
Review Article | DOI: https://doi.org/10.31579/2694-0248/040
1 KS Hegde Medical Academy, P.O. Nityanandanagar, Deralakatte, Mangaluru, Karnataka 575018, India.
2 Asian Institute of Arthroscopy Sports Injuries and Research Pvt. Ltd. 31/32 Cresent Road, Near Shivananda Circle, Bangalore 560001, India.
*Corresponding Author: Siddhartha M. Shetty, KS Hegde Medical Academy, P.O. Nityanandanagar, Deralakatte, Mangaluru, Karnataka 575018, India. Email: drshettybs@gmail.com
Citation: Siddhartha M. Shetty and Hemanth K. R. Alladu. (2022). The Sironix ACL Jig: A Solution for Tibial Tunnel Angle and Length. J Clinical Orthopaedics and Trauma Care, 4(4); DOI:10.31579/2694-0248/040
Copyright: © 2022, Siddhartha M. Shetty. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 June 2022 | Accepted: 23 June 2022 | Published: 04 July 2022
Keywords: anterior cruciate ligament; ACL jig; graft fixation; tibial; femoral tunnel placement
Anterior cruciate ligament (ACL) reconstruction is widely performed arthroscopic procedures amongst sportspersons to prevent worsening of knee joint injury. The Sironix ACL jig is a novel approach to ensure an appropriate angle for accurate placement and drilling of tibial and femoral tunnels, that is a critical step for stronger and stable ACL graft fixation. It is designed as a patented jig with a three-point arm contact system. The three reference points serve as a continuous visual feedback on the angle of approach during surgery and minimize the parallax errors. Sironix ACL jig helps the orthopaedic surgeon in deciding the feasibility of a single bundle or double bundle ACL technique, facilitates varying technique choices for drilling, including inside-out and outside-in, accurately determines the tibial and femoral tunnel positioning in arthroscopic or open ACL reconstruction and therefore increases the procedural convenience.
Anterior cruciate ligament (ACL) reconstruction is one of the most commonly performed arthroscopic procedures to prevent worsening of knee joint injury and restore knee stability [1]. Injury of ACL is mostly witnessed by sportspersons during brisk movements (jumping, sudden directional change, pivoting and sudden stop). However, in few cases, the patient may develop major local edema with joint effusion caused by massive hemarthrosis after several hours of resuming normal activities [2]. Complete ACL ruptures can result in circumstances that induce clinical symptoms of knee instability, such as meniscal tears, articular cartilage degradation, and greater stress on other soft tissues [3]. Without surgical reconstruction, ACL deficiency can lead to degenerative changes in knee joints. Need for ACL reconstruction is continuously increasing among sportspersons as quick rehabilitation and recovery is essential for their return to sports.
ACL reconstruction commonly employs single-bundle, double-bundle, and selective single-bundle augmentation procedures. Given the benefit of direct visibility with arthroscopic methods, the chance of both the bone tunnels and the ACL itself being physically repaired is extremely high [4]. Anatomic ACL reconstruction aims to restore knee kinematics and improve patient short and long-term outcomes by closely replicating the patient's individual anatomic characteristics [5]. More anatomically placed tibial and femoral tunnels gives the knee more stability and improves functional outcomes [6].
