
Case Report | DOI: https://doi.org/10.31579/2768-2757/063
1 Parveen Kumar, M. Ch, Department of Pediatric Surgery, Chacha Nehru Bal Chikitsalya, New Delhi-110031, India.
2 Manika Boipai, M. Ch, Department of Pediatric Surgery, Chacha Nehru Bal Chikitsalya, New Delhi-110031, India.
3 Vivek Manchanda, M. Ch, Department of Pediatric Surgery, Chacha Nehru Bal Chikitsalya, New Delhi-110031, India.
4 Mamta Sengar, M. Ch, Department of Pediatric Surgery, Chacha Nehru Bal Chikitsalya, New Delhi-110031, India.
5 Natasha Gupta, M.D., Department of Radiology, Chacha Nehru Bal Chikitsalya, New Delhi-110031, India.
*Corresponding Author: Parveen Kumar, M. Ch, Department of Pediatric Surgery, Chacha Nehru Bal Chikitsalya, New Delhi-110031, India.
Citation: Kumar P., Boipai M., Manchanda V., Sengar M., Gupta N., (2023), The Umbilico-Bilious Fistula: A Diagnostic Challenge. Journal of Clinical Surgery and Research, 4(1); DOI:10.31579/2768-2757/063
Copyright: © 2023, Parveen Kumar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 December 2022 | Accepted: 06 January 2023 | Published: 30 January 2023
Keywords: heart failure; morbidity; mortality; perioperative risk; surgery
Background: Hepato-biliary system is known for congenital variations. An acquired entity secondary to a pathology/infection is a rare phenomenon.
Case: A 3 months old baby presented with bilious leak from peritoneum secondary to complicated umbilical sepsis. On further work up, a fistulous communication was found between umbilical ligament and biliary tree.
Conclusion: Umbilico-bilious fistulization is a rare presentation of umbilical sepsis. It should be kept in mind while dealing with umbilical sepsis cases.
Anatomical variations in the anatomy of the liver are common. The variations in arterial supply to the liver are most frequent among these, but biliary system developmental variations are also common. We present here a rare case of umbilico-bilious fistula encountered in an infant with umbilical sepsis, which was confirmed by contrast study and the difficulties encountered in diagnosis and management.
A 3 months old male baby presented to emergency with denuded supra-umbilical skin and greenish discharge for 1 day. There was history of swelling and redness just above the umbilicus for one week. There was no history of fever or vomiting. Baby had decreased breast feeding for 2 days. History of umbilical swelling since birth and reducing at own was elicited, most likely suggesting umbilical hernia. Baby was admitted in a private hospital for 1 month post birth for preterm gestation and low birth weight. Mother was on anti-tubercular treatment for pulmonary tuberculosis. At presentation, baby was 1.95 kg in weight. On examination, baby was dehydrated with heart rate of 157/min, respiratory rate of 28/min and capillary refill time of > 3 seconds. Icteric tinge was present. Per abdomen examination had denuded supra-umbilical skin, exposing the underlying bowel with bile staining. Baby had an ultrasound outside whose report mentioned of umbilical hernia and thrombosis of portal and umbilical vein. After fluid resuscitation, USG at our center revealed normal liver and gall bladder with multiple tortuous vessels in region of portal vein and heterogenous echogenic area around 1x1 cm near portal vein and traversing towards anterior abdominal wall abutting skin upto umbilical area. Mild free fluid was noted in peritoneal cavity. Routine investigations at admission revealed hemoglobin of 9.7 g/dl, total leucocyte counts of 37300/uL and platelets of 3 lakhs/uL. C-reactive protein levels were 113 mg/L. The total bilirubin levels were 9.04 mg/dl with direct component of 4.81. International normalized ratio was 1.2. In view of sepsis, piperacillin tazobactum was started (broad spectrum). The baby was taken for emergency exploratory laparotomy with suspicion of bowel/ biliary tract perforation in view of biliary disharge. On exploration, whole bowel was intact with some bile staining near the lesser sac. On further search, the falciform ligament was found to have a tract with rent near the hepatic surface and clear bile discharge. [Figure 1] A 6-Fr Foley catheter was inserted into the tract for future contrast study, which revealed communication to the biliary tree. [Figure 2] The tract was ligated in a second surgery (for burst abdomen). Sadly, the baby succumbed to sepsis.
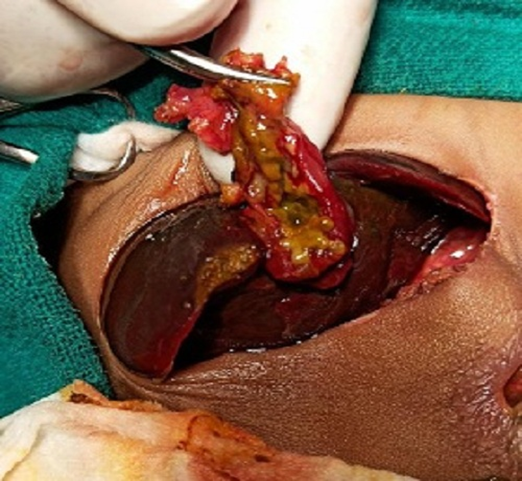
Figure 1: Intra-operative picture of bilious discharge from the umbilical ligament.

Figure 2: The contrast study showing fistulous communication with the biliary tree.
Liver develops as ventral hepatic bud from foregut. The endodermal cells of bud invades septum transversum and form hepatoblasts sheets. The hepatoblasts and mesenchyme cells form biliary tree. The hepato-biliary system is known for variations from normal anatomy. These variations arise from aberrations in embroyological development. Most of these involve extra-hepatic system, but cases are reported in literature for internal communication to other systems like respiratory or gastro-intestinal [1,2,3]. The aberrant duct opening into left triangular ligament has also been reported [4]. The index case presented as biliary peritonitis post denudation of umbilical skin after umbilical sepsis. The bile leak was from falciform ligament at liver surface. It may have been a congenital umbilico-bilious fistula, which got burst into the peritoneum via umbilical ligament or an inflammatory reaction of ligament caused secondary infection/ inflammation leading to fistulization. Only one such case is reported in the literature [5].
Umbilico-bilious fistulization is a rare presentation of umbilical sepsis. It should be kept in mind while dealing with umbilical sepsis cases.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
