
Short Commentry | DOI: https://doi.org/10.31579/2690-8808/114
*Corresponding Author: Tsuneo Ishida, Saido, Midoriku, Saitama City, Saitama Prefecture,336-0907 2-3-6, Japan
Citation: Tsuneo Ishida, Saido , Midori-Ku , Saitama-Shi and Saitama-Ken (2022) Thrombosis prevention and anti-thrombus formation by zinc(Ⅱ) ions against COVID-19 infection Journal of Clinical Case Reports and Studies 3(6); DOI: 10.31579/2690-8808/114
Copyright: © 2022 Tsuneo Ishida, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 April 2022 | Accepted: 02 May 2022 | Published: 25 June 2022
Keywords: Zn2+ ion; bronchial epithelial integrity; lung inflammation; platelet activation; blood coagulation; thromboembolism; anti-thrombus formation; Zn2+ ions-centered coordinated binding proteins
Zinc induced COVID-19 thrombosis prevention and anti-thrombus formation have been established by that zinc promotes COVID-19 thrombosis prevention and anti-thrombus formation and zinc ions-induced activated anti-thrombus activity is proceeded to prevent acute ischemic stroke among COVID-19 patients
Zinc can reduce neurological outcomes in COVID-19 patients that Zn2+ promotes inflammatory cytokine as a neurodegenerative disorder and the coronaviruses can affect the nervous system through blood circulation, causing neuro-inflammation.
Zinc supplementation affects bronchial mucosal epithelial integrity, both under normal and zinc deficient conditions. The other, zinc ions inhibit COVID-19 lung inflammation that zinc ions promote platelet activation function that inhibits pulmonary thromboembo-lism, in which platelets could respond to changes in extracellular and intracellular Zn2+ concentration.
Zn2+ plays a major role in the regulation of coagulation that zinc inhibit blood coagulation against COVID-19 infection, in which Zn2+ can modulate platelet and coagulation activation pathways, including fibrin formation that the release of ionic Zn2+ store from secretory granules upon platelet activation contributes to the procoagulant role of Zn2+ in platelet-dependent fibrin formation.
Zinc-induced platelet aggregation, low concentrations of ZnSO4 and zinc chelation involve platelet activation and potentiated platelet aggregation. Persistent zinc intake for severe aggravation of COVID-19 has been suggested to be 8–11 mg/day for adults (tolerable upper intake level 40 mg/day) and suggesting that a zinc intake of 30–70 mg/day might aid in the RNA viruses control.
Thus, zinc ions can inhibit inflammation, platelet behaviour function, blood coagulation, and neurological thrombus formation during ROS production and excessive oxidative stress against COVID-19 infection. Zn2+ ions-binding with many proteins-molecular mechanism has been clarified that Zn2+ ions may be bound with COVID-19 inflammatory, platelet, coagulation, thrombus proteins by Zn2+ ions-centered tetrahedrally binding protein molecular coordination pattern.
