
Research Article | DOI: https://doi.org/10.31579/2641-0419/559
*Corresponding Author: William E. Feeman, Principal Investigator, The Bowling Green Study, USA
Citation: William E. Feeman, (2026), The (Virtual) Elimination of Atherothrombotic Disease, J Clinical Cardiology and Cardiovascular Interventions, 9(5); DOI:10.31579/2641-0419/559
Copyright: © 2026, William E. Feeman. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 March 2026 | Accepted: 24 March 2026 | Published: 06 April 2026
Keywords: maxillofacial injuries; mandibular fractures; road traffic accidents; panfacial trauma
Background
Atherothrombotic Disease (ATD) is the most common cause of morbidity and mortality in the western world. Many attempts have been made to attempt to predict the population at risk of ATD, with the aim of treating at-risk patients and thereby in theory preventing the onset of clinical ATD. The current predictive tools either do not predict well, or they predict well in the short term, but not in the long term. The purpose of this paper is to present a means of ATD risk prediction based on the risk factor profile of patients who developed some form of clinical ATD during the Bowling Green Study (BGS) time frame of 4 November 1974 to 1 January 2023. This approach will treat the various risk factors as interdependent factors as advocated by the Framingham Heart Study.
Methods and Materials
The findings in this paper are based on a chart review of all patients known by the author to have developed some form of clinical ATD in the BGS timeframe. The risk factors to be examined are cigarette smoking, dyslipidemia, and hypertension. (Other risk factor data is available but not needed to define the populations at risk of ATD.) The BGS involves patient of both genders and all ages.
Full risk factor data is available for 907 BGS patients, with an additional 47 patients whose lipids were treated prior to entry to the BGS. The lipid data is comprised of low-density lipoprotein cholesterol (LDL-c) and high-density lipoprotein cholesterol (HDL-c), combined together in a ratio. Cigarette smoking status is determined by direct questioning. Blood pressure is determined by trained office staff.
Results
Examination of the BGS database reveals that ATD risk factors are rarely present as single entities in patients with ATD. The BGS predictive tool is therefore a graph with the Cholesterol Retention Fraction (CRF, defined as [LDL-c minus HDL-c]/LDL-c) on the ordinant and systolic blood pressure (SBP) on the abscissa. The BGS has developed a threshold line with CRF-SBP co-ordinates of (0.74, 100) and (0.49, 140). A CRF-SBP plot above this threshold line provides a first order approximation of ATD risk. This graph may in turn be subdivided into quadrants with a horizontal line at CRF = 0.70 and a vertical line at SBP = 140. Using this approach one can include patients whose lipids and/or SBP have been treated. The average age of ATD onset of the patients in the various quadrants can then be calculated to determine a second order approximation of ATD risk. A third order of ATD risk cn be gained by subdividing the BGS graph into sextiles of CRF versus SBP. The lower the average age of ATD onset, the higher the near-term risk of ATD.
Reverting back to the general population, one can create a table of all of the CRF data, stratified by age and gender, and stratified by presence/absence of clinical ATD. One can then generate revere Kaplan-Meier curves (time to event) to determine when to begin treatment, depending upon the ATD risk level one wishes to accept prior to initiating therapy. In the general population, serial lipid testing can inform the treating physician of any changes in ATD risk based on changes from baseline values.
Finally, the author has in his physical possession the databases of eight angiographic regression trials. Examining the end-of-trial lipids in terms of angiographic outcome aids in determining the amount of lipid lowering that must be obtained to maximize plaque stabilization/regression.
Conclusions
The population at risk of ATD can be readily identified on the basis of the data in the BGS. Early and repeated lipid testing, combined with cessation of cigarette smoking (most important) and control of SBP offers the opportunity to prevent ATD, at least until very late in life.
Atherothrombotic Disease (ATD) is the leading cause of morbidity and mortality in the western world. (1,2). ATD refers to atherosclerotic disease, with emphasis on the thrombosis that so often causes the acute clinical event, such as acute myocardial infarction or acute cerebral infarction. Based on the concept of “An ounce of prevention is worth a pound of cure,” and over 50 years of personal experience in the field of preventive cardiology and interventional lipidology (Harvey Hecht, MD, used with permission), it is this author’s opinion the best means of preventing ATD is the determination of who is at risk of early and middle-aged ATD. It is the common experience of this author and others, there is “no safe place” to totally prevent ATD. In other words, if one lives long enough and does not die of something else, he/she will eventually experience an ATD event. Thus the goal should be to identify those people at risk of ATD in the early and middle-aged years of life, treating them to prevent plaque formation, and to identify older at-risk patients (aged 75 years or older), treating them in the hope of delaying their ATD events till very late in the lifespan.
Unless the physician wishes to treat everyone (herd approach), the author accepts as true that a physician can not protect his/her patient unless that physician can predict which patients are at risk of ATD and moreover, that the better that a physician can predict the population at risk of ATD, the better he/she can protect that patient from ATD. Such an attempt requires accurate tools with which to make the prediction, but it also requires that testing be done early in life and be repeated at intervals to determine if the prediction has changed over time. This has been referred to as primordial prevention. (3)
Prediction of the population at risk of ATD has been attempted by various groups over the last 50+ years, beginning with the Framingham Heart Study (FHS). The FHS has published numerous papers on this topic and has identified three main ATD risk factors (cigarette smoking, dyslipidemia, and hypertension) with some contribution by the very high blood sugar levels of uncontrolled diabetes. (4-8). The FHS has specifically created a Framingham Risk Score (FRS) to predict those patients at risk of ATD. (9) In the FHS, the lipid predictor that best predicts risk is total cholesterol (CT) divided by high-density lipoprotein cholesterol (HDL-c) (10-11); however in the FRS, because of the promise of greater statistical power, the CT:HDL-c ratio has been discarded and CT and HDL-c are utilized as independent factors. (Peter Wilson, MD, personal communication). Other studies have built on the FHS findings, specifically the Atherosclerosis Risk in the Community and the Multi-Ethnic Study of Atherosclerosis, and some other studies have attempted to predict the population at risk of ATD. These latter predictors include the Pooled Cohort Equations (PCE) (12), SCORE2 (13), QRISK (14), Interheart (15), and the Sheffield Tables (16). Most recently, the American Heart Association has introduced the Predicting Risk of cardiovascular disease EVENTs (PREVENT) (17) to try to improve ATD risk prediction. There are many other predictors, but they are not used in the daily practice of medicine. Of the cited studies, the FRS, PCE, and PREVENT use CT and HDL-c as their lipid predictors and as independent risk factors. QRISK and the Sheffield Tables use the CT:HDL-c ratio as their lipid predictors. SCORE2 uses (CT minus HDL-c, termed non-HDL-c cholesterol) and Interheart uses a ratio between lipoproteins apo B and apo A-1).
Reports have been published concerning ATD events in patients without the standard ATD risk factors. (18-20) And of course, in 2017, the president of the American Heart Association sustained an acute myocardial infarction while delivering lecture at the annual scientific assembly. Concurrently, recent studies have shown that the above noted predictors are indeed faulty. Sud found that neither the FRS nor the PCE predicted ATD events very well over the long term, though they were fairly accurate very the short term.(21) Saleh has suggested that coronary artery calcium scoring be added to the PCE to improve its predictive ability. (22) And finally Nurmohamed has proposed adding coronary artery CAT scans to the predictive tool, again to enhance its accuracy. (23) The problem with these latter two approaches that they identify people who already have disease, perhaps even significant ATD.
In light of the above, there is a need to enhance the prediction of the population at risk of ATD. It will be the purpose of this paper to present a novel predictive tool, based almost entirely on the precepts of the FHS and to present a program based on this risk assessment that may well lead to the prevention of clinical ATD, at least until very late in life.
The Bowling Green Study (BGS) of the Primary and Secondary Prevention of Atherothrombotic Disease was conceived in 1968 while the author was in medical school at Ohio State University and doing a cardiology rotation. This provided the initial background for the BGS and the first tentative steps in the investigation that led to the BGS predictive tool were undertaken while the author served on active duty in the United States Air Force (1971-1974) at RAF Lakenheath Hospital in England. The major input to the BGS began in November of 1974 when the author set up his practice of family medicine in Bowling Green, the county seat of Wood County in northwest Ohio. The major portion of Wood County is rural in nature, the population of Wood County at the last census was 132,248 people, the vast majority being of northern European descent. The chief minority is people of Latin American descent. The population of Bowling Green at last census was 28,500, with 66?ing students at Bowling Green State University, which is the chief employer in Wood County. Multiple small industries exist.
When the author set his practice in 1974, he provided medical care for people of both genders and of all ages, thus giving him a typical patient cohort for Wood County. The author’s main purpose, besides providing good medical care for his patients, was to attempt to predict the population at risk of ATD. In this he followed the precepts of the FHS. The effort to collect enough data to make such a prediction was not a randomized controlled clinical trial. There were no placebo groups. Everyone who met the available criteria for lipid management, according to the FHS, was offered treatment. Some accepted therapy, but many did not. In the mid-1970’s, the existing medical community was not interested in preventive medicine, as least as regards dyslipidemia, and even treatment for hypertension was not universal. Cigarette smoking was widespread, at least in the author’s male patients. Additionally, in the mid-1970’s, the medications used to treat either dyslipidemia or hypertension (or diabetes, for that matter) were not very efficacious. AS a result, many of the author’s patients sustained ATD events. Meanwhile, the author continued to collect ATD risk factor data.
