
Research Article | DOI: https://doi.org/10.31579/2641-5194/003
Jangaon Institute of Pharmaceutical Sciences, Depot. Of Pharmaceutics, Jangaon, India.
*Corresponding Author: Vijay Kumar Bontha – Jangaon Institute of Pharmaceutical Sciences, Depot. Of Pharmaceutics, Jangaon, India.
Citation: Vijay Kumar Bontha. Theory of Additional Corpus Biopsy for Epidemiology and Diagnosis of Helicobacter Pylori. J. Gastroenterology Pancreatology and Hepatobilary Disorders. 1(1). doi. 10.31579/2641-5194/003
Copyright: © 2017 Vijay Kumar Bontha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2017 | Accepted: 22 December 2017 | Published: 26 December 2017
Keywords: gastric atrophy; sydney system; h. pylori; gastritis
Background: There is still debate on the best sites for biopsy- based tests of Helicobacter pylori infection in patients with gastritis. This study was designed to determine if it is important to add corpus biopsies to the routine antral ones for identification of H. pylori, especially in case of gastric atrophy and/or intestinal metaplasia.
Methods: A causative role is now accepted for Helicobacter (formerly Campylobacter) pylori in type B gastritis, and evidence is accumulating that H. pylori infection plays a major contributory role in peptic ulcer disease. Preliminary studies have reported that the prevalence of H pylori infection increases with age, but detailed information on the prevalence of the bacteria in any defined population and on the factors that may influence the pattern of distribution remains scanty.
Results: Up to 85% of people infected with H. pylori never experience symptoms or complications. Acute infection may appear as an acute gastritis with abdominal pain (stomach ache) or nausea. Where this develops into chronic gastritis, the symptoms, if present, are often those of nonulcer dyspepsia: stomach pains, nausea, bloating, belching, and sometimes vomiting or black stool.
Conclusion: H. pylori has been associated with colorectal polyps and colorectal cancer. It may also be associated with eye disease.
Helicobacter pylori affect nearly half of the population among the world. It is one of the most frequent and persistent bacterial infections worldwide [1]. It is responsible for many of the upper gastrointestinal tract diseases; chronic gastritis, gastrointestinal ulcers, Mucosa Associated Lymphoid Tissue Lymphoma (MALT) and gastric cancer as well [2]. Thus it has been known as "definitive biological carcinogen" by WHO in 1994 [3].
It is also linked to the development of duodenal ulcers and stomach cancer. However, over 80% of individuals infected with the bacterium are asymptomatic, and it may play an important role in the natural stomach ecology.[4]
Up to 85% of people infected with H. pylori never experience symptoms or complications.[5] Acute infection may appear as an acute gastritis with abdominal pain (stomach ache) or nausea.[3] Where this develops into chronic gastritis, the symptoms, if present, are often those of nonulcer dyspepsia: stomach pains, nausea, bloating, belching, and sometimes vomiting or black stool.[6][7]
Individuals infected with H. pylori have a 10 to 20% lifetime risk of developing peptic ulcers and a 1 to 2% risk of acquiring stomach cancer.[5][7] Inflammation of the pyloric antrum is more likely to lead to duodenal ulcers, while inflammation of the corpus (body of the stomach) is more likely to lead to gastric ulcers and gastric carcinoma. However, H. pylori possibly plays a role only in the first stage that leads to common chronic inflammation, but not in further stages leading to carcinogenesis.[4] A meta-analysis conducted in 2009 concluded the eradication of H. pylori reduces gastric cancer risk in previously infected individuals, suggesting the continued presence of H. pylori constitutes a relative risk factor of 65% for gastric cancers; in terms of absolute risk, the increase was from 1.1% to 1.7% This study was designed to determine if it is important to add corpus biopsies to the routine antral ones for identification of H. pylori, especially in case of gastric atrophy and/or intestinal metaplasia.
Methods and Materials
At least half the world's population is infected by the bacterium, making it the most widespread infection in the world. Actual infection rates vary from nation to nation; the developing world has much higher infection rates than the West (Western Europe, North America, Australasia), where rates are estimated to be around 25%.
The age when someone acquires this bacterium seems to influence the pathologic outcome of the infection. People infected at an early age are likely to develop more intense inflammation that may be followed by atrophic gastritis with a higher subsequent risk of gastric ulcer, gastric cancer, or both. Acquisition at an older age brings different gastric changes more likely to lead to duodenal ulcer.[5] Infections are usually acquired in early childhood in all countries. However, the infection rate of children in developing nations is higher than in industrialized nations, probably due to poor sanitary conditions, perhaps combined with lower antibiotics usage for unrelated pathologies. In developed nations, it is currently uncommon to find infected children, but the percentage of infected people increases with age, with about 50% infected for those over the age of 60 compared with around 10
Three hundred and twenty eight consecutive patients of uninvestigated dyspepsia, who underwent upper endoscopy were enrolled, (Mansura university hospital - Egypt, Benha University hospital - Egypt, Hafer Albatin Central Hospital, KSA) from June 2014 to December 2015. Patients who received antibiotic or proton pump inhibitor treatment one month before hand were excluded. All procedures in the study were performed in accordance with the institutional research board (IRB) committee in our institute.