ACE2=angiotensin-converting enzyme 2. ARDS=acute (adult) respiratory distress syndrome, ATE=arterial thromboembolism,
CAC=COVID-19-associated coagulopathy, COVID-19=coronavirus disease-2019, COVID AtoZ=COVID-19, Using Ascorbic Acid and Zinc Supplementation, CRP=collagen-related peptide, CUS= compression ultrasound, CVD=cardiovascular diseases, DRI=dietary reference intake, DVT=deepvein thrombosis, ER= endoplasmatic reticulum, ICU=intensive care unit, MPO= myeloperoxidase, NIH=National Institutes of Health, NOAEL=no observed adverse effect level, PE=pulmonary embolism, RDA=recommended daily allowance, RDI=recommended dietary intake, RBC=red blood cell, RdRp=RNA-dependent RNA Polymerase, ROS=reactive oxygen species, SARS=severe acute respiratory syndrome coronavirus 2, TMPRSS2=transmembrane serine protease 2, TNF=tumor necrosis factor, TRPV1=transient receptor potential vanilloid 1, VTE=venous thromboembolism,
Epidemiological and clinical characteristics against COVID-19 infection are involved with bronchial thrombosis, viral pneumonia with virus spreading and inflammation, and thrombus formation and growth by blood coagulation. The immune dysregulation characteristic of severe COVID-19 infection may be initiated by a particularly pro-inflammatory form of apoptosis with rapid viral replication leading to massive release of inflammatory mediators, which resulting in thrombus formation and eventually death [1]. Common factors of venous thromboembolic disease and microvascular thrombosis in the lungs and other organs are involved in producing both large vessel thrombosis (deep vein thrombosis, pulmonary embolism, stroke, myocardial infarction) and microvascular thrombosis, in which microvascular thrombosis in lung capillaries is common in adult respiratory distress syndrome (ARDS) and is particularly prominent in COVID-19 pneumonia [2]. COVID-19 thrombosis features are expressed as venous thromboembolism (VTE) included pulmonary embolism (PE) and deep vein thrombosis (DVT), in which the main characteristics of VTE in COVID-19 are the capacity to affect all in-hospital patients, regardless of intensive care unit (ICU) or non-ICU stay, severity of pneumonia, and degree of respiratory failure and PE is common, often affects the most distal branches of the pulmonary arteries and can arise without concomitant DVT, suggesting the possibility of primary pulmonary thrombosis [3]. VTE prophylactic measures should be given to all hospitalized patients with COVID-19, especially in the ICU setting. Since approximately one-fourth of patients admitted to the ICU setting developed VTE, careful monitoring of the patients for VTE and its complications is strongly advised [4].
Thrombus formation process consists complicatedly of possessing numerous aspects and mechanisms of coagulation, blood clotting factor, platelet activation and aggregation, and embolization [5]. COVID-19 infection results thrombosis of comsumption coagulo-pathy that progression of inflammation mediated hemostasis dysregulation to thrombotic outcomes leads cause of abnormal coagulo-pathy [6]. In addition, an association between COVID-19 Infection and the occurrence of neurological disorders in neurolysis procceses is particulaly noteworthy for severe COVID-19 complicate patients [7]. The complications of formation of unusal blood clots (thrombosis) during COVID-19 infection lead to increased risk of thrombosis. COVID-19 thrombus process may consist of inflammatory activation, cytokine production, coagulation, thrombin generation, fibrin deposition, and blood clotty formation that a thrombus occurs when the hemostatic process, which normally occurs in response to injury, becomes activated in an uninjured or slightly injured vessel. A thrombus in a large blood vessel will decrease blood flow through that vessel (termed a mural thrombus). In a small blood vessel, blood flow may be completely cut off (termed an occlusive thrombus), resulting in death of tissue supplied by that vessel. If a thrombus dislodges and becomes free-floating, it is considered an embolus [8].
On the other hand, zinc as thrombus formation inhibitors plays an important role that zinc ions-mediated angiotensin-converting enzyme 2 (ACE-2) activation may promote anti-thrombotic activity. SARS-CoV-2 viral host entry depends on ACE2 and transmem-brane serine protease 2 (TMPRSS2) that SARS-CoV-2 RNA binds platelet ACE2 to promote thrombus formation. Spike protein recombinant human ACE2 protein and anti-spike monoclonal antibody could inhibit SARS-CoV-2 spike protein-induced platelet activation [9]. Zinc is also an important trace element for immune cells and important enzymes that 0.01‐0.1 mM Zn2+ induced significant reductions of clotting times in a concentration‐dependent manner. The procoagulant effect of Zn2+ occurred in the presence of Ca2+ but was inhibited by metal chelating agents. Higher levels of Zn2+ (> 0.2 mM final concentration) were required to accelerate thrombin‐induced clot formation in the presence of citrate or oxalate. Similarly with oxalated human plasma, > 0.2 mM Zn2+ decreased the clotting time [10]. Further, zinc-induced neurological promotive anti-thrombosis as neurobiology frontier that zinc-induced thrombus research had been carried out that lower zinc concentration (0.1 to 0.3 mmol/l) induces aggregation of washed platelet suspensions and higher concentrations (1 to 3 mmol/l) of zinc were needed to aggregate platelets in platelet-rich plasma obtained from blood anticoagulated with low-molecular-weight heparin. The outcomes have been obtained that zinc increases the rate of thrombin-induced fibrin clot formation and inhibits thrombin inhibition by antithrombin, and that zinc plays an important role in hemostasis, platelet aggregation, thrombosis, and atherosclerosis [11].