ATD risk factor data collected consisted initially of the patient’s blood pressure and height/weight (converted into Body Mass Index). This was collected on each and every patient presenting to the author’s office. At times, the author was also able to collect fasting lipid data: CT and triglycerides (TG) until 1 January 1978, when HDL-c data became available and was incorporated into the lipid panel, along with a calculation of the low-density lipoprotein cholesterol (LDL-c) following the Friedewald formula. The Friedewald formula is as follows: LDL-c = CT minus HDL-c minus TG/5. (24) HDL-c was measured by the precipitation method. The measurement of a lipid panel was done on the basis of family history of dyslipidemia and/or ATD, and a personal history of dyslipidemia and/or ATD, as well as the presence of any known ATD risk factors such as hypertension or diabetes—and indeed for any reason at all. Moreover, a determination of blood glucose performed precisely two hours after a 100 gm carbohydrate meal as suggested by the Wood County Hospital dietician at the author’s request. (A copy of the protocol is presented in the Appendix I.) Finally, in the summer of 1981, when the author recognized the paramount importance of cigarette in the pathogenesis of ATD, the author began actively accumulating tobacco use data for everyone presenting to his office aged 15 years or older. And after reading surveys in 1991 that cigarette smoking was occurring in adolescents aged 10-14 years, smoking surveys were done on everyone aged 10 years or older.
All of this data was collected into a general population (Gen Pop) database. As noted previously, ATD risk factor analysis, at the time of the BGS initiation, was not precise and medications to treat dyslipidemia, hypertension, and diabetes were not very efficacious. Moreover, cigarette smoking was rampart in Wood County and many people did not wish to pursue a course of preventive medications. Additionally, the author received no support from the established medical community. Likely as a result, many of the author’s patients developed some form of clinical ATD. By 1981, the author was able to separate out those people who had developed some form of clinical ATD from the Gen Pop and place them into an ATD data base (ATD Pop).
Inspection of the ATD Pop database revealed that while interpreting cigarette smoking, blood pressure and blood sugar data was straight forward, the interpretation of the lipid data was less clear. Some people developed ATD with high levels of LDL-c, but others did so with low levels of LDL-c. Moreover, some people with low levels of HDL-c developed ATD, but others did so with high levels of HDL-c. But then in 1981 and article was published asking the question: ”Is the LDL:HDL Ratio the Best Lipid Predictor.” (The author regrets that this article is lost to him and hence he can not give proper attribution.) The author subsequently inspected the ATD Pop database and found that when people with low levels of LDL-c developed ATD, their associated HDL-c tended to be very low. Furthermore, when people with high HDL-c levels developed ATD, their associated LDL-c tended to be very high. When these were not the cases, the younger patients were virtually always cigarette smokers, whereas older ATD patients usually had hypertension with/without diabetes. Consequently, in 1981, the BGS began to use the LDL-c:HDL-c ratio as its preferred lipid predictor.
In 1983, it occurred to the author that what he really wanted to know was the amount of cholesterol accumulating within the artery wall. This, he reasoned, was best estimated by the amount of cholesterol entering the artery wall (LDL-c) minus the amount of cholesterol exiting the artery wall via reverse cholesterol transport (HDL-c), that difference being divided by LDL-c, to give an estimate of the percentage of the LDL-c being retained within the arterial wall. This fraction the author termed the Cholesterol Retention Fraction (CRF, defined as [LDL-c minus HDL-c]/LDL-c). The CRF is abnormal at 0.70 or higher.
After a conversation with Roger Illingworth, MD, in the early 1980’s, in which Illingworth pointed out that reverse cholesterol transport could not compensate for very large influxes of LDL-c, the author returned to the ATD Pop database and noted that once LDL-c exceeded 169 mg/dl (4.4 mmoles/L), ATD events could occur despite an optimal level of CRF, although the lower the CRF, the later in life did the ATD event occur. The author therefore considers a state of dyslipidemia to exist whenever the CRF is 0.70 or higher and/or LDL-c is 170 mg/dl (4.4 mmoles/L) or higher. This scenario is termed the Cholesterol Threshold (CThr).
Caveat
All scientific hypotheses must be based on factual observations. The observations so far discussed and those yet to come were all based on the measurement of HDL-c and calculation of LDL-c by the Friedewald formula, as described earlier in this paper. Until the spring of 1999, HDL-c was measured by the precipitation method (Precip) in which fasting serum is infused with either heparin manganese or phosphotungstic acid, both of which precipitate out all of the lipoproteins except HDL. (Other precipitants have been used. Different methodologies give differing HDL-c measurements, though not usually much different.) In the spring of 1999, at least in the author’s area of practice, the methodology of HDL-c measurement was changed to the enzymatic method (Enz),with no advanced warning to the medical community. These two differing methodologies (Precip versus Enz) give differing results, but this time on the order of 10 mg/dl (0.25 mmoles/L). The Enz method gives the higher value and the Precip method gives the lower value. Consequently, the LDL-c level calculated by the Friedewald formula will be on the order of 10 mg/dl (0.25 mmoles/L) lower for the Enz method than for the Precip method. A lipid ratio, such as used in the BGS, will, as a result, be significantly altered, dependent upon the methodology by which HDL-c is measured.
This is finding is not inconsequential. In 2008, the author reported the case of one of his patients who sustained an acute myocardial infarction at age 53 years. (25) The author had provided medical care for him over the years, almost always relating to employment issues. Neither the patient nor his wife had ever smoked cigarettes. He was not hypertensive or known to be diabetic. He was slim, not obese. He had no personal or family history of dyslipidemia, diabetes, or ATD. Hence the author had never tested his lipids. One day in 2008, the patient sustained an acute myocardial infarction while in Toledo, Ohio. He went to a local hospital to which he was admitted. A lipid panel was performed on admission and was mildly abnormal. The Enz method of HDL-c measurement was utilized at that hospital. When he returned to the author’s care, the author was able to obtain a copy of the lipid panel results. Using the formula provided by Wood County Hospital, the lipid panel was converted from the Enz methodology to its Precip equivalent and now the lipid panel was much more abnormal--especially the CRF—and the patient sustained his myocardial infarction when it would have been predicted by the Precip method. The formula for conversion of Enz HDL-c to Pecip HDL-c (using the auto-analyzer at Wood County Hospital) is as follows: HDL-c (Precip) = [HDL-c (Enz) minus 12]/0.93.
Since the vast majority of the author’s lipid panels utilized the Precip methodology and since the angiographic regression studies, to be discussed later in this paper, were performed using the Precip methodology, the author has elected to continue using the Precip data, converting the Enz based lipids to their Precip based equivalents. The Precip based lipid equivalents can be roughly approximated by subtracting 10 mg/dl (0.25 mmoles/L) from HDL-c (Enz), adding 10 mg/dl (0.25 mmoles/L) to LDL-c (Enz), and subtracting 0.1 from the CRF.
As noted previously, the author inspected his ATD database in the late 1970’s and early 1980’s, once enough patients had sustained enough ATD events. (See previous comments about the suboptimal risk predictors and medications to control the various risk factors—and the distinct lack of interest in preventive cardiology and interventional lipidology.) It was at this point that the paramount importance of cigarette smoking became obvious—until that time cigarette smoking was just another ATD risk factor. Almost as important as that finding was the observation that the various ATD risk factors rarely acted alone. The various ATD risk factors virtually always acted in concert with one another. Therefore the author began to look for various risk factor combinations that might be predictive of ATD. Various risk factor combinations were examined, but the only combination that proved predictive was the LDL-c : HDL-c ratio paired with systolic blood pressure (SBP)—and then only when stratified by cigarette smoking. The author, a few years later, replaced the LDL-c : HDL-c ratio with the CRF, due to the latter’s somewhat better predictive ability. (Feeman, unpublished data) (See Figure I.) The initial CRF-SBP plots amounted to a scattergram, but once the CRF-SBP plots were stratified by cigarette smoking, a clear band of those plots was present at CRF levels at or above 0.70. There were a few outliers, representing elderly patients with isolated hypertension, but by far and away the CRF-SBP plots of ATD patients lay at or above the CRF=0.70 threshold. The author terms this main group the “main sequence.”
In light of this, in 1989 (when enough patients had sustained ATD events) the author elected to draw a sloping line of demarcation, based on the principle of the fewest false negatives. (In other words, if the author told the patient that his ATD risk was low, the author did not want to have given false reassurance.) The co-ordinates of this line are CRF-SBP plots (0.79, 100) and (0.54, 140). This line was termed the Atherosclerotic Disease Threshold Line. In the last decade of the twentieth century, the author contacted the principle investigators of eight angiographic regression trials and asked for copies of their databases. Actually, more than eight principal investigators were contacted, but only eight responded in the affirmative. In any event, the end of trial average CRF-SBP plot of one of those trials (the Lipoprotein and Coronary Atherosclerosis Study, or LCAS) lay just below the threshold line. LCAS was a secondary prevention trial. (26) The author then began to consider that since most of the patients in his practice had never had a lipid panel tested, those with an elevated C Thr threshold might well have subclinical atherosclerosis and therefore might be better served by lowering the threshold line to (0.74,100) and (0.49/140). These new co-ordinates, in the year 2000, created a new threshold line, now termed the angiographic stabilization/regression line (ASRL). (27) The threshold line co-ordinates have not been changed since that time. This graph, and its ASRL, are now termed the BGS Graph. (See Figure I.)
