
Research Article | DOI: https://doi.org/10.31579/2641-0419/361
Cardiology department, Candela Nursing Home – Palermo
*Corresponding Author: Pietro Candela, Cardiology department, Candela Nursing Home – Palermo.
Citation: Pietro Candela, D Picone, L Ajello, MCE. Valerio, P. Camarda, V Mineo, et.al (2024), Thymoma Presenting as Right-Side Heart Failure in a Healthy Patient: A Case Report, J Clinical Cardiology and Cardiovascular Interventions, 15(1); DOI: 10.31579/2641-0419/361
Copyright: © 2024, Pietro Candela. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 March 2024 | Accepted: 03 April 2024 | Published: 15 April 2024
Keywords: anterior mediastinal mass; thymoma; heart failure; right ventricle
Thymoma is a rare tumor yet the most common neoplasm of the anterior mediastinum, accounting for 20-25% of all mediastinal tumors. Its incidence peaks in the fourth and fifth decades of life. Usually thymoma is diagnosed incidentally on chest imaging, or when investigating patients with myasthenia gravis, or with chest symptoms such as cough, chest pain, or dyspnea. We report here an unusual case of recidivant thymoma presenting with right heart failure in a 69 years old man.
Thymoma is an uncommon tumor originating from the epithelial cells of the thymus [1]. It is best known for its association with myasthenia gravis (MG) which occurs in about 50% of patients with thymoma. Most cases occur between the ages of 40 and 60 years [2] with a mean age at presentation being 52 years. Thymoma may present in three main different ways: 30-50% of patients present with an asymptomatic anterior mediastinal mass on chest roentgenogram. Around one-third of patients are diagnosed during the evaluation of MG or other paraneoplastic syndromes such as pure red cell aplasia or acquired hypogammaglobulinemia [3], and one-third of cases present with local symptoms such as cough, superior vena cava syndrome, chest pain, or dysphagia among others [1]. This report describes a case of thymoma in a male patient who presented with a picture of right-side heart failure with ascites and lower limbs edema.[4]
Case Report
In January 2024, a 69 year old man was hospitalized in our department for anasarcatic state and reduced exercise tolerance. The patient had been living in USA for several years, and came back to Italy few months before.
He had an history of thymoma (45 year ago) reported spontaneous regression (associated with a diet with prolonged fasting). The last CT scan of 2019 didn’t show any sign of thymoma
Since the end of 2021 you have noticed initial signs of salt and water congestion but all the test performed to at Chicago hospital were negative.
For about a year and a half he has been reporting episodes of edema in the lower limbs and in the scrotal and abdominal areas, associated with exertional dyspnea and bendopnea. He denies angina. For this reason, in June 2022 he performed a physical stress echocardiogram in America: good functional capacity (10.1 METS), left ventricle of normal size and wall thickness, EF 65%, right sections within limits; no valvular disease; no evidence of inducible ischemia; hospitalization was proposed, refused.
In November 2023 he performed a chest-abdomen CT scan with contrast medium which showed subtle pleural effusion on the right, in the early contrastographic phase opacification of the right suprahepatic vein, the inferior cava, the renal, the iliac and the lumbar veins which appeared enlarged of caliber as per probable cardiac deficiency.
In January, he had a cardiology consult in our institution and, seen the anasarcatic state, he was hospitalized.