1.1 Importance of precise graft placement
The precise placement of an ACL graft is critical for a good result following restoration. Incorrect tunnel placement can result in aberrant graft tension, loss of mobility, and recurring instability, and thus graft failure [7]. The angle of tibial tunnel implantation in the coronal plane is also necessary for avoiding posterior cruciate ligament impingement and postoperative flexion loss. Abnormalities might emerge if there are deviations of tunnel positioning from the optimal location. When the femoral tunnel is placed too shallow or too high placement of the femoral tunnel will result in graft to be tight in flexion. The graft may overstretch in extension if the tunnel is placed too high, thereby reducing range of motion. If the tibial tunnel location is sufficiently anterior, the ACL may be pathologically impinged onto the notch roof, resulting in extension deficiency. On the other hand, sustained instability may occur if the tibial tunnel location is excessively posterior and rotational instability may occur in case tibial and femoral tunnels are overly steep [8]. An audit study demonstrated incorrect positioning of 65% of femoral tunnels and 59% of tibial tunnels in the sagittal plane [9]. Another study showed that the femoral and tibial tunnels were appropriately positioned in only half of the patients undergoing ACL reconstruction by surgeons with different levels of experience (that was determined by the total amount of ACL replacements done before) [10]. Howell et al. observed that a coronal plane angle greater than 75° was related with loss of flexion and increased laxity [11]. Despite employing anatomic landmarks to position the tibial tube (such as 67.56° angle of tibial tunnel in 80% of cases), radiographic impingement ranging from 1% to 100% was identified in 34% of the patients [12]. Traditional transtibial ACL restoration fails to precisely align femoral and tibial tunnels inside the natural ACL insertion site as visualized by 3D computed tomography scans [4].
1.2 Utility of Jigs
Constant anatomic landmarks that can be used as definitive reference points have not been described till date, which makes this technique difficult. So the understanding of the correct tunnel positioning is of paramount importance [13]. Current ACL reconstructions are mainly focused on the restoration of anatomical structures using arthroscopic techniques under reliable landmarks. However, reliable landmarks in ACL tunnel positioning may have variable anatomy inducing a misplacement of tibial tunnel. Furthermore, Shafizadeh et al. have indicated that, even if ACL reconstruction is performed by experienced arthroscopic surgeons and anatomic variation is not considered within the same knee condition, there is still a great variability in tibial tunnel placement [14]. Several studies have found that ACL jig helps in accurate positioning and drilling of tibial and femoral tunnels [15-17]. They are quick and accurate to determine the precise points of tunnels for entry and exit and can efficiently control the tunnel's depth [18].
The tibial jig has also proved to be useful in talar fractures or Lisfranc’s injuries where freehand K-wire and screw fixation is difficult to use, as described by a previous study by Sharma et al. The study also mentioned the application of tibial jig in hallux metatarsophalangeal joint fusion (19). A recent study demonstrated the applicability of jig in surgical repair of extensor tendon ruptures (18). Despite these benefits, most of the currently available jigs have either a single or two teeth hook [19]. which may lead to a high chance of misalignment in all the three axis and hence, leads to inaccurate insertion of the drill pin.
2.0 A new Sironix ACL Jig (US Patent No. US D843,570 S)
Sironix, a division of Healthium, has developed an advanced ACL jig as a novel approach that ensures appropriate angle for accurate tibial tunnel drilling, that is a critical step for stronger and stable ACL graft fixation. The design for the arthroscopic jig has been patented on March 2019 under US Patent No. US D843,570 S. This Sironix ACL jig features the unique patented 3-point contact design which not only helps to ensure anatomic placement, but also delivers the most accurate angle and length of tibial tunnel, thereby allowing the surgeon to visualize the tunnel with accurate tibia connect (Figure 1).
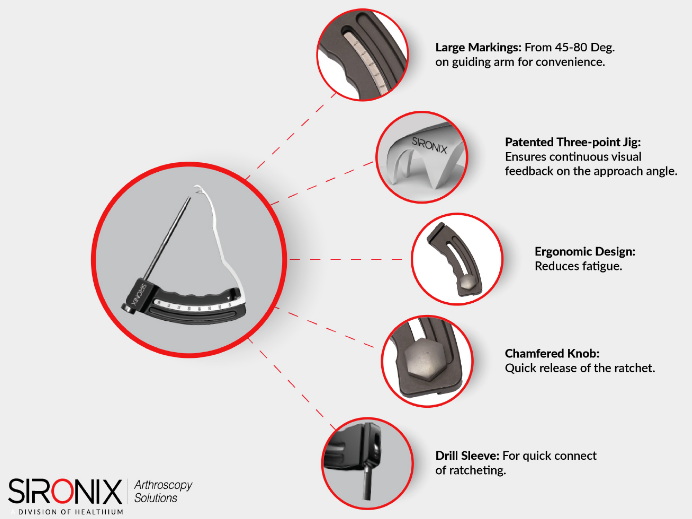
Figure 1. Features of the Sironix ACL Jig
2.0 A new Sironix ACL Jig (US Patent No. US D843,570 S)
Sironix, a division of Healthium, has developed an advanced ACL jig as a novel approach that ensures appropriate angle for accurate tibial tunnel drilling, that is a critical step for stronger and stable ACL graft fixation. The design for the arthroscopic jig has been patented on March 2019 under US Patent No. US D843,570 S. This Sironix ACL jig features the unique patented 3-point contact design which not only helps to ensure anatomic placement, but also delivers the most accurate angle and length of tibial tunnel, thereby allowing the surgeon to visualize the tunnel with accurate tibia connect (Figure 1).

