
Review Article | DOI: https://doi.org/10.31579/2578-8868/213
1 Department of Pharmacology and Toxicology, School of Pharmacy, Islamic Azad University, Tehran, Iran.
2 Department of Laboratory Hematology and Blood Bank, Shahid Beheshti University of Medical Science, Tehran, Iran.
3 Medical Genetics-Harvard University. Director of the Division of Medical Genetics and Molecular Optogenetic Research & Massachusetts Institute of Technology (MIT)
*Corresponding Author: Shahin Asadi, Medical Genetics-Harvard University. Director of the Division of Medical Genetics and Molecular Optogenetic Research & Massachusetts Institute of Technology (MIT)
Citation: Mahsa Hemati, Naser Shagerdi Esmaeli, Shahin Asadi. (2021) Effect of Ultrasound Guided Bilateral Greater Occipital Nerve Block on Serum Calcitonin Gene Related Peptide (CGRP) in Chronic Migraine. J. Neuroscience and Neurological Surgery. 10(1); DOI:10.31579/2578-8868/213
Copyright: © 2021 Shahin Asadi, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 11 October 2021 | Accepted: 28 October 2021 | Published: 02 November 2021
Keywords: lambert-eaton myasthenic syndrome (lems); genetic mutation; hla gene; autoimmune disorder
Lambert-Eaton myasthenic syndrome (LEMS) is a rare presynaptic disorder of neuromuscular transmission in which quantal release of acetylcholine (ACh) is impaired, causing a unique set of clinical characteristics, which include proximal muscle weakness, depressed tendon reflexes, posttetanic potentiation, and autonomic changes. [1] The initial presentation can be similar to that of myasthenia gravis (MG), but the progressions of the 2 diseases have some important differences.
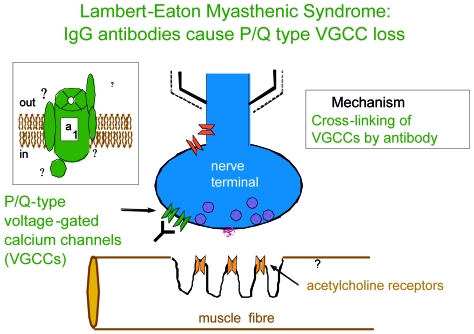
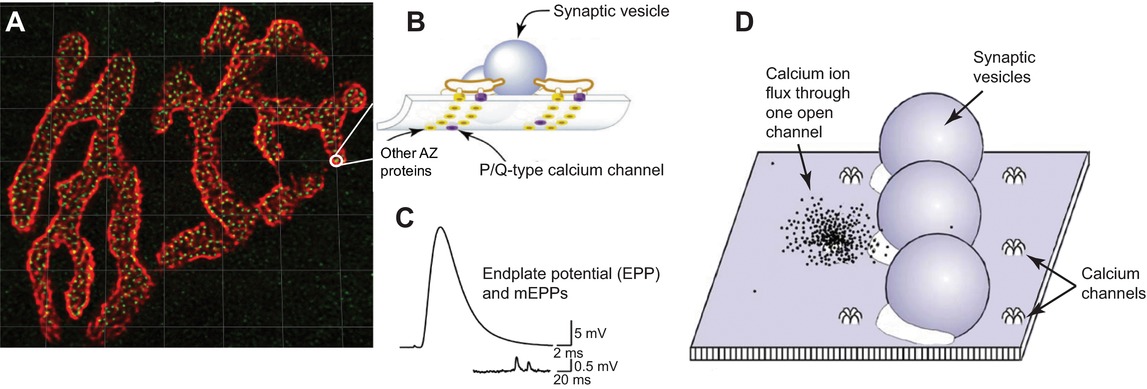
LEMS disrupts the normally reliable neurotransmission at the neuromuscular junction (NMJ). This disruption is thought to result from an autoantibody-mediated removal of a subset of the P/Q-type Ca2+ channels involved with neurotransmitter release.
LEMS syndrome is an autoimmune disorder of the neuromuscular junction. This is a false connection between the nerve cell and the muscle that leads to the gradual onset of muscle weakness. Symptoms of this syndrome begin in the proximal muscles of the legs or arms. LEMS can be classified into two distinct categories: small cell lung cancer-associated LEMS (SCLC) and cancer-free LEMS. Approximately 60% of patients with LEMS have SCLC, and the onset of LEMS symptoms often precedes the diagnosis of cancer. Patients with LEMS with cancer tend to get older - mostly men - and almost always have a long history of smoking. In patients with no accompanying cancer, the onset of the disease can be at any age and be gender neutral. LEMS may affect the quality of life of patients, depending on the severity of the symptoms [1].
