
Research Article | DOI: https://doi.org/10.31579/2639-4162/042
1 Department of Radiation Medicine Oregon Health and Science University
2 Department of Neurological Surgery Oregon Health and Science University
3 Department of Radiation Oncology Indiana University School of Medicine
4 Department of Radiation Medicine Oregon Health and Science University
5 Department of Radiation Medicine Oregon Health and Science University
6 Department of Neurosurgery University of Florida Gainesville, Fl
7 Department of Neurological Surgery Oregon Health and Science University 8Department of Radiation Medicine Oregon Health and Science University
*Corresponding Author: Brandon Lucke-Wold, Department of Neurosurgery University of Florida Gainesville, Fl.
Citation: Wencesley Paez, Rohi Gheewala, Shearwood McClelland, Jerry J. Jaboin, Charles R. Thomas, Brandon Lucke-Wold., (2021) Three-Year Experience of a Multidisciplinary Central Nervous System Clinic Model for Radiation Oncology and Neurosurgery (RADIANS) in a Community Hospital Setting. J. General medicine and Clinical Practice. 4(1) DOI:10.31579/2639-4162/042
Copyright: ©2021 Brandon Lucke-Wold, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 January 2021 | Accepted: 08 April 2021 | Published: 16 April 2021
Keywords: central nervous system; metastatic disease; multidisciplinary clinic; neurosurgery; radians; radiation oncology; radiation therapy
Background: As academic centers partner and establish healthcare systems with community hospitals, delivery of subspecialty, multidisciplinary care in community hospital settings remains a challenge. Improving outcomes for central nervous system (CNS) disease is related to integrated care between neurosurgery (NS) and radiation oncology (RadOnc) specialties. Our multidisciplinary community hospital-based clinic, RADIANS, previously reported high patient approval of simultaneous evaluation with NS and RadOnc physicians. Three-year experience is now reported.
Methods: Prospectively collected clinical and demographic patient data over three years was done, and surveys administered. Descriptive statistics reported as mean and percentages for patient characteristics, diagnosis, treatment and outcomes.
Results: Between August 2016 and August 2019, 101 patients were evaluated. Mean age and distanced traveled was 61.2 years, and 54.9 miles, respectively. Patient Satisfaction Score was 4.79 (0-5 Scale, 5-very satisfied). Most common referral source was medical oncologists. Seventy-two patients had malignant CNS disease (brain mets 28; spine mets 27; both 6; primary brain 9; primary spine 2), 29 had benign CNS disease. Post-evaluation treatment: radiation therapy (RT) only (n=29), neurosurgery (NS) only (n=16), both RT and NS (n=22), and no RT/NS intervention (n=34). Fractionated stereotactic radiosurgery was most common RT delivered; craniotomy with tumor resection was most common NS performed. Treatment outcomes: local control=61/67 (91%); radiation necrosis or radiation-induced myelitis=2/51 (3.9%).
Conclusions: The RADIANS multidisciplinary community hospital-based CNS clinic model is first of its kind to be reported, continuing strong patient approval at extended follow-up. Data indicates the model serves as a regional referral center, delivering evidence-based treatment modalities for complex CNS disease in community hospital settings, yielding high rates of local control and low rates of grade 3 or 4 radiation-induced toxicity.
SHORT TITLE: RADIANS: Multidisciplinary CNS Clinic
Central Nervous System Disease
In 2019, it is estimated that 23,800 adults (13,400 men and 10,400 women) in the United States will be diagnosed with primary malignant tumors of the brain and spinal cord. Brain tumors alone account for nearly 85% of all primary CNS tumors. Brain and other CNS malignancies are considered the 10th leading cause of death for men and women, and roughly 35% have a five-year survival rate when diagnosed. [1,2] It is without question indeed, that the care of patients with CNS disease, both malignant and benign, requires the expertise of specialized providers in a collaborative and multidisciplinary approach to administer the best treatment options and optimize patient outcomes and care.