Thus, zinc is involved in blood clot formation that there is a lot of evidence linking zinc to blood clotting. Zinc is released from cells called platelets that control blood clotting, and unwanted blood clots can form when zinc levels in the blood are faulty. It is unclear whether zinc inhibits VTE including pulmonary PE and DVT. Zinc induced COVID-19 thrombosis prevention and anti-thrombus formation have been established by that zinc ions-induced activated anti-thrombus activity is proceeded to support an ideal medical treatment for COVID-19 patients presenting with acute ischemic stroke or to prevent acute ischemic stroke among COVID-19 patients and zinc promotes COVID-19 anti-thrombus formation.
In this review article, firstly, zinc(Ⅱ) induced COVID-19 thrombosis prevention of respiratory thrombosis and pulmonary thrombo-embolism is discussed. secondly, Zn2+ ions-induced COVID-19 anti-inflammation, anti-platelet function, anti-coagulation, and anti-thrombus formation during thrombus process are debated, subsequent to the thromboic influence of ROS and oxidative stress are argued, and lastly, the zinc-binding molecular mechanism is clarified.
Thrombus process in COVID-19 infection
COVID-19 thrombus process is involved with the coagulation and the thromboembolism. The coagulopathy of COVID-19 presents with prominent elevation of D-dimer and fibrin/fibrinogen degradation products, whereas abnormalities in prothrombin time, partial thromboplastin time, and platelet counts are relatively uncommon in initial presentations [12]. Further, COVID-19 may result in immunothrombosis and venous thromboembolism (VTE) that multifactorial processes are likely to contribute to VTE and immunothrombosis in COVID-19 [13]. Thrombus process becomes underlying that COVID19-associated coagulopathy (CAC) seems to join SARS-CoV-2 RNA virus to spike protein ACE2 receptor, endotheall injury, abnormal blood flow, platelet activation, platelet-derived thrombin, and immuno-thrombosis [3], in which proinflammatory cytokine release can induce the release of platelets and their activation and aggregation, complement activation is an important inducer of coagulation, and the generation of CAC, as a defence mechanism by neutrophils, also promotes coagulation [14].
Thus, the thrombus process is considered to be consist of inflammatory activation, cytokine production, coagulation, thrombin generation, fibrin deposition, and blood clotty formation.
Zinc induced COVID-19 neurological anti-thrombus activity
COVID-19 in neurological disorders can present with a large increase in systemic pro-inflammatory cytokines as a neurodegenerative disorder that zinc may promote inflammatory cytokine storms and the coronaviruses can affect the nervous system through blood circulation and cause neuroinflammation [15]. COVID-19 thrombosis is of particular importance to the neurologist that cardiovascular diseases (CVD) is the leading cause of neurological co-morbidity in COVID-19. Furthermore, venous thromboembolism (VTE) is a leading complication of most neurological conditions. In the COVID-19 thrombosis, (1) Widespread activation of this ‘thromboinflammatory’ response can result in sepsis induced coagulopathy, multi organ dysfunction, (2) SARS-CoV-2 can invade vascular endothelial cells, causing the loss of the normal anticoagulant function of the endothelium, (3) Loss of anticoagulant function combines with platelet hyperactivity, enhanced leucocyte tissue factor expression and complement activation release of neutrophil extracellular traps associated with the proinflammatory state in COVID-19 patients [16].
Zinc induced COVID-19 neurological anti-thrombosis with acute neurologic infectious patients is involed that neurological COVID-19 acute ischemic stroke in thrombus process occurs in a higher probability of early mortality and zinc ions-induced activated anti-thrombus activity is proceeded to support an ideal medical treatment regimen for patients presenting with acute ischemic stroke or to prevent acute ischemic stroke among hospitalized COVID-19 patients. This is underscored by one study that found admitted patients with COVID-19 were experiencing acute ischemic stroke in spite of therapeutic anticoagulation [17].