Clinical Signs and Symptoms of Lambert-Eaton Myasthenic Syndrome (LEMS)
LEMS is characterized by weakness and fatigue, especially in the muscles of the legs and arms. It can affect a patient's ability to do strenuous exercise and can make activities such as climbing stairs or walking on a steep path difficult. It starts gradually and usually lasts for a few weeks to a few months. There are often symptoms that progressively affect the shoulder muscles, leg and arm muscles, speech and swallowing muscles, and eye muscles. Symptoms progress more rapidly when LEMS is associated with cancer. Most LEMS patients also show the following symptoms (sometimes called autonomic symptoms): dry mouth, dry eyes, constipation, impotence, and decreased sweating. LEMS patients with or without cancer may also experience significant weight loss. Tendon reflexes are reduced or absent on medical examination. Hence, in summary, LEMS is often described as a clinical "triple" of proximal muscle weakness, autoimmune symptoms, and decreased tendon reflexes [1].
Etiology of Lambert-Eaton Myasthenic Syndrome (LEMS)
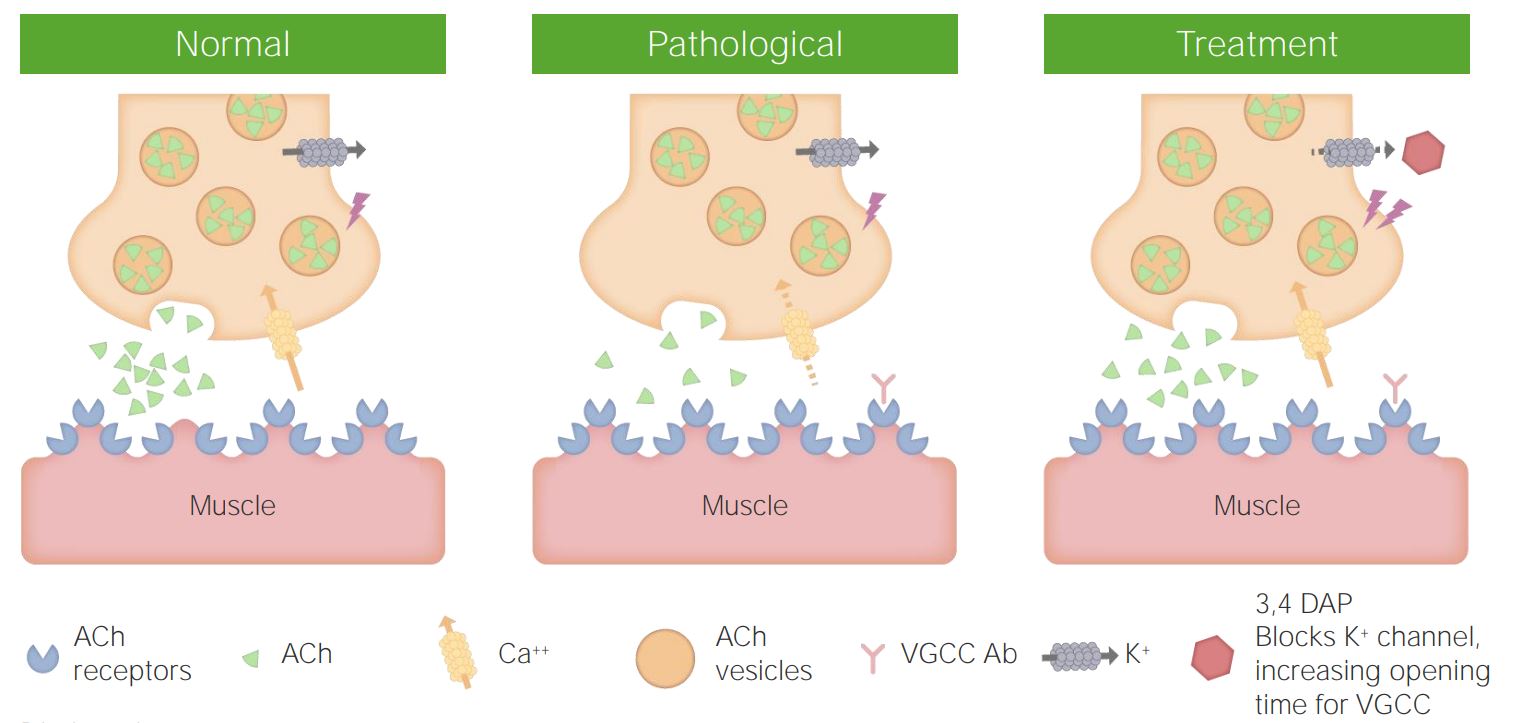
LEMS is an autoimmune disorder. Autoimmune disorders occur when the body's natural defenses against "foreign" or invasive organisms (for example, antibodies) begin to attack healthy tissue for unknown reasons. LEMS occurs because the antibodies damage the voltage-gated calcium channels (VGCCs) in the motor nerve membrane at the junction of the muscle nerve. These channels normally carry calcium to the nerves, releasing a chemical called acetylcholine. Acetylcholine helps connect nerve cells and muscles and is a group of chemicals known as neurotransmitters that help transmit nerve impulses. Antibodies attack the VGCC, resulting in decreased acetylcholine secretion [1,2] .