Figure 1. Features of the Sironix ACL Jig
2.1 The three-point jig ensures continuous visual feedback on the approach angle
Ensuring anatomic placement of the ACL jig is vital. The tibial tunnel angle influences the success of graft fixation in ACL reconstruction (20). The Sironix ACL jig is designed as a patented three-point jig to have a better grip at the tibial surface on the ACL footprint though the distal tip. During surgery, the three reference points serve as a continuous visual feedback on the angle of approach. The triple contact points ensure that the approach angle stays correct in X, Y and Z axes (Figure 2) that helps in accurate insertion of the drill pin at the desired angle and minimizing the parallax errors.
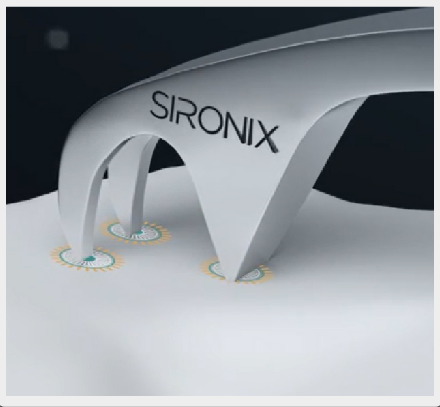
Figure 2. The three-point arm contact system of the Sironix ACL jig
The ergonomically designed grip and the uniformly distributed weight make the jig stable and decreases fatigue. The bullet uses a ratchet mechanism for locking, which makes it easy to stabilize and operate. The markings on guiding arm make setting the approach angle easier and quicker. The thumb knob has been designed for quick release and its serrations provide an additional grip.
Sironix ACL jig therefore acts as a template and aids the surgeon in visualizing the tunnels before committing to a location or size. The Sironix ACL jig also helps the orthopaedic surgeon in deciding the feasibility of a single bundle or double bundle ACL technique, thereby addressing the differences in size of the native ACL. The ideal candidates for double bundle surgery are patients with a tibial insertion site size of >16 mm, thereby making sure that the surgery reproduces most of the native ACL footprint. Sironix ACL Jig has been aptly designed to be used via the lateral portal. Consequently, the surgeons are able to insert their scope into the middle portal while marking and drilling the tibial & femoral tunnel, the jig also helps in visualizing the native ACL insertion site anatomy on the tibia & femur in a better way (Figure 3 a, b and c).
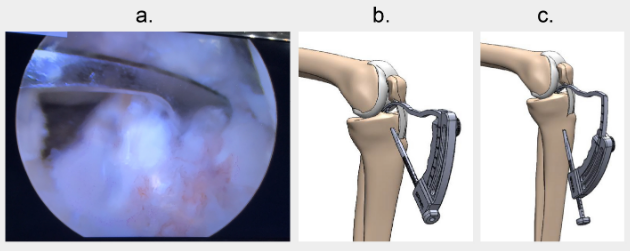
Figure 3. Image showing (a) anatomic placement of Sironix ACL jig during arthroscopy (b) Sironix ACL jig placed at tibial tunnel angle of 40° and (c) Sironix ACL jig placed at tibial tunnel angle of 65°.