Zinc ion concentration is average 10 mg/g (wet weight) for mammal brain and roughly amounts to 0.15 mM for the blood serum and in extracellula fluid. In zinc nervous system, zinc deficiency results in behavioral symptoms, such as memory problems, malaise, or higher susceptibility to stress. Zinc in excess or deficit will cause pathological conditions that toxic levels of zinc have been shown to induce lethargy, neurotoxicity, and gliotoxicity, and high levels of zinc causes neuronal death in cortical cell tissue culture [18]. Hence, an excess of free zinc is detrimental and can lead to neuronal death. Zinc induced COVID-19 neurological anti-thrombus has been established by that zinc may promote COVID-19 neurological anti-thrombus, zinc dyshomeostasis may also be a hallmark of ageing and several neurological disorders [19]
Zinc ions prevent respiratory thrombosis and pulmonary thromboembolism in COVID-19 infection
The role of thrombosis in the disease process of COVID-19 contributes to the morbidity and mortality of infected patients. While manifestation of VTE and arterial thrombosis in the neurovascular system is recognized. Thromboembolism prevention is necessary that the neurovascular and cardiovascular systems, as the manifestation of thromboembolic phenomenon in these two systems varied, suggest different pathophysiology of damage. Further research into the role of thromboembolism in COVID-19 is important to advance the understanding of the virus, its effects and to tailor treatment accordingly to prevent further casualties from this pandemic [20]. The defense on the severe bronchitis patients infected with SARS-CoV, MERS-CoV and SARS-CoV-2 has clinical features range from mild respiratory illness to severe acute respiratory disease. Both MERS and SARS patients in later stages develop respiratory distress and renal failure. The pneumonia appears to be the most frequent manifestation of SARS-CoV-2 infection, characterized primarily by fever, cough, dyspnea, and bilateral infiltrates on chest imaging that the period from infection to appearance of symptoms varies [21].
Zinc has the potential to reduce inflammation, improve mucocillary clearance, prevent of ventilator-induced lung injury, and modulate antiviral immunity. Zinc is an important cofactor in haemostasis and thrombosis that zinc compounds such as anti-coagulant [22], blood clotting [23], and thrombotic complication [24] can promote subsets of the reactions of the contact pathway, with implications for a variety of disease states and prove useful in preventing thrombosis and the formation of obstructive clots.
Zinc can prevent COVID-19 thrombosis that the contribution of extracellular or intracellular Zn2+ to megakaryocyte and platelet function and dysregulated Zn2+ homeostasis in platelet-related diseases by focusing on thrombosis, ischemic stroke and storage pool diseases. Consequently, zinc ions can impair the coagulation pathway and fibrin clot formation in humans, which can be more critical in patients with combined defects of both α and δ-granules or with thrombocytopenia [25].
Zinc plays a complex role in haemostatic modulation acting as an effector of coagulation, anticoagulation and fibrinolysis. The effectiveness of zinc intake in preventing or treating SARS-CoV-2 infections is considered that the daily recommended dietary intake (RDI) of elemental zinc is around 2 mg for infants up to 6 months of age and gradually increases to 11 mg for males and 8 mg for females older than 13 years. Tolerable upper limits for zinc are estimated to be 7 mg for children aged 1–3 years of age, increasing up to 25 mg for adults and females of any age who are pregnant or lactating. The no observed adverse effect level (NOAEL) for adults is around 50 mg/day [26]. Zinc lozenges with a daily dose of >75 mg of zinc may shorten the duration of the common cold. A daily dose higher than 100 mg of elemental zinc in a lozenge is probably not advisable, as it is questionable whether there are any additional therapeutic effects. [27]. Thus, zinc (by using 30~50~75 mg/day-zinc lozenges or 0.01‐0.2 mmol/L solution Zn2+ ) could prevent COVID-19 respiratory and pulmatotry thrombus formations.
Further, zinc finger anti-viral proteins (ZAPs) could prevent respiratory thrombosis and pulmonary thromboembolism by inhibition of thrombus formation growth in COVID-19 infection [28].