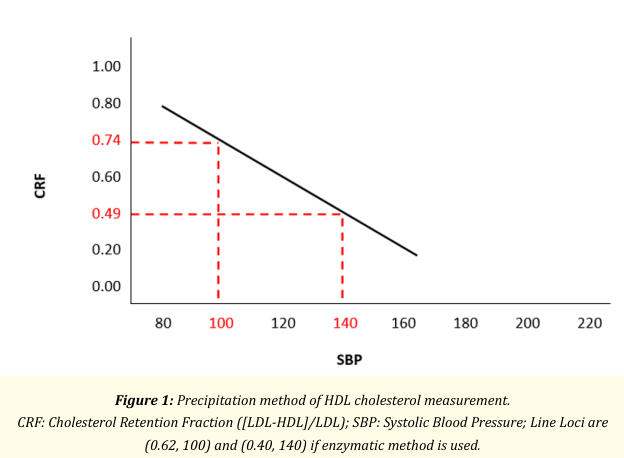
Table I gives the outcomes of BGS ATD patients from 1978 till the end of 2003. At the end of 2003 major insurance changes caused the author to lose about 25% of his patients, who were taken over by Wood County Hospital. As a result the author was unable to determine the outcomes of the “lost” patients, especially those who developed multi-system ATD (coronary, cerebral arteries, and peripheral arteries, in various combinations ). The BGS Graph (1978-2003) does give outcomes data and reveals that people who smoke cigarettes and have a CRF-SBP plot above the ASRL have the youngest age of ATD onset, age at multi-system disease and age at death. Those with CRF-SBP plots below the ASRL and who have never smoked cigarettes have the oldest ages. Indeed the average age of ATD onset in these latter patients is so old that this plot position, in people who have never smoked cigarettes, implies virtual immunity to ATD. The results for those who smoked cigarettes in the past are not far behind. Incidentally the average age of ATD onset is earlier for those people whose CRF-SBP plot lies below the ASRL but who smoke cigarettes than that of people who have a CRF-SBP plot above the ASRL but who never smoked cigarettes. This finding illustrates the prime importance of cigarette smoking. Table II gives the CRF-SBP plot position for the (1978-2003) ATD patients and those added to the BGS after 2003, with respect to the average age of ATD onset. The findings are similar to those of Table.
| Above ASR Line | Below ASR Line | |||||||
| Sex | Average Age of | + | Past | - | + | Past | - | |
| Male | ||||||||
| ATD Onset | Total Patients | 126 | 130 | 86 | 20 | 14 | 8 | |
| Total Patient Years | 6659 | 8536 | 5913 | 1174 | 1041 | 623 | ||
| Ave. Age of ATD Onset | 53 | 66 | 69 | 59 | 74 | 78 | ||
| MSD Onset | Total Patients | 38 | 41 | 32 | 6 | 5 | 1 | |
| Total Patient Years | 2363 | 2983 | 2522 | 382 | 402 | 78 | ||
| Ave. Age of MSD Onset | 62 | 73 | 79 | 64 | 80 | 78 | ||
| Death Onset | Total Patients | 49 | 64 | 47 | 12 | 11 | 4 | |
| Total Patient Years | 3153 | 4780 | 3805 | 815 | 879 | 374 | ||
| Ave. Age of Death Onset | 64 | 75 | 81 | 68 | 80 | 94 | ||
| Female | ||||||||
| ATD Onset | Total Patients | 65 | 56 | 137 | 18 | 15 | 34 | |
| Total Patient Years | 3852 | 3908 | 9955 | 1145 | 1003 | 2543 | ||
| Ave. Age of ATD Onset | 59 | 70 | 73 | 64 | 67 | 75 | ||
| MSD Onset | Total Patients | 22 | 24 | 49 | 6 | 7 | 16 | |
| Total Patient Years | 1534 | 1800 | 3931 | 440 | 532 | 1283 | ||
| Ave. Age of MSD Onset | 70 | 75 | 80 | 73 | 76 | 80 | ||
| ATD Onset | Total Patients | 26 | 23 | 79 | 9 | 7 | 23 | |
| Total Patient Years | 1830 | 1824 | 6542 | 650 | 533 | 1941 | ||
| Ave. Age of Death Onset | 70 | 79 | 83 | 72 | 76 | 84 | ||
Table I
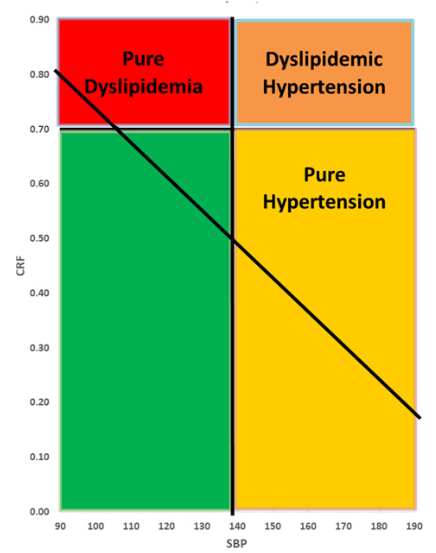
Simply using the BGS graph with its ASRL provides a rough estimate of ATD risk. A CRF-SBP plot below the ASRL, in the absence of any history of cigarette smoking, has such low risk of ATD that this scenario implies virtual immunity to ATD, at least until very old age. A CRF-SBP plot above the ASRL implies significant ATD risk. To enhance ATD risk prediction, the author has placed two lines of demarcation on the BGS Graph. The horizontal line was placed at CRF = 0.70 and the vertical line at SBP = 140 mm Hg. This divides the graph into quadrants. The left upper quadrant (zone I)represents those with pure dyslipidemia; the right upper quadrant (zone II), those with dyslipidemia and hypertension; the right lower quadrant (zone III), those with pure hypertension; and the left lower quadrant, those with neither dyslipidemia nor hypertension (zone IV). (See Figure II.) Tables III A-C give the average ages of ATD onset in each of the areas in Figure II. Table III-A gives the average age of ATD onset for all patients while Table III-B shows the same data, but for males, and Table III-C shows the data for females. The data in these tables is stratified by cigarette smoking status. Patients with CRF-SBP plots in the let upper quadrant are said to be in Zone I, with patients having CRF-SBP plots lying in the area above the ASRL being in Zone I-A and those below the ASRL being in Zone I-B. The right upper quadrant is termed Zone II, and all CRF-SBP plots in Zone II are above the ASRL. The right lower quadrant is termed Zone III, with patients above the
ASRL being in Zone III-A and those below the ASRL being in Zone III-B. The left lower quadrant is termed Zone IV, with the area lying above the ASRL being termed Zone IV-A and the area below the ASRL being termed Zone IV-B. Each of these zones can be subdivided by cigarette smoking status. Table III-A contains the data for the one patient with full lipid and blood pressure data, but whose cigarette smoking status is not known. Tables A-C can be color coded for the average age of ATD onset. Those patients who presented to the BGS with ATD events occurring younger than 64 years of age and younger are placed in the red zone; those with presenting ages of 65-74 years, in the yellow zone; and those with presenting ages of 75 years or older, in the green zone. It will be clear that red zone patients lie mainly in the current smokers category, whereas green zone patients lie mainly in the never smokers category. (The never smokers category does include people who have never smoked cigarettes, but may have smoked pipes or cigars, or may have chewed tobacco.) Zone I-A had the youngest ATD patients (average age of ATD onset at 59 years) and adding in Zone I-B does not much change the average age of ATD onset (60 years). Zone II patients are second in the age category (average age of 65 years). Zone III-A patients are older still (average of 69 years) and Zone III-B are even older (average age of 71 years). The data for Zone IV-A and IV-B follows a similar pattern.
In Table III-A, virtually all of the “red zone” patients are found in current cigarette smoking cohorts and “red zone” ex-smokers/never smokers mainly in Zones I-A and I-B. Conversely all of the “green zone” patients fall into the never smoker category. Patients in Zone II have their ATD events on the average of 6 years later than do Zones I-A and I-B. Zone III patients lie mostly (78% of patients) in Zone III-A and have their ATD events a few years earlier than do Zone III-B patients. Tables III-B and III-C reveal that males and females have similar patterns.
The advantage of this approach is that it better defines ATD risk in terms of lipids and blood pressure. The left lower quadrant can contain those with CThr and/or treated hypertension. Using this approach, those patients with an abnormal CThr can now be moved to the left upper quadrant if the SBP is below 140 mmHg or to the right upper quadrant if SBP is elevated, and treated dyslipidemic patients can be added to either the left upper quadrant or the right upper quadrant, again depending on blood pressure. Those with treated hypertension, but no dyslipidemia (treated or not) can be shifted from the left lower quadrant to the right lower quadrant. This permits better definition of ATD risk and it examines that risk in terms of risk factors combinations and now analyzes the data of 954 patients instead of 907 patients. However, this modification makes little difference to the average age of ATD onset.
There is still a large differential in ATD risk in the various subdivisions noted above. This can be further investigated by eliminating the ASRL and dividing the CRF and the SBP into sextiles and then determining the average age of ATD onset for each CRF-SBP cohort. Doing this means that the CThr patients and those on lipid modifying therapy must of necessity be excluded from the analysis. Determining the CRF-SBP cohorts for the 906 patients for whom the CRF, SBP and cigarettes smoking data is known—excluding the one patient with CRF and SBP data, but no cigarette smoking data—means that there are 36 cohorts to match with the BGS ATD patients. (See Tables IV A-D.)
Tables IV A-D give the distribution of the various CRF-SBP cohorts in the BGS ATD population for those patients who were not receiving medications for either hypertension or dyslipidemia at their presentation to the BGS. This encompasses 79% (716/907) of the BGS ATD population for whom full lipid data is available. With the loss of 21% of the BGS ATD database, stratifying the CRF-SBP cohorts by cigarette smoking status is problematical due to fewer patient numbers. To reiterate, the red zone includes all of the patients whose average age of ATD onset is 64 years or earlier. The yellow zone includes all of the patients whose average age of ATD onset is between 65 and 74 years of age. Finally, the green zone is comprised all of the patients whose average age of ATD onset is 75 years or older. (This is equivalent to early onset ATD, middle-aged onset of ATD, and old age onset of ATD.) Men and women are grouped together in these Tables. Inspection of Table IV-A reveals that 75% (316/422) of the red zone patients lie in the CRF= 0.70 or higher portion of the Table, whereas 22% (62/277) of the yellow zone patients occupy this area (CRF = 0.70 or higher) and green zone patients are absent from this area. In the area occupied by those with CRF values of 0.60-0.69 lie the CRF-SBP cohorts of most of the other red zone patients (14%, or 57/422) and the CRF-SBP cohorts of yellow zone patients (38%, or 104/277). But again no green zone patients are present. Finally in the area occupied by patients with CRF values of 0.59 or less, lie the CRF-SBP plots of the remaining red zone patients (12%, or 49/422) and yellow zone patients (43%, or 111/277). All green zone patients have CRF-SBP plots in this area. The author interprets all of this to mean that the risk of early onset ATD is mainly limited to people with a CRF of 0.70 or higher. However, Table IV-A takes into account all comers who are not taking anti-hypertensive/dyslipidemic medications and is not stratified by cigarette smoking status.