In patients with LEMS associated with cancer, an immune-mediated response is initiated because VGCC is present on the surface of cancer cells and the immune system stimulates the production of antibodies to fight cancer cells. Antibodies made against VGCC on small cell lung cancer are believed to mistakenly attack VGCC in nerve membranes instead. Smoking is one of the most important risk factors for SCLC, and in patients with LEMS associated with cancer, a long history of smoking is also an important factor [1,2] .
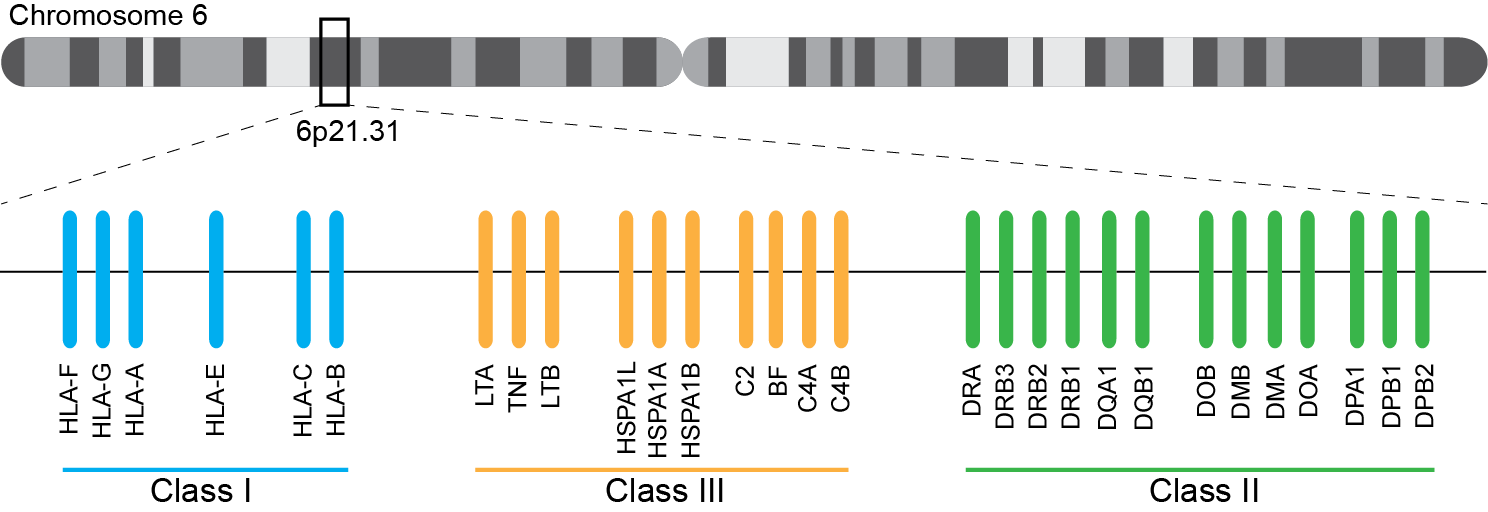
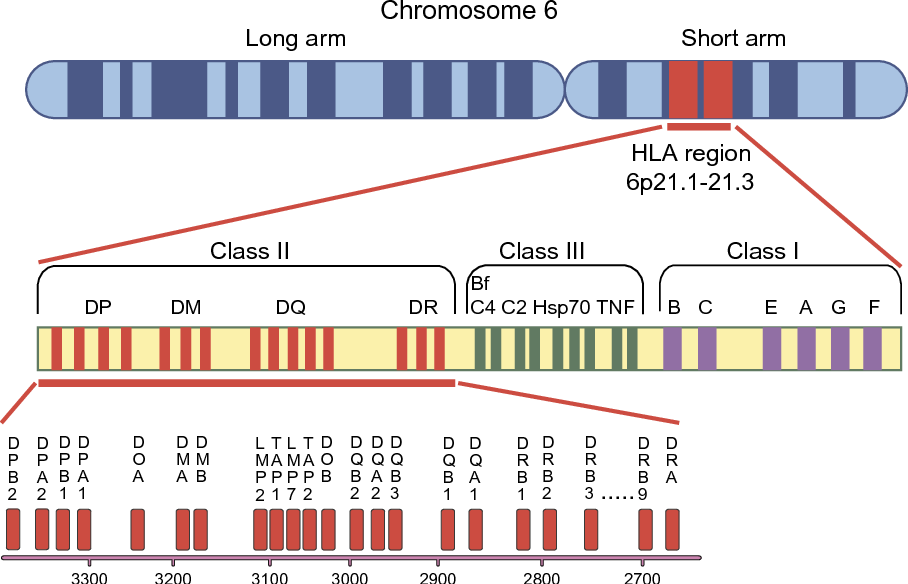
In people without LEMS without cancer, there is a genetic link to human leukocyte antigen (HLA) genotypes. HLAs are proteins that are also present on the cell surface and their function is to regulate the human immune system. However, it is still unknown what causes these proteins to break down and produce antibodie [1,3] .
Prevalence of Lambert-Eaton Myasthenic Syndrome (LEMS)
The estimated prevalence of LEMS worldwide is about 2.8 per 1 million people, making it a rare disease. There are approximately 400 known cases of LEMS in the United States. When LEMS is associated with SCLC, patients tend to get older and men are more likely to be affected by the syndrome than women. The average age of onset of SCLC is about 60 years. Approximately 3% of SCLC patients also develop LEMS, but the clinical signs of LEMS usually precede the diagnosis of SCLC (sometimes by years). When LEMS is not associated with cancer, the syndrome can occur at any age and typically begins around age 35. LEMS is very rare in the pediatric population and so far only 11 children have been reported in the medical literature. [1,3] .

