
Review Article | DOI: https://doi.org/10.31579/2639-4162/155
1Dept. of Oncology, Barzilai Medical Center, Ashkelon, Israel.
2Orthopedic oncology unit, University hospitalof Padova, Padova,Italy.
3Faculty of Medicin, Oradea, Romania.
4Dept. of Radiation Therapy,MVZ Inn Med Clinic, Oberaudorf, Germany.
5Faculty of Health Sciences,Ben Gurion University of the Negev, Beer Sheba, Israel.
6Dept. of Urology, Barzilai Medical Center, Ashkelon, Israel.
7Dept. of Pathology, Barzilai Medical Center, Ashkelon, Israel.
8Sackler medical School, Tel Aviv University, Tel Aviv, Israel.
9LaserCenter, Ludwig Maximilian University, Munich, Germany.
θThe first and the second authors equally contributed and considered as first authors.
*Corresponding Author: Ron Batash, Orthopedic Oncology unit, University hospital of Padova, Padova, Italy.
Citation: Moshe Schaffer, Ron Batash, Pamella M. Schaffer, Murad Asali, Tom Zuckerman, et al, (2024), The Role of Photosensitizers as Radiosensitizers in Cancer Treatment, J. General Medicine and Clinical Practice, 7(5); DOI:10.31579/2639-4162/155
Copyright: © 2024, Ron Batash. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 02 March 2024 | Accepted: 11 March 2024 | Published: 26 March 2024
Keywords: photosensitizers; radiosensitizers; radiotherapy; cancer therapy; cancer relapse
Enhanced cancer resistance to treatment is associated with various mechanisms. However, cancer may frequently relapse after some time. Several strategies have emerged over the last few years to halt this process - improving cancer therapy, including - chemotherapy, radiotherapy, immunotherapy, surgery, targeted therapy, hormone therapy, stem cell transplant, and precision medicine. Among those strategies, Radiotherapy (RT) is an essential modality to treat tumors and control their growth. Tumors can withstand more ionizing radiation than normal tissue. However, the addition of radiosensitizers can adjust the effect of the radiation on tumors tissues, causing significant damage to the neoplastic tissue. PDT (photodynamic therapy) was considered a promising treatment for early and localized inoperable tumors. This work provides combination therapy comprising a radio sensitizing agent and radiation therapy, describing its effectiveness in inhibiting the proliferation of cancer cells and cancer stem cells, including mechanism of function (partially known) and the possibility of using this method as a kind of targeting therapy.
New challenges in cancer therapy have emerged recently, considering enhanced resistance to conventional treatment of various cancer types. Moreover, high incidences of relapse after primary cancer regression contribute to the problem. Enhanced cancer resistance to treatment is associated with multiple mechanisms, including mutations and drug over- expression of the drug-target. Other mechanisms involve drug termination from the cells or inactivation of the drug. Several strategies have been attempted over the last few years, in order to improve cancer therapy and reduce mortality. The methods include - radiotherapy, immunotherapy, surgery, targeted therapy, hormone therapy, stem cell transplant and precision medicine. Among these strategies, Radiotherapy (RT) is an essential modality to treat tumors and hinder their growth [1-3]. As widely described in the literature, cancer lesions are comprised of a heterogeneous population of cells, which include numerous types. This may be one of the causes for failure of treatment and cancer relapse. Several cancer resistance and recurrence models have been associated with small populations of identified cancer stem cells. For instance, malignancies of hematopoietic origin and some solid cancers. Such cells are also considered cancer stem cells (CSCs) or cancer-initiating cells. These cells have self- renewal capabilities and therefore, are a fundamental concept in tumor biology4,5. Their ability to initiate tumor growth granted them the name - “tumor-initiating cells” (TICs)5. Tumor-initiating cells are phenotypically different from their fellow tumor cells, since they express explicit markers and functional features, such as resistance to conventional therapy [6-8]. TIC express organ-specific markers and characteristics that separate them from differentiated cells, e.g., expression of active DNA repair ability, expression of specific ABC drug transporters and disinclination to apoptosis signals. In clinical terms, the stem cell model for relapse may be highly suitable for chemotherapy responding cancers with a complete response, that relapse months or years later [9,10]. One explanation for the failure of conventional cancer therapy might be the presence of CTC, reflecting the need to identify new therapies to target those cells. Currently, there are various modalities for treating cancer, including a combination of radiation and a radio- sensitizing agent, which have been shown to enhance therapy [4,5,9-11]. Several radiosensitizers were depicted, partly in clinical use and partly experimental, such as small molecules and various chemotherapies, e.g., oxygen, oxygen mimics, hypoxia-specific cytotoxins, cisplatin, 5FU, nanoparticles, and photosensitizers. While considered high for tumors compared to normal tissue, the ability to withstand ionizing radiation can be adjusted by computer-controlled irradiation protocols with different radiation frequencies. [9,10,12-14].
