
case report | DOI: https://doi.org/10.31579/2639- 4162/072
1 Cardiology Department Guglielmo Da Saliceto Hospital; Piacenza, Italy.
2 Anesthesiology and ICU department Guglielmo da Saliceto Hospital; Piacenza, Italy.
*Corresponding Author: Francesco Di Spigno, MD, Cardiology Department Guglielmo Da Saliceto Hospital, Via Taverna Giuseppe, 49, 29121 Piacenza, Italy.
Citation: Francesco Di Spigno, Geza Halasz, Felice Perrino, Matteo Villani, Daniela Aschieri, (2022). Three Cases of Severe SARS-CoV 2 Pneumonia Complicated by Combined Venous and Arterial Thrombotic Events. J. General Medicine and Clinical Practice. 5(3); DOI:10.31579/2639- 4162/072
Copyright: © 2022 Francesco Di Spigno, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 July 2022 | Accepted: 05 August 2022 | Published: 12 August 2022
Keywords: arterial thromboembolic events; SARS-COV-2 pneumonia; venous thromboembolic events
Several studies suggested that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is associated with a hypercoagulable state leading to multisystem organ dysfunction. The present article describes three cases of patients with SARS-Cov-2 pneumonia complicated by venous and arterial thromboembolism. Case1 is a 51 year- old-man not vaccinated with severe SARS-Cov-2 pneumonia who developed extensive arterial thromboses and pulmonary embolism after few days from symptoms onset. Laboratory panel at hospital admission showed sign of ongoing inflammation and a severe Hypercoagulable state. Case2 is a 58 year-old-man not vaccinated at low cardiovascular risk with severe SARS-Cov-2 pneumonia complicated by anterior STEMI due to acute thrombotic occlusion of left coronary artery and massive bilateral pulmonary thromboembolism. Subsequently the patient presented an acute ischemic stroke despite being treated with triple antithrombotic therapy low molecular weight heparin (LMWH), aspirin and clopidogrel. Case 3 is a 75 year old man with an history of arterial hypertension that developed severe SARS-Cov-2 bilateral pneumonia. Doppler ultrasound of lower limb veins showed deep vein thrombosis of right main femoral vein. CT angiography of the chest ruled out sign of pulmonary embolization and underlined the presence of thrombus in the aortic arch. Physicians should be aware of these complications and remain vigilant for signs of VTE and ATE in the contextof the current
Learning points
In Covid-19 we need to be aware of thromboembolic events in the healing phase of the disease. Patients with Covid-19 may benefit from long-term anticoaugulation.
Several case reports [1-2] have demonstrated that venous thromboembolic events (VTEs) are prevalent in individuals hospitalized with SARS-Cov-2 pneumonia.
Few recent researches [3-5] have shown an increased incidence of arterial thromboembolic events in these patients, implyingthat systemic inflammation, long-established risk factors for VTE, as well as possible endothelial dysfunction predispose patients with severe SARS–CoV2pneumonia to VTE and arterial thromboembolic events (ATE). Here, we describethree cases of male patientswithout pathological conditionswho developed a severe form of SARS–CoV2 pneumonia complicated both by VTE and ATE.
Patient 1
A 51-year-old male returned from Equador with no prior SARS-COV2 vaccinations and no historyof cardiovascular diseasepresented to the Emergency Department/ED complaining of dyspnea and fever. The cardiac exam was unremarkable. A 12-lead electrocardiogram revealed sinus tachycardia with incomplete right bundle brunch. On admission, D-dimer was 28470 ng/ml (normal range 0-500 ng/ml) and serum C-reactive protein was 14.49 mg/dl (normal range 0-0.5 mg/dl). The nasofaringeal swab for SARS COV 2 was positive with subsequent genomic sequentation that validatedthe presence of equadoriant variant. Transtoracic echocardiography TTE revealed a left ventricular ejection fraction/LVEF of 55%, right ventricle enlargement (telediastolic diameter/DTD 42 mm), and two thromboticstratifications spanning the right ventricle's apex and right atrium (dimensions of 3 cm and 1 cm, respectively). Thoracic CT revealed bilateral interstitial pneumonia (visual score of 60%, figure n. 1a), and angio sequences confirmed the existence of right ventricular and atrial thrombi,as well as additional thrombotic apposition at the level of aortic istmus (figure n. 1b).

