
Research Article | DOI: https://doi.org/10.31579/2578-8868/217
¹Corresponding author, Box hill Hospital, Eastern Health, Victoria, and Australia.
²Department of Radiology, Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
³Department of Radiology, Emam Jafar Sadegh Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
⁴Department of Radiology, Shahid Beheshti University of Medical Sciences/Tehran/ Iran.
*Corresponding Author: Farzaneh Mohammadi, Box hill Hospital, Eastern Health, Victoria, and Australia.
Citation: Farzaneh Mohammadi, Hussein Soleimantabar, Fatemeh Mohamadi, Sofia Sabouri (2021). The vertebral Artery Anomalous, Stenosis vs Hypoplasia as the leading cause of Stroke. An anatomical cross-Sectional Study of VA anomalies in Neck three-Dimensional computed Tomography Angiography. J. Neuroscience and Neurological Surgery. 10(1); DOI:10.31579/2578-8868/217
Copyright: © 2021 Farzaneh Mohammadi, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 30 October 2021 | Accepted: 07 December 2021 | Published: 13 December 2021
Keywords: vertebral artery; anomalies; ct angiography; significant stenosis; hypoplasia
Introduction: A thorough understanding of the vertebral artery (VA) variations and course of the artery and its related branches could significantly enhance the efficacy and safety of interventions involving the neck and spine. Here, we aimed to investigate the incidence of various VA variations in individuals presenting with signs and symptoms of stroke with our neurology team.
Material and Method: In this retrospective study we investigate CTA images of patients with signs and symptom of stroke who referred to specialized medical imaging centre. An experienced board-certified radiologist evaluated the CTA images, recording the characteristics of VA, regarding dominance and any possible anomalies. These included anomalous origin, anomalous route, anomalous branching, stenosis, hypoplasia, atresia, thrombosis, and dissection. All data were analyzed using SPSS version24 and Pearson Chi-Square and Fishers test used for anomaly and gender correlation.
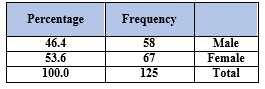
Results: A total of 125 patients (53.6% females; mean age, 60.7 (11-87)) were included. In the case of VA dominance, 66.4% of cases were co-dominant while 16.0% were right, and 12.8% were left dominant. Overall, males had more VA anomalies than females, 24.8% and 17.6%, respectively (in general, 42.4% of all participants) (p = 0.020). Among patients, 4.0% (n = 5) had an anomalous origin and anomalous branching was reported in 5 patients (4.0%). Among the variations, significant stenosis (18.4%) and hypoplasia (17.6%) were the most prevalent anomalies with the earliest one having the higher rate. While anomalous branching was reported in 5 patients (4.0%).
Conclusions: VA variations are relatively common and should be addressed during procedures involving the neck region and would allow surgeons to avoid life threatening injury.
The vertebral artery (VA) arises from the respective subclavian artery and connects the opposite site branch to form the basilar artery [1]. The VA is anatomically divided into four segments: V1, preforaminal; V2, foraminal; V3, atlantic; and V4 intracranial [2]. Anatomical variations mainly involve the distal segments of VA (V3 and V4). Several embryological explanations for these variations have been proposed in the literature [3].
With the growing use of vascular angiography, uncommon cases of hypoplasia, origin stenosis, and altered origin have thoroughly been diagnosed [4]. In Kauffman’s study, it was reported that patients with VA stenotic origin are correlated with less risk of stroke through intraarterial angiography [5]. The VA origin and aortic arch branching patterns should be assessed in cases of cerebrovascular accidents and VA dissection [6].
In Kim’s study, Vertebral Artery Hypoplasia (VAH) greatly contributes to a rising risk of Posterior cerebellar stroke (PCS) [7]. However, the rates of VAH reported in the literature vary markedly because there is currently no standard definition for this disorder [8]. The VA variations are highly significant from various clinical points of view. First of all, these variations could predispose some people to disorders impairing the blood supply to the head and neck. These could accompany other life-threatening vascular anomalies. In addition, spine surgeons and interventional radiologists might encounter problems in the VA during the procedure. It is noted that the incidence rate of VA injury in spine surgery has been reported to range from 0.3% to 8.2% [9,10,11].
Having a comprehensive understanding of the VA variations and course of the artery and its related branches preoperatively could significantly enhance the efficacy and safety of interventions involving the neck and spine, and subsequently enable surgeons to avoid injury [12]. In this study, we sought to investigate the incidence of various VA variations which would be helpful in head and neck surgery. Meanwhile, understanding the incidence of VA anomalies and variations and identifying which anomalies are more common in each gender in patients who present with signs and symptoms of stroke increases the early diagnosis and prevents life-threatening complications [13]. We are assessing individuals who presented with signs and symptoms of stroke to our neurology team and referred to the imaging centre to investigate the possibility of stroke.
Ethics approval
We conducted this study using data and CTA images from Medical Imaging center. Ethical approval for this Study and use of patients three-dimensional computed tomography angiography (CTA) images for collection and study was obtained originally from the local ethics committee and The National Committee for Ethics in Biomedical Research approved continuing this study.
All study participants provided written informed consent for studying their images. Patients explained regarding how their clinical data would be used in the study process. The patients' information remained confidential and identities were anonymous. All materials and methods were performed in accordance with the relevant guidelines and regulations and written informed consent for publication was obtained from patients.