Moreover, the tumor tissue selection to radiation is enhanced by radiosensitizers; which can be used to achieve a more significant rate of deterioration of the neoplastic tissue, as opposed to the additive effect of each modality [9,10]. When using radiosensitizers, one must consider two main parameters: possible complications of use and the therapeutic ratio - the likelihood of local tumor control. Most of the commonly utilized radiosensitizers are not tumor-specific and have poor selectivity. Usage of such compounds can potentially lead to severe complications as a result of their toxicity. Hence, an ongoing search for specific radiosensitizers has begun, as a means to improving the outcome of radiation therapy on relatively radio-resistant hypoxic tumor cells9,10
PDT (photodynamic therapy) was estimated to have promising results in treating early and localized inoperable tumors in the 1980s [15,16]. The technique involves a topical or systemic administration of a photosensitizer and the exposure of the tumors to a specific wavelength absorbed by the photosensitizer [15,16].
Due to their tetrapyrrolic macrocycle, the preferred photosensitizers are the porphyrins, and their equivalents, with absorption bands in the 600-800 nm wavelength (the red region of the visible spectrum) that enables high penetration into human tissue [8,16,17].
The PDT effects result from a reaction between the photosensitizer's initially formed excited singlet state and the photosensitizer's lowest triplet state, having an intersystem crossing [15-17]. Consequently, this triplet photosensitizer and the biological targets can interact with the transfer of electron or proton, generating the construction of radical particles that in turn, form oxidized products after interaction with oxygen – a process known as type I reaction [18-20].
Alternatively, the energy from the metabolite might be transferred to molecular oxygen directly, causing singlet oxygen to form. The singlet oxygen is cytotoxic, and the mechanism is called a type II reaction19. In both types of reactions, the presence of oxygen is crucial21,22. In contrast to ionizing radiation, which primarily targets cellular DNA, PDT is known to affect cellular membranes, blood vessels and mitochondria [16,23].
This paper aims to review the use of photosensitizers as selective and specific radiosensitizers. Due to the fact that there is a vast number of existing Photosensitizers, which can be used as radiosensitizers, we tried to focus mainly on main photo-radio-sensitizers. We are presenting a combination therapy technique, comprising of radio sensitizing agent and radiation therapy, which effectively inhibits the proliferation of cancer cells and cancer stem cells.
Photosensitizer as Radiosensitizer in Vitro and in Vivo
Photosensitizers' selectivity for tumor tissues encouraged the search for the potential use of compounds as radiosensitizers. In 1955 Schwartz et al. conducted experiments showing the radio sensitizing effects of porphyrins in patients taking HpD with radiation therapy [24,25].
The experiment showed enhanced local tumor control in patients with carcinoid tumors, fibrosarcoma, squamous cell carcinoma, and rhabdomyosarcoma [24]. In his publication, the side effects mentioned were vomiting, nausea, and remarked skin photosensitivity that lasted for several months [24]. The metabolic product is HpD, a highly heterogeneous Hp chemical derivative in a chemical reaction between acetic and sulfuric acid with hematoporphyrin. One of the partly purified forms of HpD is Photofrin II [24]. In 1960, Schwartz and Cohen demonstrated that higher doses of hematoporphyrin copper complex facilitate radioprotection, in contrast to smaller amounts, which showed a noticeable radio sensitizing effect. In 1986, Kostron et al. managed to reduce 40% of rat glioma tumor growth compared to the control group, which confirmed the radio sensitizing potential of HpD (Hemato-porphyrine derivative) [26]. One of the derivatives of perylenequinonea product of the plant Hypericum perforatum, which is used for treatment, is the red-colored Hypericin (St. John's wort) [27].