The patient presented into NYHA class III, with clinical and echocardiographic signs of congestion (anasarcatic state with massive edema of the lower limbs up to the root of the thighs, abdominal congestion, presacral edema, jugular swelling)

Figure 1: dilated inferior vena cava

Figure 2: Tricuspid regurgitation; triangle shape of CW, demonstrating high atrial pressure
We also performed a contrast-enhanced chest CT performed during this hospitalization: No evidence of signs of pulmonary embolism. Compared to the previous control, a neoformation was detected in correspondence with the thymic lodge, measuring 7.4cm x 6.6cm vs 6.3cm x 5.2cm, with gross calcifications in the context, with lobed margins and with offshoots that extend into the anterior segment of the lobe. superior, and which rests partly on the superior wall of the right ventricle and on the common trunk of the pulmonary artery. (figure 3)
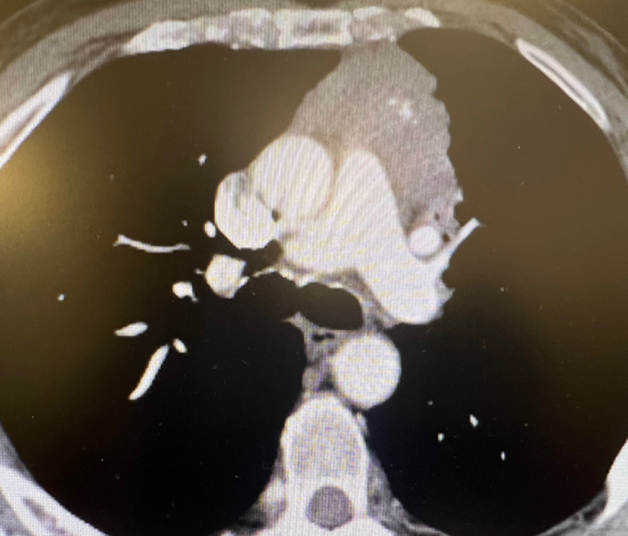
Figure 3: CT scan showing thymoma extension and contiguity with pulmonary arthery
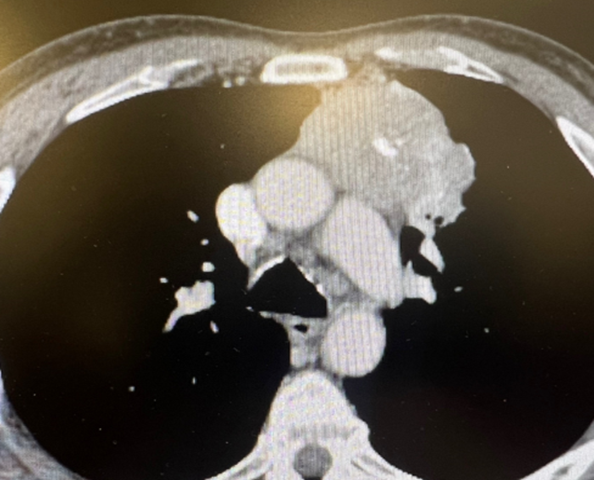
Figure 4: Calcificated thymoma – other CT scan
Good conditions of haemodynamic compensation were restored during diuretic therapy with venous furosemide in bolus (40 mg) and infusion (80 mg/24 hours).
On the discharge echocardiogram: the presence of the D shape of the SIV is confirmed. FE VS biplane 57.4%. Paradoxical movement of the SIV associated with the D shape, suggestive of pulmonary hypertension. Compared to the previous VD reduced in basal dimensions (34mm). Reduced TAPSE remains (14mm); 's TDI in normal operation (11). RFVFAC 38%. IT is better evaluated which, in a valve with a redundant aspect, presents two jets, overall it is of a moderate-severe degree. The PAPs for the triangular profile indicative of rapid equalization (in progress with V max 2.6m/s) cannot be estimated. VCI 24mm with no excursions (it was 32mm at entry). Coronary sinus 1 mm (compared to 1.5 mm inlet). No pleural effusion.
The initial optimization of the therapy was carried out by inserting sartan, antialdosterone and SGLT 2 inhibitor.
Daily dose of furosemide at discharge 125 mg. (before current hospitalization daily dose of 25 mg of torasemide)
The patient we present show an unusual case of recidivant thymoma presenting with pulmonary hypertension complicated by cardiomyopathy, heart failure predominantly affecting the right sections, with signs of mild impairment of renal function (cardio-renal syndrome).
Echocardiographic data show presence of pulmonary hypertension. We have sent the images of the thoracoabdominal CT to thoracic surgeon. A We are concluding the diagnostic process by performing cardiac MRI, right catheterization. After that, the cardiothoracic team will evaluate indication to surgical removal of thymoma.
This case remembers us that a patient with history of thymoma should always be carefully evaluated for the possible development of right heart failure.
Early recognition and diagnosis with timely and complete resection are essential for a better prognosis and higher survival rate.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