Table IV-B provides the same analysis, but limited to current cigarette smokers. It will be clear that 99% (267/269) of patients are associated with red zone risk, regardless of CRF-SBP cohort status. There is one yellow zone patient (in the CRF = 0.65-0.69 section) and one green zone patient (in the CRF= 0.60-0.64 section).
Table IV-C provides the same analysis for people who have quit smoking cigarettes for at least 6 months and have not resumed smoking. 91% (43/47) of red zone patients have CRF values of 0.70 or higher, as do 43% (63/146) of yellow zone patients and 29% (4/14) of green zone patients. Of the patients with CRF values of 0.60-0.69, 9% (4/47) of red zone CRF-SBP have cohorts in this area, as do 21% (30/146) yellow zone patients and 71% (10/14) green zone patients. Finally the area of Table IV-C for patients with CRF values of 0.59 or less contains no red or green zone patients, but does contain the cohorts of 36% (53/146) yellow zone patients. It will be clear that once current cigarette smokers are removed from consideration, there is a marked shift away from red zone (early onset) age at ATD onset, favoring yellow and green zones.
Table IV-D gives the data for patients who have never smoked cigarettes, though they may have smoked cigars or pipes or chewed tobacco. For patients who have CRF values of 0.70 or higher, red zone patients congregate in this area of the Table with 78% (28/36) being located there, as are yellow zone patients ( 48% or 71/147) and 38% ( 21/56 )green zone patients. For those with CRF values of 0.60-0.69, 22% (8/36) of red zone patients have CRF-SBP cohorts in this area, as compared to 15% (22/147) yellow zone patients and 43% (24/56) green zone patients. For those patients with CRF values of 0.59 or less, no red zone patients are present, whereas 37% (54/147) of yellow zone patients and 20% (11/56) of green zone patients are present.
In summary, Tables IV B-D reveal the marked shift away from early onset ATD as one moves from current to past to never cigarette smoking. Moreover, most of the red zone (early onset ATD) patients lie in the CRF of 0.70 or higher area. Additionally, as the CRF falls, the average age of ATD onset appears to grow older.
Once the average age of ATD onset for a patient’s CRF-SBP cohort is determined, the next question to be asked is when treatment of a lipid disorder should be commenced. The answer to this question is that it depends upon what risk of ATD one is willing to run before beginning treatment. This author has privately contacted a number of his collegues, none of whom would go on the record on this matter. One, speaking on the condition of anonymity, suggested that a lifetime risk of 15% would be a suitable threshold for initiating treatment. Recent investigations of ATD risk have indicated fault with current guidelines, with the main fault being with long term projections. (21-23) Hence this author decided to utilize that recommendation as it came from an internationally known investigator and this author’s data fits better with lifetime ATD risk.
The topic of when to begin dyslipidemic therapy can be initiated by revisiting the Gen Pop and creating a table with all of the CRF determinations, stratified by age and gender—and then by the presence/absence of ATD patients in each of the cohorts thus created. (See Tables V A-C.) The ATD risk in each cohort is determined by the number of ATD events and number of patients within each cohort. Table V-A is comprised of all-comers; Table V-B, for males; and Table V-C, for females.
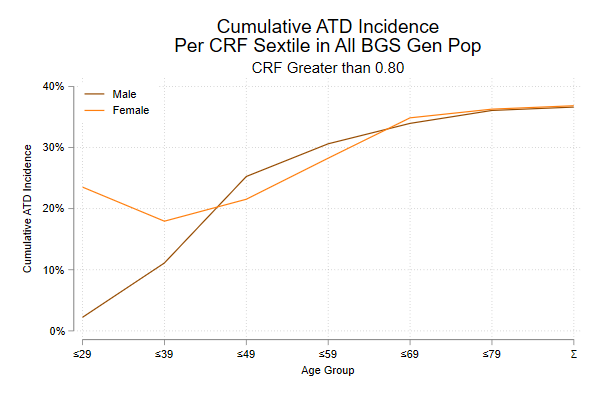
If one examines all of the CRF values, arranged by CRF sextile, patient age/gender and number of ATD patients per CRF cohort, then one can generate reverse Kaplan-Meier curves—that is time to event rather than time of survival. This is seen in Table V A-C and Figures III A-F. For purposes of comparison, in Figures III A-F, the Kaplan-Meier curves for men and women are placed on the same graph. The curves for men and women are quite similar. Table V-B is used for men and Table V-C for women. By way of illustration, and for example, the male cohort with a cumulative age of 49 years or less and a CRF of 0.80 or higher has an ATD risk of 25% (48/190) prevalence of ATD. The ATD prevalence can be calculated for each age-CRF sextile. For each CRF sextile, a curve can be created giving the ATD prevalence for each age group. When this is done, a series of six Kaplan-Meier curves is created. The curve for the CRF of 0.80 or higher rises more rapidly than does the curve for a CRF=O.75-0.79, which in turn rises more rapidly than the curve for CRF=0.70-0.74, which in turn rises more rapidly than the curve for CRF=0.65-0.69, which in turn rises more rapidly than the curve for CRF=0.60-0.64, which, finally, rises more rapidly than the curve for CRF=0.59 or lower. These curves are presented in terms of both males (brown color) and females (orange color). It will be apparent that the curves for males and for emales are very close to be overlapping. This implies that the various trials that have been done to evaluate dyslipidemia therapy (mainly involving men) will also be applicable to women. This finding is supported by noting that the ATD risk curves are virtually identical for men and women, whether those curves lie above the ASRL or below the ASRL. (Data available, not shown)
| Sex | + | Past | - | ||
| Male | |||||
| Above ASR Line | Total Patients | 166 | 154 | 113 | |
| Total Patient Years | 8715 | 10215 | 7575 | ||
| Ave. Age of ATD Onset | 53 | 66 | 67 | ||
| Below ASR Line | Total Patients | 25 | 23 | 14 | |
| Total Patient Years | 1455 | 1650 | 1035 | ||
| Ave. Age of ATD Onset | 58 | 72 | 74 | ||
| Female | |||||
| Above ASR Line | Total Patients | 87 | 67 | 158 | |
| Total Patient Years | 5050 | 4601 | 11595 | ||
| Ave. Age of ATD Onset | 58 | 69 | 73 | ||
| Below ASR Line | Total Patients | 29 | 22 | 48 | |
| Total Patient Years | 1741 | 1498 | 3437 | ||
| Ave. Age of ATD Onset | 60 | 68 | 72 | ||
Table II
| Ave Age of ATD Onset | ||||||
| Σ ATD. Pop | ||||||
| Cigarettes | ||||||
| Zone | + | Past | OT | NT | Σ | |
| IA | 102 | 61 | 7 | 64 | 234 | |
| 5362 | 3890 | 461 | 4193 | 13906 | ||
| 53 | 64 | 66 | 66 | 59 | ||
| IB | 2 | 1 | 2 | 5 | ||
| 97 | 38 | 174 | 309 | |||
| 49 | 38 | 87 | 62 | |||
| II | 83 | 89 | 7 | 102 | 281 | |
| 4670 | 5888 | 481 | 7185 | 18224 | ||
| 56 | 66 | 69 | 70 | 65 | ||
| IIIA | 39 | 49 | 7 | 64 | 159 | |
| 2172 | 3527 | 531 | 4817 | 11047 | ||
| 56 | 72 | 76 | 75 | 69 | ||