Hypericin and its derivatives have been studied for their physicochemical properties, e.g., electron transfer, singlet-oxygen sensitization, and excited- state proton transfer [28,29]. Moreover, Hypericin is an antidepressant, antiviral agent, and potent protein kinase C inhibitor, enabling tumor selectivity and specificity in photodynamic therapy [30,31]. This fact led to further studies of Hypericin as a diagnostic tool in several cancers, which induced apoptosis in tumor cells [30-33].
A study published in 2015 by Schaffer et al. [34] showed that perylenequinone derivatives (PDs) acted as potent radiosensitizers. This group proved the effects of some derivatives of Hyperecin (PDs) on tumor- initiating cells (TICs) and normal tumor cells [34]. TICs are phenotypically different from other tumor cells due to the expression of specific markers and stem functional cell characteristics, which enable resistance to conventional therapy [8,35,36]. In their study, the group checked TIC cells of PANC1 (pancreas cancer), U87 (glioblastoma), HT29 (colon cancer), MCF7 (breast cancer), A549 (lung cancer) tumor cell lines. Cells in culture were given 0.1- 2M of Hypericin tetrasulfonate (HyTS), Tetrabromo hypericin (TBrHy,) or PDs Hypericin (Hy), followed by illumination with fractionated daily dose or single high dose of radiation, then, the cell viability was assessed. Additionally, the researchers assessed the tumor development of PANC1 and U87 cells in subsequently injected PDs mice and illuminated with local ionizing radiation.
Their final findings indicated that PDs expressively hindered the viability of the tumor cells exposed to radiation and grown in the TIC-enriched culture. Furthermore, TBrHy considerably stalled PANC1 and U87 tumor development in mice exposed to high levels of radiation. These findings showed that TIC viability might be used to assess radio sensitizing activity. Therefore, PDs might be considered adequate radiosensitizers, which can mark tumor cells and TICs, underlining substantial therapeutic value [34].
Photofrin II, which is made of porphyrins, synthesized by treating heorphyrin (Hp) with acid, represents one of the backbones of clinical PDT [37]. In 2001, Schaffer et al. aimed to improve the application of Photofrin II as a radiosensitizer in ionizing radiation [38,39]. In one of the studies, human cell bladder cancer (RT4) implanted mice [40] exhibited a nearly 50% reduction in tumor growth after 12 days and X-ray irradiation (5 Gy) 24 hours after injection of Photofrin II. Compared to 5-ALA, chlorin e6, Hp, and Zn- tetrasulfophtalocyanine, Photofrin II was the only photosensitizer that showed a significant change - “doubling time” of the tumor, that changed from 6.2 days to 10.9 days. However, the mechanism responsible for the positive effect remains vague due to Photofrin's heterogeneous composition. While 5-ALA with X-ray irradiation (3 Gy) was inefficient in mice with Lewis’s sarcoma tumors implanted in them, Photofrin led to a nearly 40