Zinc ions inhibit COVID-19 respiratory thrombus formation
COVID-19 enters the target cells through the angiotensin-converting enzyme 2 (ACE2) receptor and the transmembrane protease, serine 2 (TMPRSS2). The TMPRSS2 inhibitors block the cellular entry of the SARS-CoV-2 virus through the downregulated priming of the SARS-CoV-2 spike protein [29]. COVID-19 can cause mild respiratory infections or severe acute respiratory syndrome with consequent inflammatory responses that considering inflammation plays a significant role in COVID-19 pathology. Anti-infla-mmatory treatments may hold promise for the management of COVID-19 complications [30].
COVID-19 respiratory system disorders such as respiratory tract epithelium, alveolar epithelium and interstitium, vascular endothelium, and excessive respiratory drive could lead to venous thromboembolic disease and pulmonary microvascular thrombosis [31]. Zinc used as anti-inflammatory agent inhibits transient receptor potential vanilloid 1 (TRPV1) to alleviate neuropathic pain [32] that TRPV1 might decrease the severity of the acute respiratory distress syndrome present in COVID-19 patients [33].
Zinc could decrease thrombus formation in a clinical context that zinc supplementation of the zinc deficient diet group affected the integrity of the bronchial epithelium was shown by the number and length of cilia, and the number of epithelial cells [34].
Thus, COVID-19 respiratory system disorders such as respiratory tract epithelium, alveolar epithelium and interstitium, vascular endothelium, and excessive respiratory drive could lead to venous thromboembolic disease and pulmonary microvascular thrombosis.
Zinc ions modulate pulmonary thromboembolism against COVID-19 infection
The role of ACE2 in multiple organ damage caused by COVID-19 and SARS-CoV, targeted blocking drugs against ACE2, and drugs that inhibit inflammation in order to provide the basis for subsequent related research, diagnosis and treatment, and drug development [35].
The presence of lung thrombosis seems a universally recognized feature of COVID-19 disease whether these thrombi can resolve in response to anticoagulant therapy is still matter of debate. Transient clinical improvement upon treatment with high dose of anti-coagulants could be observed within an old, organized thrombus detached from the arterial wall, consistent with re-canalization of the vessel [36].
Zinc induced ACE2 activation promotes activity of anti-thrombus formation and growth against COVID-19 infection that zinc activates COVID-19 ACE2 as entry receptor that zinc induced ACE2 activation promotes the activity of anti-thrombus formation growth, in which ACE2 activation decreases thrombus formation and reduces platelet attachment to vessels [37].
Further, treatment of zinc supplement for cardiovascular diseases (CVD) and COVID-19 comorbidity should be preventing viral replication by inhibiting the RNA-Dependent RNA Polymerase (RdRp) of the SARS-CoV-2, and enhance protective immune responses, and restoring functional balance of ACE2 [38].
However, the role of zinc in regulation of inflammatory response was important, aspects of the regulatory role of zinc in pneumonia pathogenesis, and zinc ions may inhibit COVID-19 lung inflammation. Zn2+ ions may possess anti-inflammatory effects in pneumonia with limiting tissue damage and systemic effects. How anti-coagulation that occlusive pulmonary embolism (PE) strongly support a hypercoagulable state incurred by SARS-CoV-2 and the medical community to share a perspective about long-term management guidelines for SARS-CoV-2 associated venous thromboembolism (VTE) and prompt future research [39].
The potential role of zinc as an adjuvant therapy for SARS-CoV-2 may be broader than just antiviral and/or immunological support. Zinc also plays a complex role in haemostatic modulation acting as an effector of coagulation, anticoagulation and fibrinolysis [40].
Zn2+ accelerates clot formation by enhancing fibrin assembly, resulting in increased fibre thickness that Zn2+ promotes clotting and reduces fibrin clot stiffness in a Factor XIII or fibrin stabilizing factor (FXIII)-independent manner, suggesting that zinc may work in concert with FXIII to modulate clot strength and stability [41].