Figure 1a: HRCT at the time of pulmonary embolism.

Figure 1b: Angio-CT showing thrombotic apposition at the level of aortic istmus
Due to the low risk of neurological embolization of aortic thrombus, the cardiac surgeon ruled out any invasive procedures. As a result, the patientwas treated in the Intensive Care Unit/ICU with intravenous unfractionated heparin/UFH and a large dosage of steroids. During the hospitalization, the patient'sventilatory parameters progressively deteriorated, and he was intubatedand pronated. Aspergillus was found in a broncoalveolar lavage/BAL. Unfortunately after few days the patient died.
Patient 2
A 58-year-old male with no prior SARS-COV2 vaccination and no history of cardiovascular illness presented to the emergency department with chest discomfort and dyspnea. The nasofaringeal swab tested positive for SARS COV 2, and furthergenomic sequencing confirmedthe presence of the deltavariant. A 12-leadelectrocardiogram revealed anteriorST elevation consistent with STEMI. Coronary angiography revealed acute thrombotic occlusion of the left coronary artery/LAD (figure n. 2a), which was successfully treated by primary coronary angioplasty and stent implantation (Synergy 3,5 x 32 mm @ 18 atm). The final angiography was suboptimal because of a substantial thrombotic burden in the distal LAD with TIMI 0 low. Across the procedure, a glycpprotein Iib/IIa inhibitor (tirofiban) and a loading dose of ticagrelor were provided. TTE revealed a 35% LVEF with apical, lateral, and anterior wall akinesia in the medio-distal segments in the presence of biatrial thrombotic apposition. Additionally, the patient receivedintravenous UFH and was intubated as a result of acuterespiratory syndrome/ARDS. Thoracic computed tomography demonstrated bilateral interstitial pneumonia (visualscore of 70%), and angiograms revealed severe bilateral pulmonary thromboembolism, indicating the presence of additional thrombotic apposition at the level of the left atrium and left pulmonary veins (figure n. 2b).

Figure 2a : Coronary Angiography showing acute thrombotic occlusion of LAD
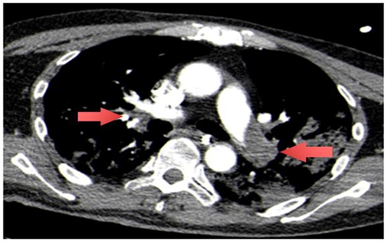
Figure 2b: Angio TC showing Filling defects at the level of right and left pulmonary artery
There was even an intercurrent sepsis caused by Staphylococcus aureuswith parossistic atrial fibrillation/FAP. Followingweaning from mechanical ventilation, the patient complained of right hemisome weakness. Without contrast agent, head CT revealedtwo ischemic lesionsin the left parietal lobe and right cerebellar lobe, both of which were cardioembolic in origin and were treated conservatively. The patient presented with a minor muscle deficit in the right hemisphere upon discharge, and contrast echocardiography demonstrated full clearanceof cardiac thrombotic apposition. Because the patient declinedwarfarin-based anticoagulation, dabigatran was administered in conjunction with dual antiplatelet treatment (cardioaspirin + clopidrogel) [6].
Patient 3
A 75-year-old male with a history of arterial hypertension who had previously been vaccinated againstSARS-COV2 (Vaxzevria, two injections) went to the emergency department complaining of dyspnea.Cardiac examination revealedno abnormalities. A 12-lead electrocardiogram exhibited a sinus rhythm. The D-dimer level was 1897 ng/ml (normalrange:0-500 ng/ml), while the serum C-reactive protein level was 4.91 mg/dl (normal range: 0-0.5 mg/dl). Doppler ultrasonography of the lower limb veins detected right main femoral vein thrombosis. The nasofaringeal swab for SARS COV 2 was positive, and a CT pulmonary angiography revealed bilateral interstitial pneumonia (visual score of 45%, figure n. 3a) and thrombus (maximal diameter of 10 mm) in the aortic arch, lower than the origin of the left subclavian artery(figure 3b). Any invasive treatments have been ruledout by the cardiac surgeon.Additionally, the patientreceived low molecular weight heparin/LMWH, as well as a high dosage of steroids and remdesivir. Warfarin was prescribed upon discharge.