Results are shown in Table 2
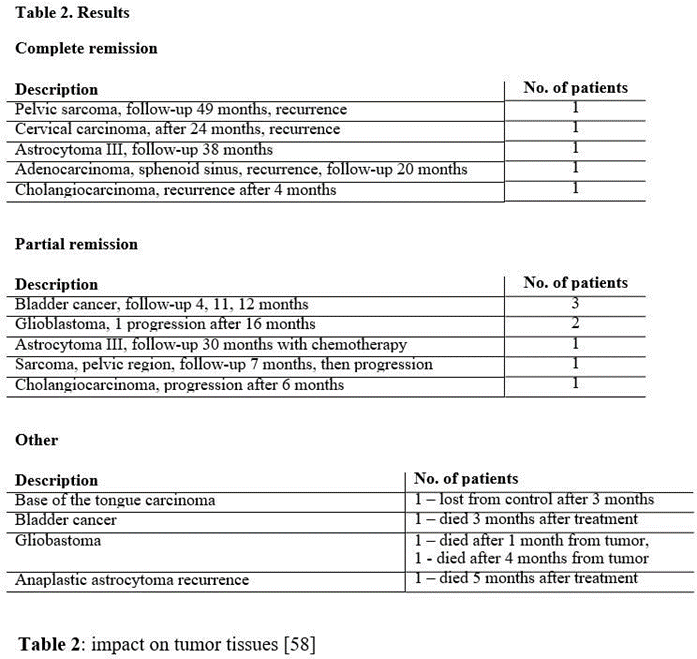
[58]. Due to the light sensibility by photosensitizers, especially photofrin II, the patients were protected from light during their treatment for a period of 3-4 weeks. All lights indoors were limited with lamps of 40W. Two of these patients with advanced tumors, one female with Astrocytoma Grade III and another female with Cervix Carcinoma FIGO IIIb, are still alive and currently free of disease [60,61].
The literature review and demonstrated results illustrate that PS might be utilized as a radio sensitizing agent in the right circumstances. While PS on its own showed no noticeable tumor response in concentrations that presenteda marked radio sensitizing effect, the radiosensitizing effect it has can be confirmed in highly radio resistant tumor models, such as bladder carcinoma and glioblastoma [34,55,58,60,61].
As a general rule, radiosensitizers imitatethe effects of oxygen caused by free radicals in radiationtherapy. Nitroimidazole is the most common radiosensitizer evaluated in clinical studies. A significant drawback of this agent lies in its neurotoxicity, which prevented using an effectual dose with a standard daily fractionated radiation [54,62]. Other compounds, for example, Tirapazamine[63,64], bovine hemoglobin modified with polyethylene glycol (PEG)[65], and RSR [13,66], are currently in the clinical investigation for hypoxic tumor cells. The direct consequence of radiation (RT) is to cause double-strand breaks (DSB) and single-strand breaks (SSB) in DNA. The breaking of the DNA leads to the termination of cell divisionand cell proliferation, and in some cases, to cell necrosisand cell apoptosis. See figure1a.[24,25,26,34,38]
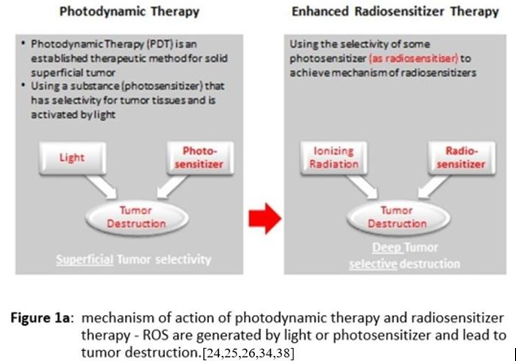
The indirect consequences of radiation lead to the generation of reactivity of Oxygen Radicals such as RO; ROS might cause cellular stress, induce biomolecules damage and eventually change the cellular signaling pathways. A number of studies demonstrated that 70% of the patients should be treated with controlled linear accelerators to carry the specific radiation quantities to the malignanttumor or the selected areas inside the tumor tissue [51,62,67,68].
Although these advanced developments increase the therapeutic results,hurdles still exist - cancer stem cells and tumor heterogeneity, limiting the use of RT alone as an ns of tumor eradication. However, by utilizing radiosensitizers that enhance the radiosensitivity of the tumor tissue and have toxicity within the range of pharmacologically normal tissue, one can apply RT more effectively and achieve the desired outcome [62,67,69].