Multidisciplinary Clinics
Currently with managed care at the forefront of healthcare systems, medical centers are encouraged to develop and implement clinical delivery systems that collaborate with different providers and specialists with the overall goal to improve quality of care, reduce practice variation, define and measure treatment outcomes, and to minimize treatment costs. This is certainly more evident in the setting of cancer care, such that it provides patients with the opportunity to see their providers in one clinic, lessens the travel burden, and allows for concurrent provider visits. [3] Numerous MDC modeling and approaches have been reported for cancer care. The findings have shown to increase overall survival, slow disease progression, improve patient compliance, increase adherence to treatment guidelines, promote early treatment intervention, and decrease treatment costs. [4-8]
RADIANS
In the fall of 2016, the novel RADIANS (RADIation oncology And NeuroSurgery) clinic was formed at a local community hospital as a collaboration between radiation oncology and neurosurgery physicians to evaluate central nervous system disease in one clinic setting. The MDC was formed to align with the delivery of quality of care, as outlined by the American Society of Clinical Oncology (ASCO) [9] for the better part of the community for which it serves. The RADIANS clinic proved to be highly favorable from the patient’s view in terms of overall experience and satifisfaction. [10]
METHODS
With approval from the Institutional Review Board (IRB), a prospective patient registry was developed, and clinical and demographic data were collected. Data was stored in a secure database where only IRB-approved research team members had access. Patients that were referred into the RADIANS clinic were seen simultaneously by both physicians, the radiation oncologist and neurosurgeon, in a single clinic visit setting. Prior imaging and workup were reviewed before the initial visit. Discussion regarding diagnosis and treatment options were done and questions were answered. Family members and/or caregivers were included in the discussion with the consent and approval of the patient. A patient survey was given to all patients prior to the conclusion of their visit to collect data regarding overall patient experience and satisfaction. Patients had the option of completing the survey before leaving the clinic or returning the survey in the mail.
In total, 101 patients were evaluated in RADIANS from August 2016 through August 2019 with CNS disease. Patient characteristics are presented in Table 1.
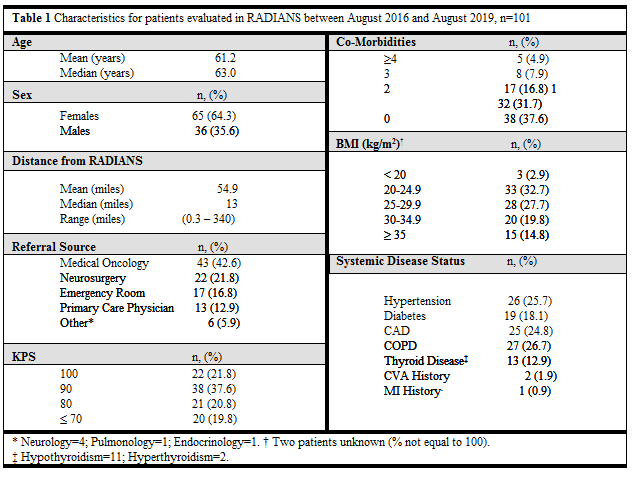
The mean patient age was 61.2 years and females nearly doubled the number of males seen (F=65; M=36). Patients travelled an average of 54.9 miles (median = 13.0; range = 0.3 to 340) for their initial clinic visit. Patient Satisfaction Score (PSC) was 4.79 (respondents, n=39). PSC was calculated on a 0-5 scale, 0=not satisfied and 5=very satisfied.