All patients underwent upper gastrointestinal endoscopy and two standard gastric biopsies were taken from both antrum (2-3 cm from the pylorus both lesser and greater curvature) and corpus (8-10 cm from the cardia both lesser and greater curvature) for the histological examination [15].
Histological Examination
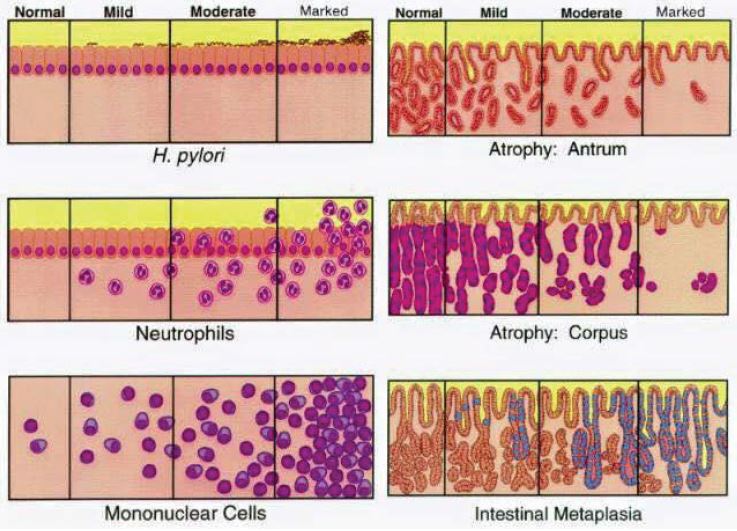
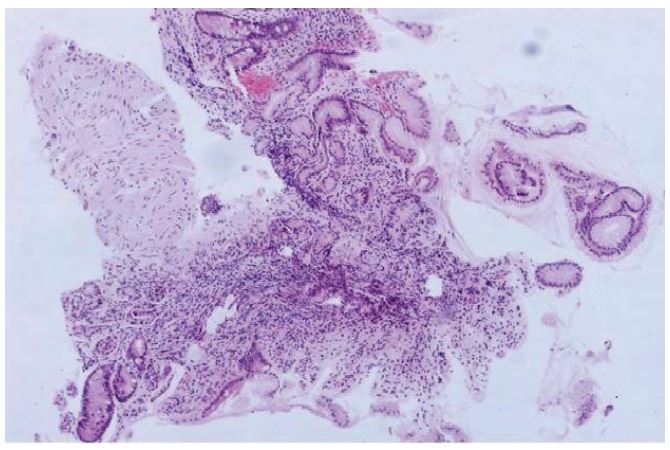
Endoscopic biopsies were processed as formalin fixed paraffin embedded tissues, cut into 3 μm thick sections, and then stained with H&E and modified Giemsa stain. These were scored semi-quantitatively according to the updated Sydney classification [15] (Figure 1). The following features were evaluated on each slide, inflammatory activity, glandular atrophy and intestinal metaplasia. According to these histological criteria, there were four grades of atrophy; 0- none; 1- mild; 2- moderate and 3- severe.
Criteria for positivity and negativity of H. pylori were set: Patients were defined positive for H. pylori if either one or both was positive with Giemsa stained slides. Patients were considered negative if all specimens were negative. The histological evidence of atrophy was identified when the gastric glands were found decreased in amount and/or widely separated [16]
Results
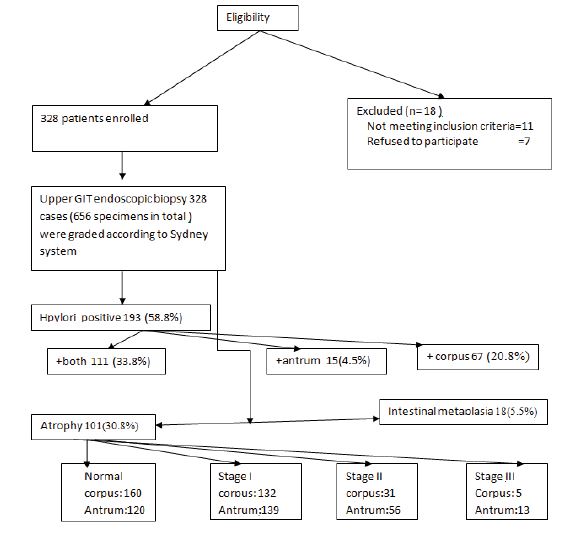
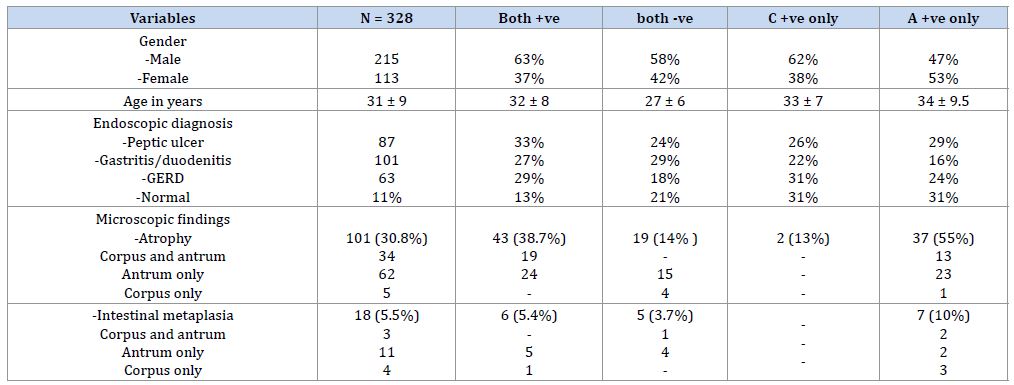
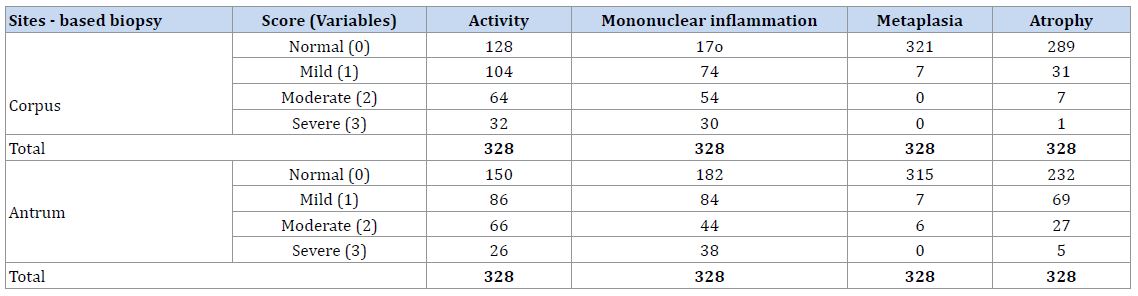
Figure 3 shows the flow chart for the whole study population. A total of 328 consecutive patients underwent an upper endoscopy procedure during the study period. The mean age of our patients was 39 ± 12 years; 145 (44.3%) were men. Upper gastrointestinal endoscopy was indicated for functional dyspepsia in 113 (34.5%), epigastric pain in118 (35.9%) or heart burn in 97 (29.6%) patients. Endoscopic diagnosis was peptic ulcer disease in 52 (15.9%), gastritis or duodenitis in 173 (52.7%), or reflux esophagitis in 103 (31.4%) patients. None of our patients were diagnosed with gastric carcinoma. Regardless of the biopsy site, a total of 656 biopsy specimens were received for histological evaluation (Table 1).