Zinc ions is a platelet agonist that zinc-induced platelet aggregation involves secondary mediators of platelet activation and low concentrations of ZnSO4 potentiated platelet aggregation by collagen-related peptide (CRP-XL), thrombin and adrenaline. Chelation of intracellular zinc reduced platelet aggregation induced by a number of different agonists, inhibited zinc-induced tyrosine phosphorylation and inhibited platelet activation in whole blood under physiologically relevant flow conditions [42].
Zn2+-induced platelet activation is integrin aIIbb3-dependent that Integrin αIIbβ3 is expressed at a high level in platelets and their progenitors, where it plays a central role in platelet functions, hemostasis, and arterial thrombosis. Thus, zinc ions promote platelet activation that Zn2+-induced platelet activation is integrin aIIbb3-dependent, contribute to the procoagulant role in platelet-dependent fibrin formation, and leading to modulation of thrombosis formation [43].
Zn2+ plays a major role in the regulation of coagulation that zinc inhibit blood coagulation against COVID-19 infection, activated platelets secrete zinc into the local microenvironment, the concentration of zinc increases in the vicinity of a thrombus. Consequently, the role of zinc varies depending on the microenvironment; a feature that endows zinc with the capacity to spatially and temporally regulate haemostasis and thrombosis [44].
Zinc ions promote platelet activation function that inhibits pulmonary thromboembolism, in which the influence of Zn2+ on platelet behaviour during thrombus formation and the contributions of exogenous and intracellular Zn2+ to platelet function are assessed, and the potential pathophysiological implications of Zn2+ signalling are evaluated having the mechanisms by which platelets could respond to changes in extracellular and intracellular Zn2+ concentration [45].
Thus, zinc regulates coagulation, platelet aggregation, anticoagulation and fibrinolysis and outlines how zinc serves as a ubiquitous modulator of haemostasis and thrombosis.
Zn2+ also circulates in the blood plasma at a concentration of 10–20 µM. Zn2+ can modulate platelet and coagulation activation pathways, including fibrin formation that the release of ionic Zn2+ store from secretory granules upon platelet activation contributes to the procoagulant role of Zn2+ in platelet-dependent fibrin formation [46].
Zn2+ ions-induced platelet activation, blood coagulation, and thrombosis formation are mediated that persistent zinc ion concentration for aggravated COVID-19 patient is involved that zinc intake for severe aggravation of COVID-19 suggesting that the recommended daily allowance (RDA) of zinc according to the Dietary Recommendation Intake (DRI), is 8–11 mg/day for adults (tolerable upper intake level 40 mg/day) and that a zinc intake of 30–70 mg/day might aid in the COVID-19 RNA virus control [47]. Thus, 50 mg Zn/day caused a factor to increased platelet reactivity, which could cause a predisposition to increased coagulability without altering the platelet count [48]. The other, low zinc levels were established if zinc levels were <70 level=70>[49, 50].
Accordingly, COVID-19 ACE2 is an integral membrane-bound zinc-metallopeptidase that zinc ions can inhibit inflammation, platelet behaivour function, blood coagulation, and thrombus formation against COVID-19 infection. Zinc influences thrombocyte aggregation and coagulation, indicating that zinc could decrease thrombus formation. In addition, COVID-19 mutation also possesses a high thrombophilic risk, but zinc ions could inhibit the coagulation and the thrombus formation [51].
Thus, COVID-19 respiratory system disorders such as respiratory tract epithelium, alveolar epithelium and interstitium, vascular endothelium, and excessive respiratory drive could lead to venous thromboembolic disease and pulmonary microvascular thrombosis.
The Zn2+ ions-binding molecular mechanism is considered that zinc ions may be bound by zinc ions centered tetrahedrally binding proteins molecular coordination.
Zinc induced ROS generation in COVID-19 infection
In COVID−19 infections, the large artery inflammation secondary to the cytokine storm results in the formation of unlimited quantities of reactive oxygen species (ROS) produced through activation of the mitochondrial respiratory chain, peroxisomal fatty acid metabolism, and flavoprotein oxidases. In addition, COVID-19 infection is associated with the generation of interleukins and tumor necrosis factor (TNF α), which increase neutrophil myeloperoxidase (MPO) activity. Excessive MPO activity can generate the Fenton reaction to further produce ROS that including the highly reactive hydroxyl radical (•OH), superoxide (O2•−) and hydrogen peroxide MPO-H2O2 [52]. Oxidative stress by ROS is related to all the main changes observed in other inflammatory and infectious diseases. The host’s response to viral infection emphasizes oxidative stress rather than the virus’s mechanisms of aggression [53].