Patterns of referral were as following: approximately half (42.6%, n=43) were referred from medical oncologists. Systemic disease status of patients evaluated in RADIANS showed eighty percent having a Karnofsky Performance Status (KPS) of ³ 70 and about two-thirds (61.4%, n=62) had at least one co-morbidity, while 12.9% (n=13) had three or more at the time of their initial visit. The two most common co-morbidities seen in the clinic were chronic obstructive pulmonary disease (26.7%, n=27) and hypertension (25.7%, n=26). Twenty patients had an Obesity Class I classification [BMI (kg/m2) = 30-34.9] and 15 had an Obesity Class II classification [BMI (kg/m2) = 35-39.9]. [11]
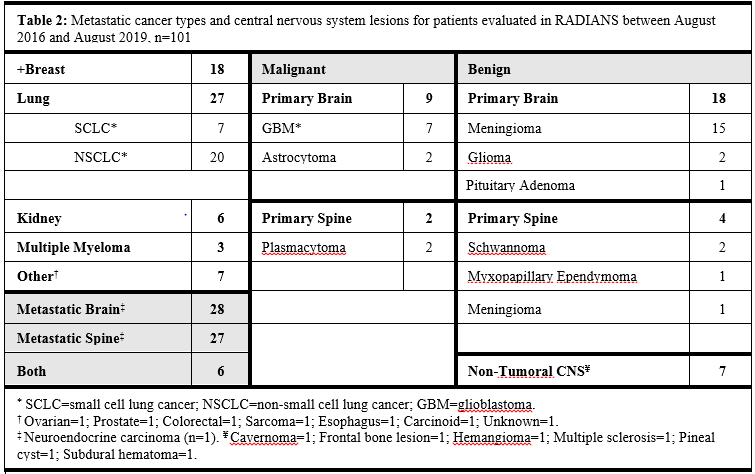
Patients with eleven different histologies were evaluated in RADIANS, see Table 2. Lung cancer (26.7%, n=27) was the most common metastatic cancer diagnosis, of which 73% (20/27) were non-small cell lung cancer. Breast cancer (17.8%, n=18) was the second most commonly seen metastatic malignancy. Of the primary brain malignancies evaluated, glioblastoma (81.8%, 7/9) was most commonly diagnosed. Among patients with primary benign CNS brain lesions, meningiomas were most commonly diagnosed (83.3%, 15/18).
More than half of patients evaluated at the RADIANS clinic received radiation therapy with no surgical intervention (54.5%), with fractionated stereotactic radiosurgery being the most common type (74.5%) of radiation therapy delivered. Two patients with a diagnosis of glioblastoma (2/7, 28.6%) received tumor treating fields (TTF), one of whom received both conventional fractionated RT and TTF to follow, see Table 3.
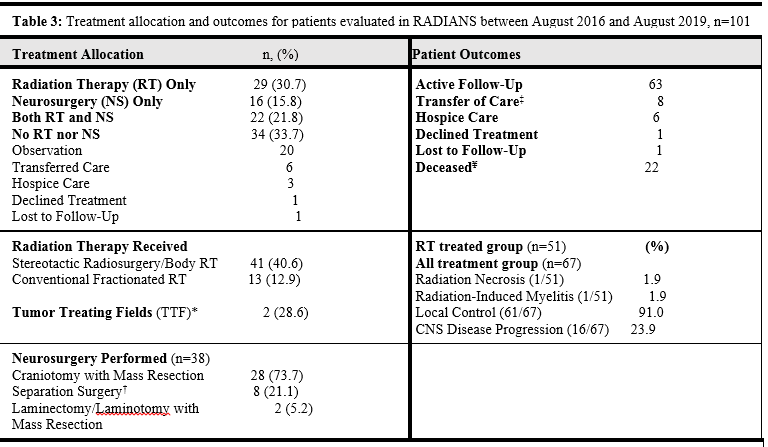
Nearly a quarter of patients (24%) received both radiation and neurosurgical intervention. Craniotomy with mass resection was the most common neurosurgical intervention [Table 3]. Since the beginning of this study, 22 patients are deceased, and 6 patients have entered hospice. Of the 22 patients, 86% (n=19) had stage IV metastatic cancer. A low rate of radiation necrosis or myelitis (2/51, 3.9%), and a high rate of local control (61/67, 91%) was experienced.
The Multidisciplinary Tumor Board provides patients with CNS malignancies the most coordinated care for their complex diseases. Current models have shown success in both pediatric and adult CNS disease. [12,13] Research also shows that multidisciplinary teams result in better clinical and organizational outcomes for patients. [14] While the use of weekly or monthly multidisciplinary tumor boards to review select oncologic cases has been adopted at many institutions, formal single-site, single-day multidisciplinary clinics have not been common.