In endoscopic diagnosis, atrophy was found in 101 (30.8%) of our patients. Atrophic gastritis was significantly more often in the antrum than the corpus (29.2 vs 11.9%, respectively, p < 0>). Intestinal metaplasia was identified in 17 (5.2%) patients and antrum was more often than the corpus (4 vs 2% of all patients, respectively). Patients with only positive corpus biopsies showed more incidences of both atrophy and intestinal metaplasia compared with the other possible outcomes, 55 vs 24.5% for atrophy and 10 vs 4.6% for metaplasia (Table 1, 2).
In the clinical setting, it is desirable to find a rapid and cost-effective method for detection of H. pylori. There are many methods for detection of H. pylori infection [17]. Endoscopic mucosal biopsy and histopathology are considered as valuable diagnostic tools for H. pylori detection. As well as, it provides a proper evaluation of gastric mucosal changes that have been attributed to chronic H. pylori infection i.e. glandular atrophy and/or intestinal metaplasia. It is still widely used as a main diagnostic method in suspicious patients with upper gastrointestinal symptoms or in highly prevalent areas [7]. We reported in our study that 193 (58.8%) have been detected to have H. pylori, 111 (38.8%) patients, both antral and corpus biopsies were identified positive for H. pylori. Totally 30.8% of our patients had atrophy in the antrum and/or corpus or both. Intestinal metaplasia was identified in 17 (5.2%) patients.
There is always a debate about the best location of gastric mucosal biopsy that can yield more sensitive detection of H. pylori especially in presence of atrophic gastritis [18]. In our work; we found that the frequency of H. pylori detection in case of gastritis without atrophy or metaplasia was higher with additional corpus biopsy compared with only antrum-based biopsy.
H. pylori associated atrophic gastritis decreases sensitivity of detection rates of H. pylori. Atrophic changes are predominantly affect antrum first. Adding corpus biopsy to the routine antrum biopsy during endoscopy is recommended for proper evaluation of H. pylori infection case of gastric atrophy and to avoid false negative diagnosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