In people without LEMS without cancer, there is a genetic link to human leukocyte antigen (HLA) genotypes. HLAs are proteins that are also present on the cell surface and their function is to regulate the human immune system. However, it is still unknown what causes these proteins to break down and produce antibodies. [1,4] .
The symptoms of the following disorders may be similar to those of Lambert-Eaton syndrome. A comparison may be useful for the differential diagnosis of this syndrome:
Myasthenic gravis (MG) is a chronic neuromuscular disease characterized by abnormally rapid weakness and fatigue of the sphincter muscles and resolves upon rest. Each muscle group may be affected, but the area around the eyes and the muscles used for swallowing are more involved. Often, because of the similarity in symptoms, LEMS is misdiagnosed as MG, but there are fundamental differences. In LEMS, eye muscle weakness, if present, is mild and, unlike MG, is almost never the only symptom. Severe respiratory muscle weakness, which can be fatal in MG, is rare in LEMS. There are no autonomic symptoms in MG that affect most LEMS patients. [1,5] .
Guillain-Barré syndrome is an autoimmune disease that causes damage to the myelin and axons of the nerve when the body's immune system attacks the nerves. Nerve signals are delayed and altered, causing weakness and paralysis of the muscles of the legs, arms, and other parts of the body. Abnormal feelings such as numbness or tingling may also occur. If the nerves are damaged, the patient experiences muscle pain and weakness, shortness of breath, and difficulty swallowing. If the autonomic nervous system is damaged, the patient may experience changes in blood pressure, heart rate, vision, body temperature, bladder function, and blood chemotherapy. [1,6] .