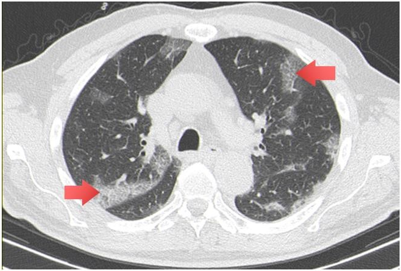
Figure 3a: HCRT on admission showing a diffuse bilateral“crazy paving” pattern with subpleural and peribronchial consolidation
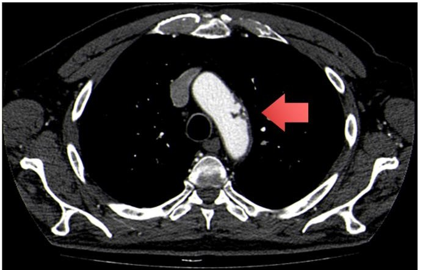
Figure 3b: AngioTc showingthrombus (diameter of 10 mm) at the level of aortic arch, lower than left subclavian artery origin
Severe SARS-CoV-2 infectionis associated with arterial and venous thrombotic complications including myocardial infarction (MI), ischemic stroke, and venous thromboembolism (VTE) [7].
The majority of studies have focused on venous thromboembolism, with the pulmonary circulation having substantially greater event rates than arm orleg veins [8].
Venous thrombotic complications occurred in 2.6 percent of 229 non- critically hospitalized patients and 35.3 percent of 170 critically ill hospitalized patients in a US registry of COVID-19 patients [9]. In two recent prospective researches from Italy, arterial thrombotic events had an incidence of roughly 10% [10].
Many patients with severe COVID19have an earlier stage of sepsis- associated disseminated intravascular coagulation (DIC) characterized as "sepsis-induced coagulopathy," according to the International Society of Thrombosis and Haemostasis (ISTH) (SIC) [11].
Thrombotic complications have been shown to have a significant impact in determining a patient's prognosis. Microthrombi seen in the lungs,heart, and kidneys after autopsy show that severe COVID-19 patients may suffer from multisystem organ failure due to thrombosis [12].
This disease-specific hypercoagulable state is thoughtto be caused by cytokine-mediated diffuse microvascular damage and, in some circumstances, reactive thrombocytosis. Obesity,advanced age, and hospitalization-related immobilization can all increasethe risk of thrombosis and pulmonary embolism [13].
Furthermore, Stress-induced cardiomyopathy (Takotsubo cardiomyopathy), paroxysmal atrial fibrillation, or paradoxical embolization through a patent foramen ovale in the context of pulmonary hypertension caused by acute lung injury could all be sourcesof embolism to the brain, splanchnic circulation, or peripheral arteries.In these critically ill individuals, vasospasmcaused by pressortreatment, iatrogenic artery damage, or spontaneous dissection are all possible explanations [14].
Moreover, elevated D-dimer levels levels have been found in COVID 19 patients,with a strong relation betweenelevated D-dimer levels on admissionand in-hospital mortality, raising concerns about potentially undetected pulmonary embolism in these patients[15].
Pulmonary embolism can also occur late in the course of the disease raisingthe possibility that the hypercoagulable state persist over the activeinflammation phase and cytokine storm [1].
In conclusion, our case studies highlight important cardiovascular consequences associated with COVID-19 pneumonia. The occurrence of arterial and venous thrombosis at the same time increases the risk of poor survival due to multisystem organ failure. The cytokine storm-related mechanism for this disease-specific hypercoagulable condition has been highlighted, and it may persist in the late stages of infection. Anticoagulant and antiplatelet therapy are required in this situation, however the time though they must be discontinued is unclear. Close radiologic (angio-CT, transtoracic echocardiography) and laboratory (dosage of D-dimer and C- reactive proteinlevels) follow-up is required after discharge in good clinicalpractice.
Ethics approval and consentto participate:
Not applicable
Consent for publication
All the patients involved in the current manuscript gave their consent for publication
Availability of data and materials
Data sharing is not applicable to this articleas no datasets were generated or analysed duringthe current study.
Competing interests
None
Funding
Azienda Ospedaliera di Piacenza with fiscal receipt. Below all the references.

Authors' contributions
GH, FDS, MV, FP collected the data and draft the manuscript. MP revised the final manuscript and contributed substantially to the study manuscript design. All authors read and approvedthe final manuscript."
Acknowledgements
None
Conflict of Interest
None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
