precipitated her thyroid storm, as well as implications for identifying and counseling at-risk patients.
Thyroid storm (TS) is a medical emergency, which is very challenging to diagnose, given that there are no specific laboratory abnormalities specific to the condition, and diagnosis is made based on a scoring system of clinical criteria [1]. TS, a rare but severe manifestation of thyrotoxicosis (excessive circulation of thyroid hormones), exists in an estimated .22% of all thyrotoxic patients and can often be the first clinical presentation of thyrotoxicosis. This is a medical emergency given the associated high morbidity and mortality rates [9]. TS was first described as “the crisis of exophthalmic goiter” due to the fact that many patients suffering from the condition had an exacerbation of underlying Graves’Disease. The disease can be caused by a multitude of factors, including but not limited to non-thyroidal surgery, manipulation of the thyroid, medication exposure, diabetic ketoacidosis, hypoglycemia, molar pregnancy, infection,
Emotional stress, and intense exercise. This disorder is characterized by multi-organ decompensation resulting in altered mentation (psychosis, agitation, extreme lethargy, coma), high fever (>100.4 F), tachycardia (median heart rate 100.5 bpm), congestive heart failure, GI and hepatic disturbance. Diagnostic criteria include thermoregulatory dysfunction, CNS dysfunction, GI and hepatic dysfunction, and cardiovascular dysfunction. Mortality is often associated with shock, disseminated intravascular coagulation, and multi-organ failure. Often, there is an identifiable precipitating event [2, 3].
Because of the challenges associated with diagnosing TS, multiple methods have been proposed to aid in the diagnosis of the condition. The two most prominent methods of diagnosis are the Burch-Wartofsky Point Scale for the Diagnosis of Thyroid Storm, [1] and the Japanese Thyroid Association Criteria for Thyroid Storm [2]. The Burch-Wartofsky scale is a point-based scale that assigns points based on the presence and severity of symptoms affecting the CNS, cardiovascular, and GI system. it also assigns points to the presence and severity of a fever and a precipitating history. The score values range from 0 to 140, with a score of below 25 unlikely to represent TS, a score of 25 to 44 suggesting impending storm, and a score of 45 or above indicating a high likelihood of thyroid storm [1]. While the Japanese Thyroid Association Criteria for Thyroid Storm is a more generalized criteria and proposes that at least one CNS manifestation has to be present for a definitive diagnosis of TS, which they define as TS1. Furthermore, it defines TS2 as a lower grade TS that has symptoms of TS1 but does not have CNS involvement. Other than the CNS symptoms, the symptoms used to determine TS1 or TS2 also include presence of fever, tachycardia, Congestive Heart Failure (CHF), GI/Hepatic Manifestations, and most importantly, thyrotoxicosis as a prerequisite for making a diagnosis. These criteria are supported by the review which found over 80% of TS patients have tachycardia, and over half of TS patients have symptoms stated in the criteria such as CNS symptoms, GI symptoms, and fever [2]. It is to be noted, however, that both of these criteria do not represent definitive methods of diagnosing TS, but rather an aid to help confirm the suspicion of TS, clinical judgement is still crucial in the diagnosis of the condition.
Despite many studies and case reports, there are still significant gaps in our knowledge of TS. There is no full understanding of the trigger of TS, although nonadherence to anti-thyroid medication and infection are among the most common triggers of TS, there are still a significant portion of cases with unidentifiable causes [2,3]. The exact mechanisms that lead to the development of TS from uncomplicated thyrotoxicosis are still not well understood, although theories have suggested possible increases in sensitivity to thyroid hormones [3]. Furthermore, even with the two existing diagnostic criteria mentioned earlier, there is still no definitive way to identify and diagnose TS due to its extremely variable and dynamic presentation. Additionally, there is no uniform effective treatment for TS. Both of these factors have led to a high mortality rate for the disorder, even when treated. Our study will focus on a patient case of TS following the use of methamphetamine, which could provide insight into the use of stimulants and onset and presentation of TS, a phenomenon that has not been extensively explored before.
This patient showed signs and symptoms of TS including elevated T3 and T4, atrial fibrillation, high bilirubin levels, hyperglycemia, lightheadedness and subjective fever in the context of underlying hyperthyroidism. The precipitating event appears multifactorial including hyperthyroid medication non-compliance, methamphetamine abuse, and UTI. In this paper, we will discuss the details of our patient’s case and the implications for the medical community in terms of prevention of TS and management of patients with the condition.
Patient description:
The patient is a 37-year-old Asian female brought in by ambulance for right flank pain associated with subjective fever. The patient had a history of hyperthyroidism diagnosed as Graves Disease, although she was unaware of this specific diagnosis. She had been prescribed medication for her hyperthyroidism however she did not know the names of her medications. The patient stated that she had been non-compliant because she “does not like taking pills.” She had a history of methamphetamine abuse and reported last using amphetamines 3-4 days ago.
Additionally, the patient had a history of hypertension, uterine cancer, bilateral tubal ligation, and C-section.