When the RADIANS MDC clinic model was first established, investigators hypothesized that the model would optimize patient and physician time by reducing clinic visits and avoiding unnecessary duplication of tests, while improving quality of care, delivering evidence-based treatment modalities, and providing access for on-going clinical trials. Contrary to standard tumor boards, this model serves a unique role for the patient and their caregivers because of its direct involvement with patients and their caregivers in the discussion of their treatment plan. Despite advances in surgical procedures, chemotherapy, and targeted molecular and radiation therapies, breakdown in the continuum of cancer treatment can remain high. [15] This breakdown is attributed to failure of communication with involved providers resulting into delays in treatment, increased patient anxiety, decreased patient satisfaction, and declines in quality of life. [16]
One unique feature of the RADIANS clinic is that it is based at a small community hospital. Patient approval remains high since the initial published report back in July 2018. Trending similarly, patient volume has increased. The previous report showed a total patient census of 42 since the start---a span of approximately two years. [10] Since that published report, the clinic has seen a marked increase in patient volume (n=101), a 140.5% increase. The increase could be attributed to several factors. Our analysis identified that the current MDC model favors an improved practice pattern that’s patient-centric. The simultaneous provider visits increase efficiency in the workup and management for newly diagnosed CNS disease, fostering faster collaborative decision-making, thus avoiding potential treatment delays and additional referrals to another specialist. Both radiation oncologist and neurosurgeon prior to the new patient visit, review the workup, imaging, and labs and engage dynamically, interdependently, and adaptively towards a common goal. Dialogue between the two specialists are structured to adhere to standard clinical practice guidelines---an integral component for a successful MDC. [16]
Our data also shows that patients come from a vast array of provider referrals and varying degrees of systemic disease status. Primary care physicians and medical oncologists may refer patients into RADIANS for further workup with associated neurologic focal signs and preliminary work-up with imaging and labs, whether benign or malignant CNS disease. Patient referrals that come from emergency room consults are the direct result from patients requiring immediate neurosurgical intervention and are then referred to RADIANS for post-op workup, or from patients presenting with stable disease requiring further management and workup. Patients are then given treatment recommendations offering various radiation therapy planning or neurosurgical intervention based on standard of care guidelines whether for curative or palliative intent. All of which are openly discussed with the patients and their caregivers---a dynamic that patients showed high appreciation for based on the administered surveys.
We acknowledge, however, limitations to the current clinic model and our three-year experience. Patient scheduling and clinic flexibility can be challenging as the clinic is dependent upon provider availability. As the clinic continues to expand and grow, flexibility could be achieved by the addition of more clinic days or providers for broader coverage. Another area that should be pursued is the impact and effect the MDC clinic model may have on the caregivers involved. Their role in the overall quality of cancer care should be considered. Finally, another area of consideration and not often studied, as pointed out by Fennel et al., [17] is how external regulatory influences (especially reimbursement incentives) play a role in the sustainability of MDCs in the community hospital setting. Despite these limitations, the model has proven to be highly effective in the community hospital setting for CNS disease.
CONCLUSIONS
To date, we are the first to report on an outpatient community hospital-based multidisciplinary CNS clinic model where patients with benign or malignant CNS disease are evaluated jointly and simultaneously by the radiation oncologist and neurosurgeon. Our three-year data demonstrates that the patient-centric, clinic model optimizes both patient and physician time and patient approval remains high at extended follow-up. The clinic model proves to be a reliable, regional referral center that contributes substantially to improving the care of cancer patients, while providing access to ongoing clinical trials.
RADIANS give patients the option to be evaluated and treated in the community hospital-based setting, rather than at large tertiary centers. Patients are offered evidence-based treatment modalities, where outcomes have shown to have low rates of post-radiation therapy side effects and good local control. Despite being in a community hospital setting, the clinical model could serve beneficial in larger urban medical centers.
Data collection and treatment analysis will continue as we investigate the potential cost-benefit, clinical long-term outcomes, morbidity and mortality rates, impact on caregiver outcomes, and possible mechanisms for early detection by means of vigilant follow-up and imaging surveillance.
CONFLICT OF INTEREST: Dr. Mitin receives research funding and consulting fees from Novocure, Inc., and personal consulting fees from Janssen. Dr. Ciporen is a consultant for spiWAY, but does not receive consulting fees. No other authors have any conflicts of interest to report.
FUNDING: No funding source was provided to conduct this study.
ACKNOWLEDGEMENTS: The authors are grateful for the entire Tuality/OHSU Cancer Center and the Tuality Community Hospital Neurosurgery Clinic for their outstanding patient care and coordination.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