The high neutrophil to lymphocyte ratio observed in critically ill patients with COVID-19 is associated with excessive levels of ROS, which promote a cascade of biological events that drive pathological host responses. ROS induce tissue damage, thrombosis and red blood cell (RBC) dysfunction, which contribute to COVID-19 disease severity. Free radical scavengers could be beneficial for the most vulnerable patients. Excessive oxidative stress might be responsible for the alveolar damage, thrombosis and RBC dysregulation seen in COVID-19. Anti-oxidants and elastase inhibitors may have therapeutic potential [54].
ROS are involved in the regulation of all of the major processes that promote the formation of venous thrombi. These include coagulation; platelet reactivity; and sterile inflammation during formation. Oxidative stress also appears to control the remodeling of a venous thrombus and adjacent vein wall including fibrinolysis; sterile inflammation (monocyte accumulation); extracellular matrix deposition and its remodeling; and neovascularization [55]. DVT formation and resolution are influenced by ROS through modulation of the coagulation, fibrinolysis, proteolysis and the complement system, as well as the regulation of effector cells such as platelets, endothelial cells, erythrocytes, neutrophils, mast cells, monocytes and fibroblasts. Consistence with a functional association between Zn2+ and ROS production in platelets that could inhibit thrombus formation in a clinical context [56].
Recently, a functional association between zinc and ROS production in platelets indicate that zinc could decrease thrombus formation in a clinical context. Complications of SARS-CoV2 infections also include tissue damage affecting the gastrointestinal system, the liver, kidneys, blood vessels. In this regard it should be mentioned that a balanced zinc homeostasis is essential for wound healing and tissue recovery after mechanical and inflammation-mediated damage, adding more potential benefits of zinc supplementation of COVID-19 patients.
Thus, Zinc influences thrombocyte aggregation, coagulation, and thrombosis that complications of SARS-CoV2 infections also include tissue damage affecting the gastrointestinal system, the liver, kidneys, blood vessels.
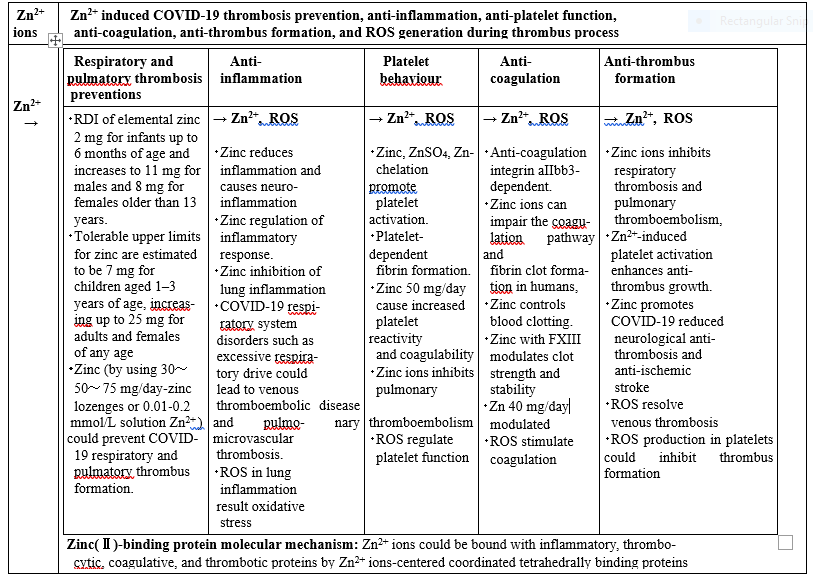
As mentioned above, zinc(Ⅱ)-induced thrombosis prevention and anti-inflammation, platelet activation, blood anti-coagulation, reducing neurological thrombotic formation, and ROS production during thrombus process against severe COVID-19 infection are expressed in Table 1. Accordingly, zinc ions-binding proteins molecular mechanism becomes clarified that zinc ions could be bound with inflammatory, thrombocytic, coagulative, and thrombotic proteins by Zn2+ ions-centered coordinated tetrahedrally binding proteins.