Case history:
The patient was brought in by ambulance for right flank pain that began one day ago with associated subjective fever. Her pain had been progressively worsening, was rated at an 8/10 in severity, and was made worse upon palpation. She denied dysuria, hematuria, nausea or vomiting upon presentation. She further denied the possibility of pregnancy and reported her last menstrual period (LMP) to be approximately 3 weeks ago. Additionally, she reported lightheadedness. Initial working diagnoses included kidney stone and/or pyelonephritis. The patient’s initial vital signs are shown in Figure 1 below. She was normotensive and hemodynamically stable.


She later developed dysuria and shortness of breath while still in the Emergency Department. As her condition progressively worsened, so too did her vital signs. Further review of systems results were unremarkable, and the patient continued to be normotensive and hemodynamically stable.
Physical examination results:
Of significance in the patient’s vital signs was a heart rate (HR) of 114 bpm and a respiratory rate (RR) of 22. She appeared to be in severe distress and was lethargic.
Cardiovascular examination revealed evidence of tachycardia (reaching rates up to 178bpm) with an irregularly irregular rhythm consistent with atrial fibrillation. There was right flank tenderness without costovertebral angle (CVA) tenderness. Further physical exam results were unremarkable, and the patient was hemodynamically stable and normotensive.
Results of pathological tests and other investigations:
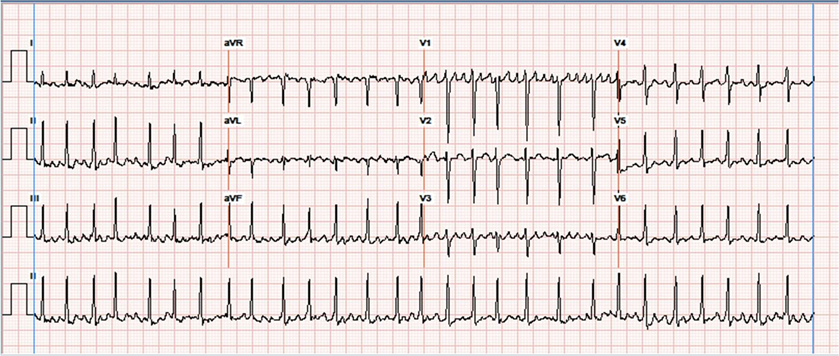
Electrocardiogram revealed evidence of atrial fibrillation. Significant laboratory results included an elevated lactate, high T3 and T4, low TSH, positive presence of amphetamines in the urine, proteinuria, hematuria, hyponatremia, hypokalemia, hyperglycemia, hypocalcemia, high alkaline phosphatase, high total and direct bilirubin, and a high percentage of segmented neutrophils.
Treatment Plan
Differential diagnoses included methamphetamine intoxication, thyroid storm, sepsis, UTI and electrolyte abnormality. Interventions included monitoring for hemodynamic management (post cardioversion), IV propranolol, IV iopamidol, IV magnesium sulfate, IV fluid boluses and PTU. The patient reported feeling “much better” after IV propranolol which lowered her heart rate to 140-150bmp. DC cardioversion is performed unsuccessfully in the ED in attempt to control the patient’s atrial fibrillation. She was then admitted to the ICU for persistent tachycardia in conjunction with her UTI. Upon admission, the primary diagnoses were thyroid storm, UTI, methamphetamine abuse and hypokalemia. In the ICU, the patient was treated with propranolol, PTU, potassium iodide, hydrocortisone and ceftriaxone. Urine amphetamines were positive, however it was noted in the documentation that the patient did not appear to be acutely intoxicated with methamphetamines, in which administration of a beta blocker could lead to unopposed alpha adrenergic stimulation. Thyroid ultrasound was performed and revealed findings related to thyroiditis including 2 small nodules on the left thyroid lobe. The ICU progress note stated that after treatment the patient was doing well with a HR in the 70’s and on no pressors. The patient was then transferred to the medical floor with telemetry. On the medical floor, PTU, propranolol, hydrocortisone and ceftriaxone were continued. Patient discharge was pending improvement of her clinical state including leukocytosis, culture results and IV steroids for her thyroid storm. IV steroids were slowly tapered down on the floor and the patient became eager to go home. The patient was counseled about switching from IV to oral steroids and from PTU to MMI and it was requested that the patient stay overnight to monitor her response to treatment. The patient left AMA and was unable to be found. The patient’s total hospital course was 5 days. Her last known vitals are shown below in Figure 3.

According to the Burch-Wartofsky Point Scale for the Diagnosis of Thyroid Storm, our patient would have a score of 75, which is well beyond the 45 points required to be highly suggestive of thyroid storm. According to the Japanese Thyroid Association Criteria for Thyroid Storm, the patient would also be classified as TS1, which is a definitive case of TS.