| IIIB | 11 | 17 | 1 | 17 | 46 | |
| 680 | 1261 | 86 | 1242 | 3269 | ||
| 62 | 74 | 86 | 73 | 71 | ||
| IVA | 29 | 21 | 1 | 20 | 71 | |
| 1561 | 1452 | 79 | 1502 | 4594 | ||
| 54 | 69 | 79 | 75 | 65 | ||
| IVB | 42 | 27 | 41 | 1 | 111 | |
| 2474 | 1853 | 2891 | 75 | 7293 | ||
| 59 | 69 | 71 | 75 | 66 | ||
| Σ | 308 | 265 | 23 | 310 | 1 | 907 |
| 17016 | 17909 | 1638 | 22004 | 75 | 58642 | |
| 55 | 68 | 71 | 71 | 75 | 65 | |
Table III-B
| Ave Age of ATD Onset | ||||||
| Σ Male ATD. Pop | ||||||
| Cigarettes | ||||||
| Zone | + | Past | OT | NT | Σ | |
| IA | 65 | 44 | 7 | 35 | 151 | |
| 3345 | 2786 | 461 | 2198 | 8790 | ||
| 51 | 63 | 66 | 63 | 58 | ||
| IB | 1 | 1 | 2 | |||
| 50 | 85 | 135 | ||||
| 50 | 85 | 68 | ||||
| II | 58 | 64 | 7 | 35 | 164 | |
| 3105 | 4208 | 481 | 2394 | 10188 | ||
| 54 | 66 | 69 | 68 | 62 | ||
| IIIA | 25 | 30 | 7 | 15 | 77 | |
| 1382 | 2114 | 531 | 993 | 5020 | ||
| 55 | 70 | 76 | 66 | 65 | ||
| IIIB | 4 | 12 | 1 | 2 | 19 | |
| 208 | 880 | 86 | 120 | 1294 | ||
| 52 | 73 | 86 | 60 | 68 | ||
| IVA | 18 | 16 | 1 | 7 | 42 | |
| 883 | 1107 | 79 | 516 | 2585 | ||
| 49 | 69 | 79 | 74 | 62 | ||
| IVB | 20 | 11 | 9 | 1 | 41 | |
| 1197 | 770 | 667 | 75 | 2709 | ||
| 60 | 69 | 74 | 75 | 66 | ||
| Σ | 191 | 177 | 23 | 104 | 1 | 496 |
| 10170 | 11865 | 1638 | 6973 | 75 | 30721 | |
| 53 | 67 | 71 | 67 | 75 | 62 | |
Table III-C
| Ave Age of ATD Onset | ||||||
| Σ Female ATD. Pop | ||||||
| Cigarettes | ||||||
| Zone | + | Past | OT | NT | Σ | |
| IA | 37 | 17 | 29 | 83 | ||
| 2017 | 1104 | 1994 | 5115 | |||
| 55 | 65 | 69 | 62 | |||
| IB | 1 | 1 | 1 | 3 | ||
| 47 | 38 | 89 | 174 | |||
| 47 | 38 | 89 | 58 | |||
| II | 25 | 25 | 67 | 117 | ||
| 1565 | 1680 | 4791 | 8036 | |||
| 54 | 67 | 72 | 69 | |||
| IIIA | 14 | 19 | 49 | 82 | ||
| 790 | 1413 | 3824 | 6027 | |||
| 56 | 74 | 78 | 74 | |||
| IIIB | 7 | 5 | 15 | 27 | ||
| 472 | 381 | 1122 | 1975 | |||
| 67 | 76 | 75 | 73 | |||
| IVA | 11 | 5 | 13 | 29 | ||
| 678 | 345 | 986 | 2009 | |||
| 62 | 69 | 76 | 69 | |||
| IVB | 22 | 16 | 32 | 70 | ||
| 1277 | 1083 | 2224 | 4584 | |||
| 58 | 69 | 70 | 65 | |||
| Σ | 117 | 88 | 206 | 411 | ||
| 6846 | 6044 | 15030 | 27920 | |||
| 59 | 69 | 73 | 68 | |||
Table IV-A
| CRF vs SBP: Σ Cigarettes | |||||||
| ΣATD. Pop | |||||||
| SBP: No Rx | |||||||
| SBP | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≥180 | 8 | 14 | 8 | 10 | 5 | 10 | 55 |
| 451 | 976 | 555 | 632 | 337 | 672 | 3623 | |
| 56 | 70 | 69 | 63 | 67 | 67 | 66 | |
| 160-178 | 9 | 18 | 16 | 11 | 10 | 17 | 81 |
| 522 | 1149 | 1158 | 767 | 684 | 1291 | 5571 | |
| 58 | 64 | 72 | 70 | 68 | 76 | 69 | |
| 140-158 | 32 | 32 | 24 | 18 | 15 | 41 | 162 |
| 1878 | 1930 | 1616 | 1234 | 932 | 2796 | 10386 | |
| 54 | 60 | 67 | 69 | 62 | 68 | 64 | |
| 130-138 | 31 | 21 | 22 | 11 | 17 | 29 | 131 |
| 1800 | 1307 | 1377 | 793 | 1163 | 1934 | 8374 | |
| 58 | 62 | 63 | 72 | 68 | 67 | 64 | |
| 120-128 | 29 | 32 | 24 | 20 | 13 | 31 | 149 |
| 1478 | 1899 | 1489 | 1174 | 884 | 2128 | 9052 | |
| 51 | 59 | 62 | 59 | 68 | 69 | 61 | |
| ≤118 | 21 | 17 | 20 | 19 | 12 | 49 | 138 |
| 1298 | 997 | 1121 | 1235 | 737 | 3106 | 8494 | |
| 62 | 59 | 56 | 65 | 61 | 63 | 62 | |
| Σ | 130 | 134 | 114 | 89 | 72 | 177 | 716 |
| 7427 | 8258 | 7316 | 5835 | 4737 | 11927 | 45500 | |
| 57 | 62 | 64 | 66 | 66 | 67 | 64 | |
Table IV-B
| CRF vs SBP | |||||||
| ΣATD. Pop | |||||||
| + Cigarettes; SBP: No Rx | |||||||
| SBP | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≥180 | 3 | 4 | 1 | 5 | 1 | 4 | 18 |
| 145 | 233 | 56 | 244 | 76 | 236 | 990 | |
| 48 | 58 | 56 | 49 | 76 | 59 | 55 | |
| 160-178 | 4 | 6 | 5 | 3 | 3 | 5 | 26 |
| 228 | 342 | 308 | 167 | 167 | 317 | 1529 | |
| 57 | 57 | 62 | 56 | 56 | 63 | 59 | |
| 140-158 | 15 | 9 | 5 | 4 | 4 | 13 | 50 |
| 768 | 470 | 265 | 204 | 222 | 741 | 2670 | |
| 54 | 52 | 53 | 51 | 56 | 57 | 53 | |
| 130-138 | 14 | 9 | 11 | 1 | 7 | 6 | 48 |
| 726 | 462 | 600 | 66 | 448 | 369 | 2671 | |
| 52 | 51 | 55 | 66 | 64 | 62 | 56 | |
| 120-128 | 16 | 12 | 9 | 8 | 9 | 9 | 63 |
| 724 | 696 | 452 | 375 | 566 | 515 | 3328 | |
| 45 | 58 | 50 | 47 | 63 | 57 | 53 | |
| ≤118 | 8 | 6 | 11 | 9 | 9 | 21 | 64 |
| 375 | 298 | 620 | 507 | 474 | 1224 | 3498 | |
| 47 | 50 | 56 | 56 | 53 | 58 | 55 | |
| Σ | 60 | 46 | 42 | 30 | 33 | 58 | 269 |
| 2966 | 2501 | 2301 | 1563 | 1953 | 3402 | 14686 | |
| 49 | 54 | 55 | 52 | 59 | 59 | 55 | |
Table IV-C
| CRF vs SBP | |||||||
| ΣATD. Pop | |||||||
| Past Cigarettes; SBP: No Rx | |||||||
| SBP | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≥180 | 2 | 4 | 1 | 3 | 2 | 3 | 15 |
| 113 | 298 | 63 | 246 | 134 | 198 | 1052 | |
| 57 | 75 | 63 | 82 | 67 | 66 | 70 | |
| 160-178 | 5 | 6 | 3 | 3 | 2 | 4 | 23 |
| 294 | 394 | 221 | 240 | 111 | 290 | 1550 | |
| 59 | 66 | 74 | 80 | 56 | 73 | 67 | |
| 140-158 | 10 | 14 | 12 | 7 | 2 | 16 | 61 |
| 658 | 890 | 828 | 484 | 124 | 1164 | 4148 | |
| 54 | 64 | 69 | 69 | 62 | 73 | 68 | |
| 130-138 | 8 | 5 | 6 | 6 | 4 | 12 | 41 |
| 446 | 344 | 426 | 422 | 271 | 800 | 2709 | |
| 56 | 69 | 71 | 70 | 68 | 67 | 66 | |
| 120-128 | 8 | 9 | 5 | 6 | 3 | 7 | 38 |
| 481 | 581 | 335 | 414 | 230 | 501 | 2542 | |
| 60 | 65 | 67 | 69 | 77 | 72 | 67 | |
| ≤118 | 7 | 1 | 4 | 5 | 1 | 11 | 29 |
| 461 | 41 | 162 | 344 | 87 | 785 | 1880 | |
| 66 | 41 | 41 | 69 | 87 | 71 | 65 | |
| Σ | 40 | 39 | 31 | 30 | 14 | 53 | 207 |
| 2453 | 2548 | 2035 | 2150 | 957 | 3738 | 13881 | |
| 61 | 65 | 66 | 72 | 68 | 71 | 67 | |
Table IV-D
| CRF vs SBP | |||||||
| ΣATD. Pop | |||||||
| Σ- Cigarettes; SBP: No Rx | |||||||
| SBP | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≥180 | 3 | 6 | 6 | 2 | 2 | 3 | 22 |
| 193 | 445 | 436 | 142 | 127 | 241 | 1584 | |
| 64 | 74 | 73 | 71 | 64 | 80 | 72 | |
| 160-178 | 6 | 8 | 5 | 5 | 8 | 32 | |
| 413 | 629 | 360 | 406 | 684 | 2492 | ||
| 69 | 79 | 72 | 81 | 86 | 78 | ||
| 140-158 | 7 | 9 | 7 | 7 | 9 | 12 | 51 |
| 452 | 570 | 523 | 546 | 586 | 891 | 3568 | |
| 65 | 63 | 75 | 78 | 65 | 74 | 70 | |
| 130-138 | 9 | 7 | 5 | 4 | 6 | 11 | 42 |
| 628 | 501 | 351 | 305 | 444 | 765 | 2994 | |
| 70 | 72 | 70 | 76 | 74 | 70 | 71 | |
| 120-128 | 5 | 11 | 10 | 6 | 1 | 14 | 47 |
| 273 | 622 | 702 | 385 | 88 | 1037 | 3107 | |
| 55 | 57 | 70 | 64 | 88 | 74 | 66 | |
| ≤118 | 6 | 10 | 5 | 5 | 2 | 17 | 45 |
| 462 | 658 | 339 | 384 | 176 | 1097 | 3116 | |
| 77 | 66 | 68 | 77 | 88 | 65 | 69 | |
| Σ | 30 | 49 | 41 | 29 | 25 | 65 | 239 |
| 2008 | 3209 | 2980 | 2122 | 1827 | 4715 | 16861 | |
| 67 | 65 | 73 | 73 | 73 | 73 | 71 | |
Table V-A
| Cumulative ATD Risk | |||||||
| Σ Σ Gen Pop | |||||||
| Σ Σ Cigarettes | |||||||
| Age Group | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≤29 | 5 | 8 | 7 | 2 | 6 | 11 | 39 |