2.1. Study design and participants
The present study was a single-center retrospective observational investigation. Inclusion criterion for this study was: individuals who visited our neurology team with signs and symptoms of stroke [7] therefore referred to our specialized medical imaging centre and underwent CTA of neck.
This study including patients with minimum age 18 years and maximum 87 years. This is not including pregnant ladies (Table 1,2). This study exclusion criteria were patients in whom VA was not clear or patients without proper contrast injection [7]. These patients underwent computed tomography (CT) angiography in September 2019, using the "census" sampling method.
In this descriptive, sample size calculated with formula:
According to Soltani study, considering Prevalence (P) = 5%, confidence interval (CL)=
In this section, we assess the prevalence of VA anomalies according to data from CT Angiography of patients who referred to the neurology team with signs and symptoms of PICA stroke. Initially, we studied the frequency of each variation followed by assessing the correlations between each anomaly. In the final analysis, 125 patients (53.6
Our findings revealed that approximately 42% of patients had at least one VA variation with a male preponderance. Co-dominance was the most commonly observed dominance. Among the variations, hypoplasia and significant stenosis were the most prevalent anomalies.
With advances in interventional radiology and surgical methods in the neck, a thorough knowledge of VA's anatomical variations regarding its origin, course, and branches is crucial to minimize procedure-related complications [14]. Although colour Doppler ultrasonography has been traditionally considered the primary diagnostic modality in VA variations, CTA and MR angiography more accurately depict these variations and anomalies [15]. Coexisting intracerebral abnormalities in patients with VA variations should be investigated and vice versa, particularly in patients who experience cerebrovascular accidents [15].
Regarding dominance, the right outnumbered the left in our study. Our findings echoed those documented in previous studies, in which right and left dominance were observed in 45% and 30%, respectively [1]. Some studies hypothesize that the VA's origin and diameter differences may result in cerebral disorders because of the altered cerebral haemodynamic [16]. Originating from the left aortic arch was observed in 3.2% of participants in this study. A left VA of aortic origin is correlated with a predilection for dissection, presumably due to the vessel's longer course in the neck [17]. This could also be attributed to congenital defects in the structural arterial wall and cerebral haemodynamic changes [15]. Our findings are consistent with previous studies that also reported a greater incidence of VA variation in males [17].
Significant origin stenosis was detected in approximately 18% of our patients. A stenotic VA origin is principally associated with arterial thromboembolism and hypoperfusion. These patients generally have coexisting atherosclerotic stenosis in both carotid and renal arteries [18]. A stenotic VA origin with the vessel's tortuousness of origin raises the probability of stent fracture during the placement procedure [19]. Posterior circulation stroke in about 5% of patients was linked to VA origin stenosis [20].
Regarding VA branching variations, PICA originated from V3 rather than V4 in 3.2% of our patients. After the VA enters the suboccipital region, meningeal branches emerge, and its terminal and largest branch - the PICA - is given off [2]. Extradural origins of VA, similar to our findings, were reported in about 4% of patients through previous studies [21]. PICA termination is widespread in cases of left VA origin from the aortic arch, and the extradural branches of VA should be taken into consideration [14].
The present study reveals that the VA variations, especially significant stenosis (23 cases) and hypoplasia (22 cases), are the two most common variations with significant stenosis occurring more than hypoplasia. It is important to differentiate between acquired narrowing and hypoplasia of the VA because each of these has a different atherosclerotic burden [7].
In conclusion, our study shows that stenosis is more frequent than hypoplasia, so the former could be the most acquired and preventable factor of stroke. Besides, anatomical variations, including origin and branching, should be seriously considered in surgical or interventional radiology procedures to minimize the complications.
Vertebral Artery (VA)
Computed Tomography Angiography, CT-Angiography (CTA)
Anterior Inferior Cerebellar Artery (AICA)
Posterior Inferior Cerebellar Artery (PICA)
Subclavian Common Artery (SCA)
Standard Deviation (SD)
Confidence Interval (CI)
Posterior Cerebellar Stroke (PCS)
Ethics approval and consent to participate
Ethical approval for this Study and use of patients three-dimensional computed tomography angiography (CTA) images for collection and study was obtained originally from the local ethics committee in Shahid Beheshti university of medical sciences, Tehran, Iran. The Iran National Committee for Ethics in Biomedical Research approved continuing this study.
We conducted this study using data and CTA images from Tooska Medical Imaging center. All study participants provided written informed consent for studying their images. Patients explained regarding how their clinical data would be used in the study process. The patients' information remained confidential and identities were anonymous.
Consent for publication
All images were performed in accordance with the relevant guidelines and regulations and written informed consent for studying and publication was obtained from all patients.
Availability of data and material
The computed tomography angiography (CTA) raw data generated and analyzed during the current study are available in the Dr Sofia Saburi repository, Radiologist and main director of imaging center.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
None
Authors' contributions
This work was able to be completed due to the substantial contribution of the authors. All authors have contributed to the preparation and writing of the paper. All authors have read and approved the manuscript. Farzaneh Mohammadi: Conceptualization, Writing-Original draft preparation, Writing- Reviewing and Editing, Hussein Soleimantabar: design of the work, supervising and editing, Fatemeh Mohamadi: Methodology, interpretation of data, Sofia Sabouri: Reviewing and Editing, data availability.
Authors confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the authorship criteria. Authors further confirm their unanimous approval of the order of the authors listed in the manuscript. Additionally, the authors declare that this manuscript is original, has not been published before, and is not currently being considered for publication elsewhere.
Acknowledgements
Not Applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