Sironix ACL jig easily allows the instruments to reach the most posterior and proximal part of the lateral notch, where the ACL attachment lies. Accurate estimation of the size of the insertion site anatomy before drilling is vital and the Sironix ACL jig aids the surgeon in determining the tibial and femoral tunnel placement. To achieve an ideal anatomic tibial and femoral tunnel placement, consideration of the relative position of the anteromedial (AM) and posterolateral (PL) bundles is important and the ACL jig has been optimally designed to insert screws at desirable angles between 45 to 80 degrees. The length of bore at different jig angles are summarized in (Table 1).
| Jig angle (degree) | Length of bore (mm) |
| 40◦ | 25.54 |
| 45◦ | 26.21 |
| 50◦ | 27.67 |
| 55◦ | 30.32 |
| 60◦ | 32.62 |
| 65◦ | 38.12 |
Table 1: Length of the bore with respect to different jig angles
2.2 Large markings: 45 to 80 degrees on guide arm for convenience
Sironix ACL jig has large markings between 45 to 80 degrees on guide arm for convenience. To allow the surgeons to estimate how much of the native ACL tibial and femoral footprint the graft(s) will cover, depth markings are provided on each guide and different size templates (Figure 4).
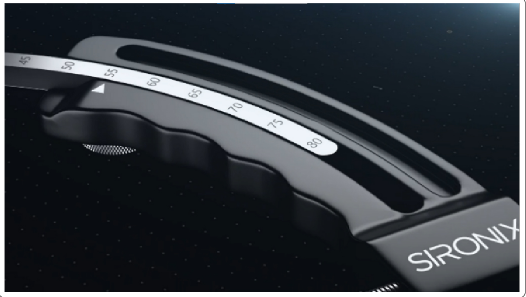
Figure 4. Guide arm of Sironix ACL jig with large markings
When the ACL tibial and femoral footprint is small, there is a risk of damage to the attachment site of the anterior horn of the lateral meniscus when performing a reconstruction with a large bone tunnel at the centre.
The Sironix ACL jig is a guide used for positioning the tibial and femoral tunnel in arthroscopic or open ACL reconstruction. The Sironix ACL jig includes a guide arm and a drill sleeve connected to the guide arm (Figure 5).

Figure 5. Image showing Sironix ACL jig with the drill sleeve connected to the guide arm
The guide arm of this Sironix ACL jig may be oriented desirably by adjusting the guide arm with respect to the drill sleeve. There are markings on the guide arm to indicate the optimum orientation of the guide arm with respect to the drill sleeve.
2.3 Drill Sleeve
Sironix ACl jig has a drill sleeve that is attached for quick and easy deployment of the blade by simply switching power on the drill from forward to reverse. The blade deploys once it contacts bone in a reverse setting.
The unique patented three-point contact design of Sironix ACL jig has addressed some of the key challenges associated with anatomic placement and ACL reconstruction due to size variability of the native insertion sites on the femur and tibia. The Sironix ACL jig offers accuracy, manoeuvrability, ease of use and offers the following advantages over other existing ACL Jigs:
• Accurately drills tunnels and bone socket for anatomic reconstructions. Precise positioning, placement and drilling of tibial and femoral tunnels in an imitable and accurate fashion can be ensured using Sironix ACL Jig.
• Avoids the requirement for bony landmarks for tunnel placement.
• System components are appropriately assessed for both bone-tendon-bone and soft tissue grafts.
• Quick and easy deployment of the blade by simply switching power on the drill from forward to reverse.
• Facilitates the placement of AM and PL bundles along with varying technique choices for drilling, including inside-out and outside-in.
• Point to point tibial and femoral guide increases the procedural convenience.
The authors thank WorkSure® India to provide assistance in preparation of the manuscript.
On behalf of all authors, the corresponding author states that there is no conflict of interest.
ACL: Anterior cruciate ligament; AM: anteromedial; PL: posterolateral
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