Diagnosis of Lambert-Eaton Myasthenic Syndrome (LEMS)
The diagnosis of LEMS is based on clinical signs and symptoms. Several diagnostic test methods are available to help diagnose LEMS. Electrophysiological studies are performed to measure muscle response and muscle strength. Repetitive nerve stimulation measures the electrical activity of a muscle during stimulation. Antibody testing is performed to detect the presence of anti-VGCC antibodies. [1,7].
Electromyographic results usually show a decrease in the combined motor performance potential (CMAP). Repetitive nerve stimulation initially shows a small amount of electrical activity in the muscle. After repetitive stimulation or high-repetition exercise, muscle activity increases. [1,8].
Anti-VGCC antibodies are detectable in approximately 85% of LEMS patients and are very specific to the disease if diagnosed. This is because anti-VGCC antibodies are found in LEMS with SCLC and in LEMS without cancer association. [1,9] .
Screening for SCLC is a very important part of the diagnostic process of LEMS. Chest CT (and sometimes FDG-PET) is usually the basis of this screening. Depending on the hazard profile, a negative initial screen is repeated at appropriate intervals. A recently discovered tumor marker antibody against the SOX gene, found in 65% of SCLC LEMS patients and absent in only 5% of non-tumor LEMS patients, may contribute to clinical treatment in the future. [1,10] .
Treatment Pathways in Lambert-Eaton Myasthenic Syndrome
Treatment for LEMS may vary depending on the presence of the accompanying cancer. If cancer is present, treatment first includes cancer-oriented therapies, which alone may help relieve the symptoms of LEMS. [1,11] .
There is no cure for LEMS, and treatment usually involves improving patients' quality of life. The FDA recently approved a new drug to relieve the symptoms associated with muscle weakness called Firdapse (amifampridine). It is a potassium channel blocker that works by increasing the secretion of acetylcholine. It is currently the only approved drug to improve the quality of life of LEMS patients. This drug has been shown to have significant benefits such as improving muscle strength and CMAP. In addition, it is a tolerable drug. [1,12] .
If Firdapse alone does not improve symptoms, there are other options that can be added if symptoms improve. Mestinon has been shown to treat MG, but is often used in combination with Firdapse to treat the symptoms of autonomic dysfunction (dry mouth, dry eyes, constipation, impotence, and decreased sweating). In MG, Menstinon improves muscle strength, but in LEMS, it only improves the symptoms of autonomic dysfunction. [1,13] .
In 2019, amifampridine was approved for the treatment of LEMS in patients 6 to 17 years of age. This is the first FDA treatment specifically approved for children with LEMS. [1,13] .
Immunosuppressive drugs (immunosuppressive drugs) are used in LEMS patients with more severe symptoms, such as prednisone (alone or in combination with azathioprine or cyclosporine). In some patients, a high-dose course of immunoglobulin may prevent further progression of the disease. Genetic counseling is also essential for all parents who want a healthy baby. [1,13] .
Discussion and Conclusion
LEMS syndrome is an autoimmune disorder of the neuromuscular junction. This is a false connection between the nerve cell and the muscle that leads to the gradual onset of muscle weakness. Symptoms of this syndrome begin in the proximal muscles of the legs or arms. LEMS is characterized by weakness and fatigue, especially in the muscles of the legs and arms. It can affect a patient's ability to do strenuous exercise and can make activities such as climbing stairs or walking on a steep path difficult. It starts gradually and usually lasts for a few weeks to a few months. There are often symptoms that progressively affect the shoulder muscles, leg and arm muscles, speech and swallowing muscles, and eye muscles. In patients with LEMS associated with cancer, an immune-mediated response is initiated because VGCC is present on the surface of cancer cells and the immune system stimulates the production of antibodies to fight cancer cells. Screening for SCLC is a very important part of the diagnostic process of LEMS. Chest CT (and sometimes FDG-PET) is usually the basis of this screening. Depending on the hazard profile, a negative initial screen is repeated at appropriate intervals. There is no cure for LEMS, and treatment usually involves improving patients' quality of life. The FDA recently approved a new drug to relieve the symptoms associated with muscle weakness called Firdapse (amifampridine). It is a potassium channel blocker that works by increasing the secretion of acetylcholine. [1,13] .
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