Risk Factors and Conditions associated with Thyroid Storm:
Provided that the diagnosis of TS is difficult and multifaceted, it is important to understand the risk factors that can lead to thyroid dysfunction. Demographically associated risk factors are being female and increased age [4]. Many drugs can alter thyroid hormone synthesis and
circulating thyroid hormone levels, specifically the common cardiac drug, amiodarone, which is used in the management of arrhythmias. Amiodarone has the potential to cause both hyper and hypothyroidism. Amiodarone inhibits deiodination enzymes (responsible for the deiodination of thyroid hormones) resulting in an amiodarone-induced hypothyroidism [5]. Conversely, amiodarone can induce thyrotoxicosis in approximately 3% of patients through the breakdown of thyroid follicular cells resulting in the release of thyroid hormones into circulation [6]. Currently, amiodarone-induced thyrotoxicosis is only predicted by age less than 62 [7]. Additionally, as amiodarone is a popular drug with a generic option available, there is no significant difference in thyroid function between patients using the name brand amiodarone vs generic for the treatment of atrial fibrillation [1]. It is recommended that patients taking amiodarone have baseline thyroid function tests performed and that they have these tests repeated every 3 months while taking the drug [12].
Common precipitating events for the development of TS include the abrupt discontinuation of antithyroid medication, trauma, thyroid or non-thyroid surgery, acute illness such as infection, myocardial infarction, cardiac failure, drug hypersensitivity or adverse reaction, childbirth, radioiodine therapy, use of iodine contrast medium, stroke, burns, severe emotional distress, vigorous exercise, and pulmonary embolism. In addition to amiodarone, notable drugs that have TS as an adverse effect include anesthetics and salicylates. It is important to determine whether a patient has sepsis, cocaine use, infection, malignant hyperthermia, neuroleptic malignant syndrome, pheochromocytoma, or psychosis, as these disorders can present similarly toTS [8].
The management of TS typically includes a drug to inhibit thyroid hormone synthesis, such as PTU, carbimazole, or MMI. However, the potential for liver toxicity with PTU makes MMI or carbimazole the first-choice thioamide. This is typically administered along with an iodine drug to inhibit hormone release, such as Potassium Iodide (Lugol’s solution), or Iapionic acid. These iodine containing medications should be given at least an hour after administering the thioamide drug in order to ensure blockade of preformed thyroid hormone release. Through the Wolff-Chaikoff effect, large doses of iodine will suppress the release of thyroid hormone.
Along with the thioamide and an iodine containing agent, treatment typically involves a beta blocker to address tachycardia, such as Propranolol, Esmolol, or Metoprolol, although Diltiazem may be used if beta blockers are contraindicated. Supplementary management includes the use of steroid medications to prevent peripheral conversion of T4 into T3, such as Hydrocortisone, Dexamethasone, and Acetaminophen/Paracetamol. Additional therapy may include Lithium Carbonate to inhibit thyroid hormone release from the gland, Potassium Perchlorate to inhibit iodide transport into the thyrocyte, and cholestyramine to block enterohepatic circulation [9].
Management of TS also requires treatment of the underlying cause. Any patient with a diagnosis of TS should be screened for infection, trauma, and myocardial infarction, diabetic ketoacidosis or other triggering events that caused the attack. Often, the treatment of TS involves treatment of the underlying disorder resulting in extreme hyperthyroidism. For example, treatment of Graves-induced hyperthyroidism involves the use of Anti-CD-antibodies, such as Rituximab [7].
TS may persist despite the above measures, in which case other treatment options should be considered. Plasmapheresis of the patient’s blood to remove excess thyroid hormone has been successfully used to treat TS and as prophylaxis against thyroid storm following thyroid surgery [10]. When plasmapheresis is used, less than 20% of the T4 pool and even less of the T3 pool can be removed in one session, and so multiple sessions are required. Charcoal hemoperfusion has also been demonstrated as a method of removing excess thyroid hormone from the blood in thyroid storm [11]. Unfortunately, treated TS has a mortality of 10% [3].
We believe that our case will add to the currently limited knowledge on the diagnosis and management of TS and elucidate the multifaceted nature of the disease. Our patient presented with a concomitant UTI, which is likely to have been the precipitating factor. However, our patient had many associated comorbidities, including previously diagnosed hyperthyroidism, a history of uterine cancer, uterine surgery, and amphetamine abuse as well as a history of medication noncompliance. Additionally, our patient left against medical advice after being treated. Our case has interesting implications regarding the importance of patient education and identifying barriers to accessing care. For example, our patient was not aware that she had a diagnosis of Graves’ Disease, which may have contributed to her medication non-compliance.
Additionally, her amphetamine abuse likely significantly increased her risk.
Future directions of research include developing effective methods of identifying and counseling patients regarding the risk of thyroid storm; particularly among those with a prior diagnosis of hyperthyroidism and a precipitating risk factor, such a UTI or drug abuse.
Furthermore, additional work needs to be done in identifying barriers to care for at-risk patients, and in creating resources for patients who face barriers in complying with treatment, so as to prevent this life-threatening disease.
We would like to acknowledge Dr. Ranasinghe for his mentorship, and Drs. Thiesen and Alhadi for providing us with the case.
The authors have no conflicts of interest to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