Zinc(Ⅱ) induced COVID-19 thrombosis prevention and anti-thrombus formation have been discussed during thrombus process and ROS production, and subsquently zinc-binding proteins molecular mechanism is clarified.
Zinc induced COVID-19 ACE2 activation as entry receptor promotes activity of anti-thrombus formation and growth that the ACE2 activation decreases thrombus formation and reduces platelet attachment to vessels. Thrombus process becomes underlying that COVID19-associated coagulopathy seems to join SARS-CoV-2 RNA virus to spike protein ACE2 receptor, abnormal blood flow, platelet activation, platelet-derived thrombin,and immunothrombosis.
Neurological COVID-19 acute ischemic stroke in thrombus process occurs in a higher probability of early mortality and zinc ions-induced activated anti-thrombus activity is proceeded to support an ideal medical treatment regimen for patients presenting with acute ischemic stroke or to prevent acute ischemic stroke among hospitalized COVID-19 patients.
Zinc can prevent COVID-19 thrombosis that zinc modulates antiviral immunity, has the potential to reduce inflammation, improves mucocillary clearance, and prevents of ventilator-induced lung injury. Zinc plays a complex role in haemostatic modulation acting as an effector of coagulation, anticoagulation and fibrinolysis. The zinc intake in preventing or treating COVID-19 infection is around 2 mg for infants up to 6 months of age and gradually increases to 11 mg for males and 8 mg for females older than 13 years. Tolerable upper limits for zinc are estimated to be 7 mg for children aged 1–3 years of age, increasing up to 25 mg for adults and females of any age.
Zinc ions can inhibit COVID-19 inflammation, platelet behaviour function, blood coagulation, and thrombosis formation.
Zinc supplementation affects the integrity of the bronchial epithelium that zinc inhibits COVID-19 respiratory thrombus formation, and zinc promotes platelet activation function that inhibits pulmonary thromboembolism, in which the potential pathophysiological implications of Zn2+ signalling are evaluated having the mechanisms by which platelets could respond to changes in extracellular and intracellular Zn2+ concentration with Zn2+-induced platelet activation is integrin aIIbb3-dependent from which the influence and the contributions of Zn2+ on platelet behaviour during thrombus formation
Zinc inhibit blood coagulation against COVID-19 infection that Zn2+ can modulate platelet and coagulation activation pathways, including fibrin formation that the release of ionic Zn2+ store from secretory granules upon platelet activation contributes to the procoagulant role of Zn2+ in platelet-dependent fibrin formation.
Persistent zinc intake for severe aggravation of COVID-19 has suggested that Recommendation Intake (DRI) is 8–11 mg/day for adults (tolerable upper intake level 40 mg/day), suggesting that a zinc intake of 30–70 mg/day might aid in the RNA viruses control.
Zinc induced lung inflammatory ROS productions lead to that especially, ROS induce tissue damage, thrombosis and RBC dysfunction, which contribute to COVID-19 disease severity that free radical scavengers could be beneficial for the most vulnerable patients. Excessive oxidative stress might be responsible for the alveolar damage, thrombosis and RBC dysregulation seen in COVID-19. Thus, zinc ions can inhibit inflammation, platelet behaviour function, blood coagulation, and thrombosis formation during ROS production, excessive oxidative stress, and thrombosis process against COVID-19 infection.
Thus, zinc inhibits respiratory thrombosis, pulmonary thromboembolism, and thrombus formation and growth in COVID-19 infection. In addition, the zinc ions-binding molecular mechanism pattern has been, resulting that the Zn2+ ions-proteins complexes promote anti-thrombasis formation activity may be bound with COVID-19 inflammatory, platelet, coagulation, thrombus proteins by Zn2+ ions-centered tetrahedrally binding protein molecules coordination pattern, resulting that the Zn2+ ions-proteins complexes promote anti-thrombasis formation activity.
The author declares there is no conflicts of interest.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
