
Case Report | DOI: https://doi.org/10.31579/2768-2757/095
General Cir Specialist, Vascular Cir, Endovascular and Phlebology; Phlebology Service - Hospital San Luis - San Luis – Argentina.
*Corresponding Author: ME Muñoz Surgeon, General Surgery Department, Ain Taya Hospital, 16029, Algiers, Algeria.
Citation: S. Ammari, N. Nait S, Y. Benhocine, N. Bounab, A. Bouzid, et al., (2023), Thoracic Aorta Artery - Endovascular Treatment, Journal of Clinical Surgery and Research, 4(6); DOI:10.31579/2768-2757/095
Copyright: © 2023, García Olaisa. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 November 2023 | Accepted: 16 November 2023 | Published: 24 November 2023
Keywords: blunt chest trauma; thoracic pseudoaneurysm; polytrauma; endovascular treatment
Trauma to the Thoracic Aorta is a common injury in patients with blunt chest trauma and polytrauma in general (1), its association with injuries in other territories adds significant morbidity and mortality. In those patients in whom this lesion is suspected, a Multislice Axial Tomography should be performed, with intravenous contrast (2). Its correct management and treatment constitute an emergency (3,4,5). Endovascular treatment is considered a valid option in these cases (6,7). Some lesions may be susceptible to conservative medical treatment (8,9).
Trauma to the Thoracic Aorta is a common injury in patients with blunt chest trauma and polytrauma in general (1), its association with injuries in other territories adds significant morbidity and mortality. In those patients in whom this lesion is suspected, a Multislice Axial Tomography should be performed, with intravenous contrast (2). Its correct management and treatment constitute an emergency (3,4,5). Endovascular treatment is considered a valid option in these cases (6,7). Some lesions may be susceptible to conservative medical treatment (8,9).
male, 21 years old. He is admitted after having suffered motorcycle vs. wall trauma. Hemodynamically stable, with dyspnea, chest pain, severe trauma to the right lower limb. Brain and Thoracoabdominal CT, and other pertinent studies, were requested. The diagnosis was: absence of acute lesions at the brain level, right hemopneumothorax, descending thoracic aortic artery pseudoaneurysm at the level of the isthmus,
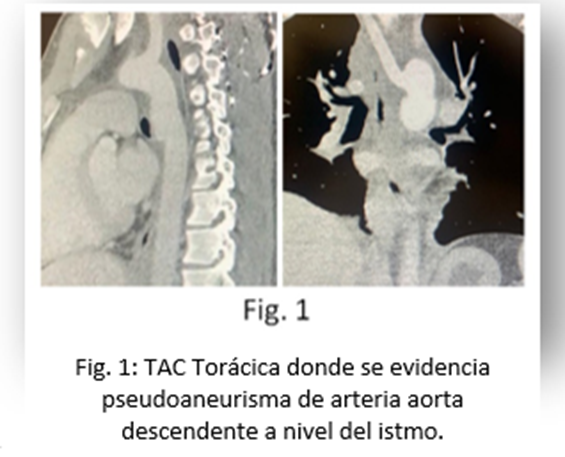
with aberrant right subclavian artery (Figure 1),
absence of injuries to intra-abdominal solid organs, right femur fracture. In the shock room he suffered from arterial hypotension, which was reversed with fluid replacement and low-dose vasoactive drugs. The femur fracture was stabilized, a right pleural drainage tube was placed, and urgent treatment of the aortic injury was indicated.
The same was resolved by placing 2 CP Stent Lined Stents. NuMed – Braum 24 mm diameter x 45 mm length: Platinum-Iridium Stent with ZIGS configuration, coated with PTFE Stent with good radial strength and
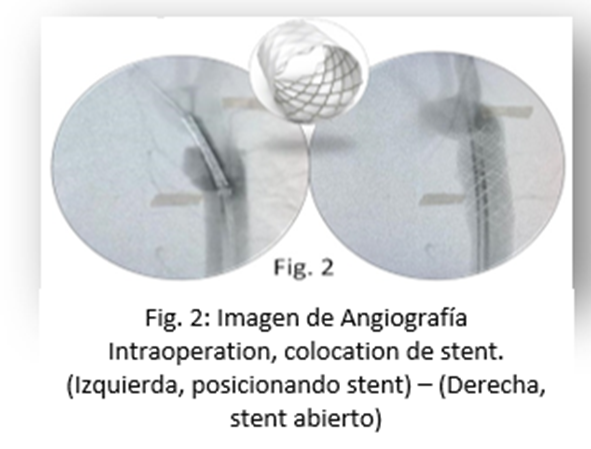
with the possibility of future re-expansion (Figure 2).
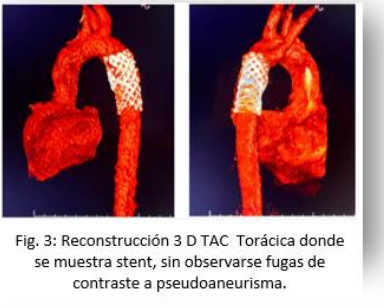
Post-surgical course in ICU with imaging control using AngioTAC at 48 hours (Figure 3),
where the correct positioning of the Stents is confirmed, without filling of the pseudoaneurysm sac or presence of leaks.
Conclusions: In our experience, we consider that in severe trauma, aortic injuries should be actively ruled out with a Thoracoabdominal CT on admission. Placement of an aortic stent should be done as soon as possible if a major vascular injury is detected.
We believe that the most important thing in this type of trauma is to make an early diagnosis in the face of strong clinical suspicion.
which will allow us to optimize the therapeutic options and times in each case, as well as carry out correct monitoring of the injuries.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