When combined with radiation, radiosensitizers demonstrate higher tumor inactivation than predicted from the particular singular modalities [69,70]. The mechanisms of action of radiosensitizers can be classified into five different steps: (1) blocking the radioprotective effect of intracellular thiols or other endogenous substances; (2) generation of cytotoxic agents by radiosensitizer radiolysis; (3) inhibition of biomolecules repair; (4) thymine analogs incorporation into DNA; and (5) electrophilic activityof oxygen mimickers [9,70]. According to recently published studies, radiosensitizers can be categorized into three differentclasses, based on their molecularstructure: little molecules, e.g., oxygen Mimics [5,70],
macromolecules, e.g., Proteins and Peptides, and Oligonucleotides [67,68]. The last group is nanomaterials, e.g., metal and ferrite nanomaterials [69,70]. Junzhi Liu, et al. [70], found that acridine orange (AO), a small molecule radiosensitizer, can be loaded onto mMnO2 nanoparticles at very high efficiency and released to the surroundings in a controlled fashion. This review has focused on PS as radiosensitizers, which belongs to the second group. Not all commercially available PS evaluated can perform as a radiosensitizer. Furthermore, it appears to be utilizedonly as a photosensitizing agent [34,55].
As mentioned previously in this review, a number of hypotheses aim to showcase the PS radiosensitization of tumors: i) PS has a reaction with molecules that have been activated by cytotoxin, e.g., hydroxyl, radicals that are the productsof the interaction of X-raysand water [10,41,42,49,51,56]. PS reduces the chancesof starting repair processes that prevent radio- induced cell damage [41,50]. The damage that Ionizing irradiation causes split into two categories62: sublethaldamage and lethal damage. The sublethal damage might become lethal or excite the cell mechanisms of repair; the use of Photofrin might minimize the effects of those mechanisms if used in addition to ionizingradiation.
The radiosensitizing ability of PS is a subject of interest for several reasons, regardless of its actual course of action. PS is clinically approved in large amountsin Photodynamic Therapyof cancer. Hence, its use as a radiotherapeutic substance is derived from the ability to avoid, or at least significantly reduce expensive toxicological studies. PS has demonstrated no toxicity in humans at the doses used in radiotherapy [11,17,18,72] and showed certain selectivity of tumor targeting. This is stated in comparison to a number of radiosensitizers in clinical uses that have a much lower tumor targetingand demonstrate harsh side effectsin in vivo settings [15,62].
PS's ability to be utilized as a phototherapeutic and a radiotherapeutic substance provides extraordinary insights on its mechanisms, and enables superior regulation of tumor growth. However, various PS cause skin photosensitization (depends on the type of PS) that might hinder the use of this agent, while radiation therapy is considered. This is also true for the practice of boost irradiation, HDR following loading irradiation, brachytherapy, or only high precision radiation therapy [37-40]. The standard radiation dose in these modalities is ranged in ranges 2-16 Gy, which is administered to the tumor in a limited time and deprived of loco-regional irradiation. In vivo and vitro studies demonstrated that PS can be utilized in cases of tumor tissue hypoxia and can be considered an effectual radiosensitizer [7,37-41,55,56,73].
The combination of PS with a known contrast media - Gadolinium or with Manganese-dipyriddoxyl-5`diphosphate(Mn-DPDP – might be looked at in searchof diagnostic and treatment methods [71,74].
Conclusion
We believe that PS could potentially become a symbol for helpful agents in managing tumors and demonstrate: i) Better efficacy of radiation on the tumor alone, leaving the radiation effects on the neighboring tissues unchanged. ii) Enhancement of mechanisms that hinder hypoxic cells. iii) Minor toxicity in humans.
Moshe Schaffer and Ron Batash– initiated the study, contributed to its conception, design and writing of the manuscript.
Pamella Schaffer and Alfons Hofstetter designed and performed part of the experiments in the review.
Alejandro Livoff, Murad Asali and Tom Zuckermann contributed to the clinical data and review of the literature.
All authors reviewed and agreed on the manuscript.
All authors state that there are no conflicts of interest.
We wish to express our gratitude to Prof. Giulio Jori, who is considered among the leading pioneers in the field of radiosensitizers and photodynamic therapy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