| 62 | 96 | 139 | 189 | 157 | 711 | 1354 | |
| 8% | 8% | 5% | 1% | 4% | 2% | 3% | |
| ≤39 | 19 | 25 | 20 | 14 | 10 | 24 | 112 |
| 147 | 198 | 236 | 277 | 219 | 933 | 2010 | |
| 13% | 13% | 8% | 5% | 5% | 3% | 6% | |
| ≤49 | 62 | 58 | 43 | 27 | 20 | 55 | 265 |
| 255 | 311 | 332 | 342 | 276 | 1089 | 2605 | |
| 24% | 19% | 13% | 8% | 7% | 5% | 10% | |
| ≤59 | 101 | 86 | 70 | 43 | 39 | 97 | 436 |
| 337 | 374 | 408 | 393 | 316 | 1214 | 3042 | |
| 30% | 23% | 17% | 11% | 12% | 8% | 14% | |
| ≤69 | 129 | 125 | 103 | 75 | 54 | 97 | 583 |
| 337 | 436 | 457 | 451 | 347 | 1278 | 3306 | |
| 38% | 29% | 23% | 17% | 16% | 8% | 18% | |
| ≤79 | 142 | 142 | 126 | 97 | 69 | 162 | 738 |
| 393 | 459 | 486 | 481 | 365 | 1328 | 3512 | |
| 36% | 31% | 26% | 20% | 19% | 12% | 21% | |
| Σ | 146 | 157 | 139 | 109 | 78 | 191 | 820 |
| 398 | 466 | 501 | 495 | 377 | 1363 | 3600 | |
| 37% | 34% | 28% | 22% | 21% | 14% | 23% | |
Table V-B
| Cumulative ATD Risk | |||||||
| Σ Male Gen Pop | |||||||
| Σ Σ Cigarettes | |||||||
| Age Group | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≤29 | 1 | 4 | 2 | 2 | 3 | 3 | 15 |
| 45 | 50 | 81 | 98 | 78 | 289 | 641 | |
| 2% | 8% | 2% | 2% | 4% | 1% | 2% | |
| ≤39 | 12 | 15 | 11 | 9 | 5 | 9 | 61 |
| 108 | 128 | 136 | 151 | 105 | 352 | 980 | |
| 11% | 12% | 8% | 6% | 5% | 3% | 6% | |
| ≤49 | 48 | 36 | 28 | 19 | 10 | 23 | 164 |
| 190 | 200 | 196 | 189 | 138 | 398 | 1311 | |
| 25% | 18% | 14% | 10% | 7% | 6% | 13% | |
| ≤59 | 75 | 59 | 44 | 28 | 20 | 45 | 271 |
| 245 | 244 | 239 | 218 | 156 | 446 | 1548 | |
| 31% | 24% | 18% | 13% | 13% | 10% | 18% | |
| ≤69 | 91 | 77 | 58 | 39 | 24 | 58 | 347 |
| 268 | 276 | 262 | 242 | 170 | 472 | 1690 | |
| 34% | 28% | 22% | 16% | 14% | 12% | 21% | |
| ≤79 | 101 | 88 | 71 | 52 | 29 | 72 | 413 |
| 280 | 291 | 276 | 259 | 175 | 490 | 1771 | |
| 36% | 30% | 26% | 20% | 17% | 15% | 23% | |
| Σ | 104 | 91 | 77 | 56 | 32 | 79 | 439 |
| 284 | 295 | 284 | 264 | 179 | 500 | 1806 | |
| 37% | 31% | 27% | 21% | 18% | 16% | 24% | |
Table V-C
| Cumulative ATD Risk | |||||||
| Σ Female Gen Pop | |||||||
| Σ Σ Cigarettes | |||||||
| Age Group | ≥0.80 | 0.75-0.79 | 0.70-0.74 | 0.65-0.69 | 0.60-0.64 | ≤0.59 | Σ |
| ≤29 | 4 | 4 | 5 | 0 | 3 | 8 | 24 |
| 17 | 46 | 58 | 91 | 79 | 422 | 713 | |
| 24% | 9% | 9% | 0% | 4% | 2% | 3% | |
| ≤39 | 7 | 10 | 9 | 5 | 5 | 15 | 51 |
| 39 | 70 | 100 | 126 | 114 | 581 | 1030 | |
| 18% | 14% | 9% | 4% | 4% | 3% | 5% | |
| ≤49 | 14 | 22 | 15 | 8 | 10 | 32 | 101 |
| 65 | 111 | 136 | 153 | 138 | 691 | 1294 | |
| 22% | 20% | 11% | 5% | 7% | 5% | 8% | |
| ≤59 | 26 | 27 | 26 | 15 | 19 | 52 | 165 |
| 92 | 130 | 169 | 175 | 160 | 768 | 1494 | |
| 28% | 21% | 15% | 9% | 12% | 7% | 11% | |
| ≤69 | 38 | 48 | 45 | 36 | 30 | 70 | 267 |
| 109 | 160 | 195 | 209 | 177 | 806 | 1656 | |
| 35% | 30% | 23% | 17% | 17% | 9% | 16% | |
| ≤79 | 41 | 54 | 55 | 45 | 40 | 90 | 325 |
| 113 | 168 | 210 | 222 | 190 | 838 | 1741 | |
| 36% | 32% | 26% | 20% | 21% | 11% | 19% | |
| Σ | 42 | 56 | 62 | 53 | 46 | 112 | 371 |
| 114 | 171 | 217 | 231 | 198 | 863 | 1794 | |
| 37% | 33% | 29% | 23% | 23% | 13% | 21% | |
Table VI-A
End of Trial LDL-C
| Trial | Angiographic Outcome | > 200 | 175-199 | 150-174 | 125-149 | 100-124 | < 99> |
| POSCH | Progression Non Progression ∑ % Progression | 26 15 41 63% | 45 27 72 63% | 51 82 133 38% | 27 83 110 25% | 12 94 106 11% | 2 267 269 1% |
| NHLBI | Progression Non Progression ∑ % Progression | 16 37 53 30% | 1 10 11 9% | 4 9 13 31% | 0 4 4 0% | 0 7 7 0% | 0 2 2 0% |
| FATS | Progression Non Progression ∑ % Progression | 5 7 12 42% | 5 10 15 33% | 7 8 15 47% | 7 12 19 37% | 9 18 27 33% | 5 27 32 16% |
| LCAS | Progression Non Progression ∑ % Progression | 1 2 3 33% | 6 12 18 33% | 14 25 39 36% | 32 54 86 37% | 39 72 111 35% | 21 55 76 27% |
| PLAC-1 | Progression Non Progression ∑ % Progression | 7 9 16 44% | 21 15 36 58% | 38 32 70 54% | 29 55 84 35% | 31 53 84 37% | 13 17 30 43% |
| Heidelburg | Progression Non Progression ∑ % Progression | 6 6 12 50% | 7 16 23 30% | 8 16 24 33% | 6 10 16 38% | 2 9 11 18% | 2 1 3 67% |
| LOCAT | Progression Non Progression ∑ % Progression | 10 1 11 91% | 22 8 30 73% | 63 29 92 68% | 77 50 127 61% | 38 35 73 52% | 17 21 38 45% |
POSCH Means Program on the Surgical Control of the Hyperlipidemias
NHLBI Means National Heart Lung and Blood Institute
FATS Means Familial atherosclerosis Treatment Study
LCAS Means Lipoprotein and Coronary Atherosclerosis Study
PLAC-1 Means Pravastatin Limitation of Atherosclerosis in the Coronary Arteries
Heidelburg Means Study on The Effects of Regular Physical Exercise and Low-Fat Diet on the Progression of Coronary Artery Disease
LOCAT Means Lopid Coronary Angiography Trial
Table VI-B
End of Trial LDL-C
| Trial | Angiographic Outcome | 90-99 | 80-89 | 70-79 | 60-69 | 50-59 | 40-49 | < 39> |
| POSCH | Progression Non Progression ∑ % Progression | 0 73 73 0% | 0 69 69 0% | 0 60 60 0% | 0 31 31 0% | 1 16 17 6% | 0 4 4 0% | 1 14 15 7% |
| NHLBI | Progression Non Progression ∑ % Progression | 0 1 1 0% |
|
| 0 1 1 0% | |||
| FATS | Progression Non Progression ∑ % Progression | 1 8 9 11% | 3 9 12 25% | 1 6 7 14% | 0 2 2 0% | 0 2 2 0% | ||
| LCAS | Progression Non Progression ∑ % Progression | 9 20 29 31% | 9 20 29 31% | 1 10 11 9% | 2 4 6 33% | 0 1 1 0% | ||
| PLAC-1 | Progression Non Progression ∑ % Progression | 8 10 18 44% | 2 5 7 29% | 2 1 3 67% | 0 1 1 0% | 1 0 1 100% | ||
| Heidelburg | Progression Non Progression ∑ % Progression | 2 1 3 67% | ||||||
| LOCAT | Progression Non Progression ∑ % Progression | 9 7 16 56% | 5 6 11 45% | 2 3 5 40% | 1 2 3 33% | 0 3 3 0% |
POSCH Means Program on the Surgical Control of the Hyperlipidemias
NHLBI Means National Heart Lung and Blood Institute
FATS Means Familial atherosclerosis Treatment Study
LCAS Means Lipoprotein and Coronary Atherosclerosis Study
PLAC-1 Means Pravastatin Limitation of Atherosclerosis in the Coronary Arteries
Heidelburg Means Study on The Effects of Regular Physical Exercise and Low-Fat Diet on the Progression of Coronary Artery Disease
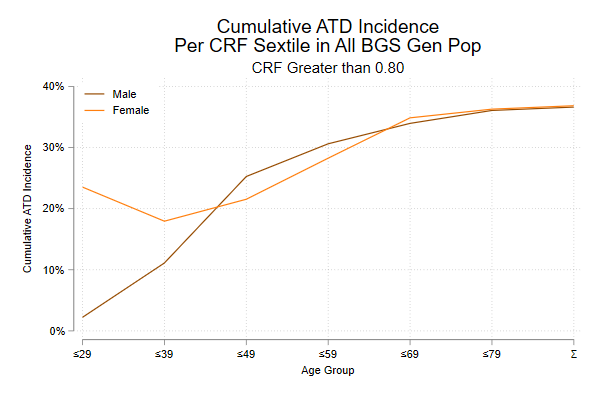
Figure III-A
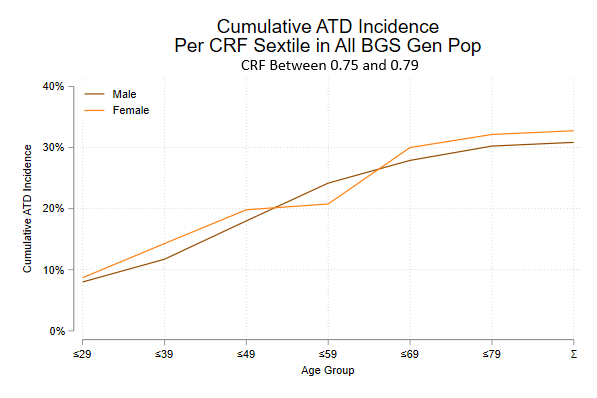
Figure III-B
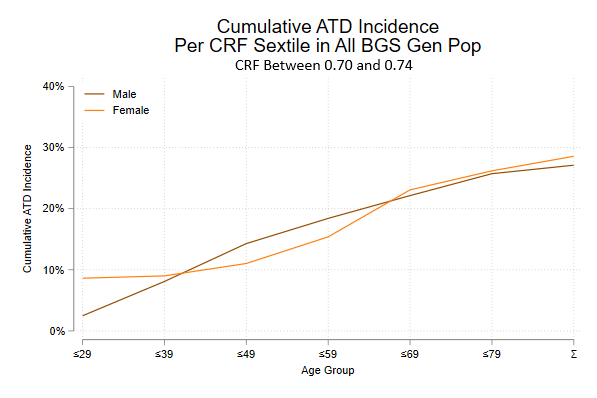
Figure III-C
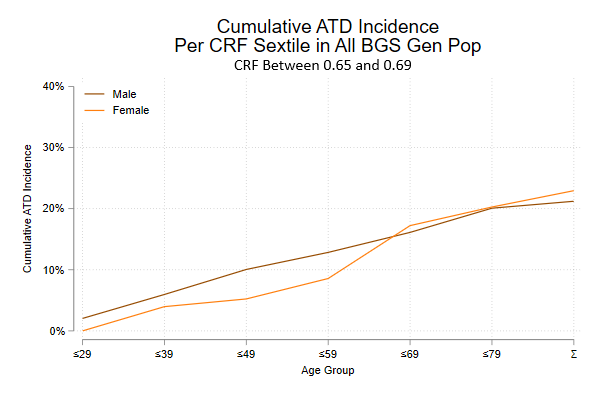
Figure III-D
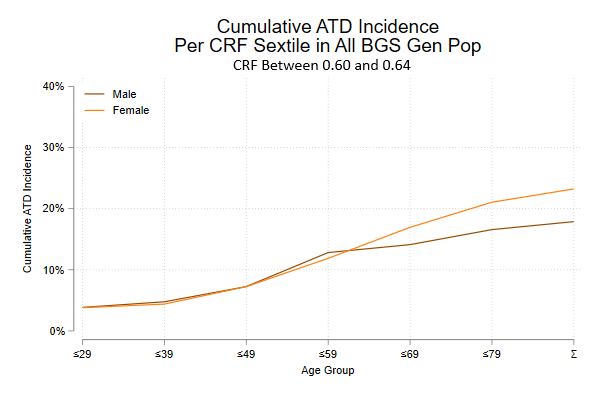
Figure III-E
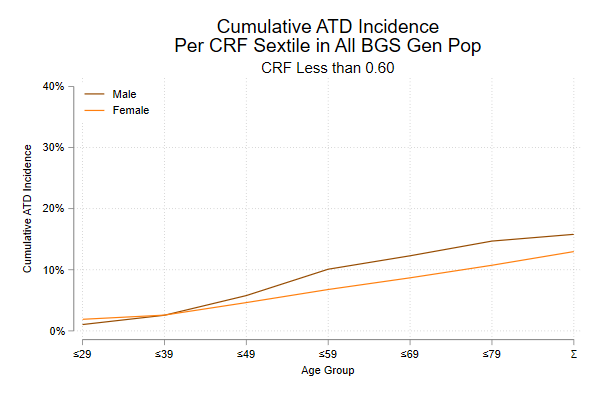
Figure III-F
Two caveats are note for this analysis. First, that follow-up in incomplete and it is not impossible that some of the patients who were lost to the author’s practice may have had values that may have influenced the prevalence of ATD or CRF-age cohort. The author had no control over
the loss of those patients. When Wood County Hospital took over the insurance coverage of those patients, it did so not knowing their lipid values. Thus there should be no selection bias involved. If anything, the “lost” patients who sustained ATD events unknown to the author should shift the curves to the left. And secondly, that the lipid values presented in this study are, as noted previously, upon the precipitation method of HDL-c measurement. The same approach could be used for lipids based on the enzymatic methodology of HDL-c measurement, using the corrections described earlier.
To utilize this approach, using the 15% lifetime risk parameter, one simply determines one’s CRF in order to select the appropriate Kaplan-Meier curve and then moves up the prevalence (vertical) arm of the Table until one gets to the 15% level. One then crosses over to the appropriate point on the Kaplan-Meier curve and drops down to the age group (horizontal) axis to determine the age group at which the 15% risk is associated. One begins treatment when that age group is reached, though it is the author’s preference to initiate treatment in the decade prior to reaching the age group specified by the Kaplan-Meier curves in order to give treatment a “head start.” Of course, any desired risk can be used, depending upon the investigator’s preferences.
It is common knowledge that lipids change with the length of life lived. In the author’s long experience, such changes may occur rapidly (yearly) or slowly (over decades). This has been termed “trajectory jumping.” This is an important concept because it is clear that ATD events do not happen the moment that one achieves a certain CRF, but rather it takes time for the CRF to form plaque within the artery wall. Knowing the history of CRF trajectory jumping—that is, how long one has had a given CRF—permits one to determine the need for therapy. Also, it may well be useful to know the rate of change of the “trajectory jumping,” since if a patient begins with a low CRF trajectory (say 0.59 or lower), but his/her CRF is rapidly changing then the goal of treatment is to prevent long term ATD, even though that patient is of no immediate ATD risk: the low short term risk but high long term risk scenario. After all, it would seem to be easier to prevent ATD earlier in life than to try to stabilize/regress more advanced ATD later in life. This concept is the basis for lipid testing in childhood with follow up testing depending on the CRF trajectory and trajectory jumping. The author considers this concept to be vital in the fight against ATD.
The above evaluation and treatment of dyslipidemia represents the ideal practice of epidemiology, though the United States Preventive Task Force Service (USPTFS) has opined against it.(28) The USPTFS is simply wrong on this topic, for the reasons outlined above. In Wood County and the city of Bowling Green, at least in the author’s long experience, lipid panels are rarely ordered by the physicians who attended the patient prior to that patient being seen by the author. Hence the author has no idea how long the dyslipidemia has been present and hence the state of any ATD that may be present (subclinical ATD). As a result, the author must assume that the dyslipidemia may have been present for a long enough period of time to cause plaque formation and to begin treatment immediately—especially when the patient’s CRF value is on the more rapidly progressive trajectory, or in the older patients when the CRF is on the moderately progressive trajectory. The minimally progressive trajectory (CRF of 0.59 or lower) is rarely treated and if the patient remains on this trajectory, he will not reach the 15% threshold until the latter part of the eighth decade of life and she will not reach that threshold until the ninth decade of life if ever.
The author has published an article detailing ATD risk factors in patients aged 19 years or less in his family practice. (29) Cigarette smoking was present in 10% of these patients; elevated CRF (0.70 or higher), in 15%; elevated LDL-c (125 mg/dl [3.2 mmoles/L] or higher), in 23%; low HDL-c (39 mg/dl [1.0 mmoles/L] or lower) in 28%; and elevated CT (200 mg/dl [5.2 mmoles/L] or higher), in 14%. TG, 2 hr postprandial glucose levels , SBP, and body mass index were not elevated in the vast majority of cases. Males tended to have lower HDL-c, whole females tended to have higher LDL-c. This counteracts the idea that children do not have ATD risk factors and supports early and repeated testing.
The next question is how far to lower LDL-c. The author has in his physical possession the actual data bases of eight published angiographic regression trials. These trials are as follows: 1) Saint Thomas Atherosclerosis Regression trial (STARS) (30), 2) the Program on the Surgical Control of the Hyperlipidemias (POSCH) (31), 3) the National Heart, lung, and Blood Institute Type II Coronary Intervention Study (NHLBI) (32), 4) Lipoprotein and Coronary Atherosclerosis Study (LCAS) (26), 4) Familial Atherosclerosis Treatment Study (FATS) (33), 5) Pravastatin Limitation of Atherosclerosis in the Coronary Arteries (PLAC-1) (34), Lopid Coronary Artery Trial (LOCAT) (35), and the Heidelberg Study (36). POSCH is a surgical (partial ileal bypass) trial; STARS, FATS, and NHLBI, resin trials, though FATS had a statin arm and a niacin arm to go with the resin : LCAS and PLAC-1 are statin trials, though in LCAS resins might be used to achieve lipid goals if those goals were not achieved by fluvastatin; LOCAT is a fibrate trial; and Heidelberg is a diet and exercise trial. Angiographic regression trials are known to predict clinical outcomes, with plaque regression being associated with fewer subsequent ATD events and plaque progression associated with more subsequent ATD events. (37,38)
Table VI-A shows the rates of plaque progression at the end-of-trail LDL-c levels of each trial. Since the goal of dyslipidemia therapy is and always must be the stabilization/regression of plaque, it is clear that the lower the end-of-trial LDL-c, the lower the rate of associated plaque progression. The best results were obtained with POSCH and NHLBI, whereas the least good results were obtained in LOCAT and the Heidelberg trial—at the same end-of-trial LDL-c levels. This result is at odds with the current mantra that it does not make a difference how LDL-c is lowered—only that the goal is achieved.
Table VI-B show the same findings as Table VI-A, but for end-of-trial LDL-c levels below 99 mg/dl (2.5 mmoles/L). There is basically no difference if plaque progression rate rates at any end-of-trial LDL-c level below 80 mg/dl (2.0 mmoles/L) This result is at odds with the current mantra that “Lower is better” with respect to LDL-c.
The author has advocated the use of the CRF and CThr and yet he has used the end-of-trial LDL-c to measure the success of dyslipidemia therapy. The author favored LDL-c in this analysis because it was marginally better at predicting plaque progression. The question is why this is so. The answer may lie in the fact that when choline and carnitine are delivered to the terminal ileum, they are metabolized to trimethyl alanine (TMA). TMA is then absorbed into to intestinal blood vesels and taken to the liver where TMA is oxidized to YMA-oxide (TMAO). TMAO is thrombogenic and also blocks reverse cholesterol transport. (39) This hypothesis is suggested by the remarkable decreases in plaque progression when choline and carnitine are shunted away from the terminal ileum (POSCH) or are bound to resins (NHLBI). The intermediate results (plaque progression) in FATS and LCAS) when resins may/may not have been given at maximally tolerated doses would further support this hypothesis. (FATS used colestipol as the baseline therapy, with one arm receiving lovastatin and the other arm receiving niacin. In LCAS resins were given only when fluvastatin failed to achieve goals of lipid therapy.) PLAC-1, LOCAT, and Heidelberg did not involve the use of resins and had the worst results.
This is pertinent because in POSCH, using the CRF as the measure of dyslipidemia treatment results, a rise of the CRF at one year after initiation of therapy—even minutely—always resulted in plaque progression at the three-year angiogram. Conversely, a fall in the CRF at one year after initiation of therapy—even minutely-- always resulted in plaque non-progression. No exceptions. (40) Additionally, the author has reported the case of a post-myocardial infarction female patient who reached her 104th birthday, still taking her statin, some 25 years post infarction, and being followed by CRF. Her LDL-c levels never achieved 79 mg./dl (2.0 mmoles/L). (41) The author has also reported the case of a man with ATD risk factors, but free of clinical ATD, who reached his `100th birthday, still taking his statin, before passing away. Because his HDL-c was very low, he was followed by LDL-c level and his LDL-c was basically kept below 99 mg/dl ( Precip but 89 mg/dl if Enz) (2.6 mmoles/L and 2.3 mmoles/L respectively) until the more potent statins, whereupon his LDL-c was lowered even farther to below 80 mg/dl (Precip, but below 70 mg/dl if Enz) ( 2.1 mmoles/L and 1.8 mmoles/L respectively ). His total time of therapy was 29 years. (42)
Finally, for any treatment proposal, the “proof of the pudding is in the eating.” To this end the author has examined his database for patients with AMI/ACI, both male and female. This involves inspection of records dating back 30-40 years and such data can be difficult to extract. Even so, there were 133 male and 70 female patients with the diagnosis of AMI/ACI, Of those patients only 5 male and 9 female patients had one of these events within the last 10 years and only 1 male and 3 female patients within the last 5 years. All but one of the 5 males and 5 of the nine females were current cigarette smokers, which means that at best the author could only delay the onset of their AMI/ACI events—or as the author tells his patients, ”I can save you from many conditions, but not from the effects of cigarette smoking. You have to quit smoking.” There were no strokes. The author suggests that in addition to the power of statins to prevent ATD, the guidelines offered in this manuscript may have played a major role in these results.
This has been a long manuscript, but the author wanted to put all of his work, old and new, into one site, readily accessible to all. As far as the virtual elimination of early/middle aged ATD is concerned, one must be able to predict the population at risk of ATD with high accuracy to assure that no future ATD patient is mischaracterized as being at little risk of an ATD event, only to have such an event occur. It is not possible to predict everyone who will sustain an ATD event under age 75-80 years, but the vast majority of these patients are predictable and hence their ATD event preventable, so long as the protocols described in this paper are followed. However, this ideal scenario is not always at hand. Some patients will not be seen in the physician’s office until shortly before the ATD event occurs and the physician will not have the time needed to stabilize/regress any extant ATD. Such cases do not represent a failure of ATD prevention but rather a failure to take advantage of the protocol. The following dicta are fundamental to ATD eradication and must be understood by the patient as well as by the treating physician. These dicta are taken from the findings of the FHS, with some supplementation by the author:
To these precepts, this author would add the following corollaries:
When all of these precepts are taken into account, the protection of patients from ATD—and hence the virtual elimination of ATD, at least until very late in life—is straight forward.
First and foremost is the determination of the patient’s ATD risk factors. This must include a full lipid panel (CT, LDL-c, HDL-c, and TG, since LDL-c will likely be calculated by the Friedewald formula as noted earlier). Knowing the patient’s cigarette smoking status is fundamental to determining risk of clinical ATD. And of course knowing the patient’s SBP and 2 hour postprandial blood sugar (see Appendix for the protocol) is also important.
The first step in treatment, as noted above, is the cessation of cigarette smoking. If this is not accomplished, the plaques will continue to evolve, though the lower the CRF, the later in life the ATD event will occur.
The next step is to calculate one’s CRF. Remember that this author’s work was done when the Precip method of HDL-c measurement was the gold standard. If the treating physician must use the Enz method of HDL-c measurement, he/she will have to make the adjustments the author noted earlier, which means that the CRF goals will need to be lowered by 0.1 and the LDL-c goals by 10 mg/dl (0.25 mmoles/L). Then combine the CRF with the SBP and find the patient’s position on the BGS graph. If that CRF-SBP plot is located below the ASRL and the patient has never smoked cigarettes, the physician need go no further. There is no “safe” place in interventional lipidology/preventive cardiology, but the patient is as close to a “safe” place as he/she can get. The physician must also remember that lipids change over time, and with that change comes a change in ATD risk, so periodic follow-up is necessary. A CRF that remains at levels of 0.59 or lower rarely requires treatment—unless of course the patient’s LDL-c is 170 mg/dl (4.4 mmols/L), in which case treatment is necessary.
A CRF-SBP plot above the ASRL, on the other hand, entails a large variation in ATD risk. The initial phase of follow-up for those with CRF-SBP plots above the ASRL is to decide the broad classification of the patient’s ATD risk: pure dyslipidemia, dyslpidemic hypertension, or pure hypertension. The ATD risk is highest for pure dyslipidemia; dyslipidemic hypertension has the next highest risk; and pure hypertension has the lowest risk of these three categories. Given this finding, the physician should be careful to not use anti-hypertensive medications that elevate the CRF. People who have neither dyslipidemia nor hypertension, and who have never smoked cigarettes, are at low risk.(45)
The next step is to determine when to begin therapy. Such a decision is based on the patient’s perceived risk of ATD. This can be done using the method described in this manuscript. First, one simply locates the patient’s plot on the appropriate CRF graph as portrayed in Figures III A-F in light of the patient’s current age and begin therapy about a decade prior to the average age of ATD onset. The presence of cigarette smoking implies an urgent need to begin therapy; the absence of cigarette smoking allows a more measured determination of when to begin therapy. This decision can be enhanced by determining the patient’s ATD risk using the reverse Kaplan-Meier curves located in Tables V A-F. The author suggests using a lifetime risk of 15%, but the threshold of ATD risk is up to the treating physician. Treatment should be begun about a decade prior to the age indicated on the Figure. Treatment should be begun about a decade prior to the age group indicated by the graph to allow time to achieve the desired goal, lest the patient “run out of time” and the ATD event occur prior to the patient achieving the desired goal of therapy. The goal of therapy is determined by the angiographic studies as noted in Tables VI A-B. For those patients free of clinical ATD, a LDL-c goal of 99 mg/dl (Precip, but 89 mg/dl if Enz; 2.5 mmoles/L and 2.3 mmoles/L respectively). For people with clinical ATD a goal of 79 mg/dl or lower (Precip, but 69 mg/dl if Enz; 2.0 mmoloes/L and 1.8 mmoles/L respectively).). This latter goal could also be considered for those with very high baseline CRF or LDL-c levels, who may have subclinical ATD. If the patient is undergoing an acute ATD event, an argument could be made to lower LDL-c to 55 mg/dl (1.4 mmoles/L) or lower during the acute inflammatory phase, but once the patient is stable, say at 6 months, then the LDL-c goal could be reduced to the 79 mg/dl (Precip, but 69 mg/dl if Enz) (2.0 and 1.8 mmoles/L respectively).
Appendix II contains the breakdown of the various ATD events in the author’s ATD database, in terms of ATD of the coronary circulation, cerebral circulation, and the peripheral vascular circulatin.
Using the approach outlined in this manuscript, the author has had a remarkable reduction in ATD events in his practice of family medicine. The approach is simple and easily implemented into medical practice. It works for both genders and all ages. Physicians can understand this methodology and more importantly, patients can understand it as well, and it is well known that a patient who understands why he/she is being treated is more likely to continue with that treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
