
Research Article | DOI: https://doi.org/10.31579/2641-0419/535
1 Emergency department, Yaounde Emergency Center, Yaounde, Cameroon.
2 Department of Internal Medicine, Wayne State University School of Medicine, Detroit, Michigan, United States of America.
3 Liberty University School of Medicine Virginia, United State of America.
4 Department of Internal Medicine, Division of Cardiology, Tulane University School of Medicine, New Orleans, Louisiana, United States of America.
5 Department of Internal Medicine and Cardiology, Garden City Hospital, Michigan, USA.
*Corresponding Author: Aubin Sandio, Department of Internal Medicine, Wayne State University School of Medicine, Detroit, Michigan, United States of America.
Citation: Fleury Bolla, Aubin Sandio, Lady D Ayong, Ludovic Tchounja, Nana Dangpa, et al, (2025), The Role of Elevated Blood Pressure, Consciousness Level, and Hemiparesis in Stroke Outcome: a Retrospective Cohort Study, J Clinical Cardiology and Cardiovascular Interventions, 9(1); DOI:10.31579/2641-0419/535
Copyright: © 2026, Aubin Sandio. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 November 2025 | Accepted: 30 December 2025 | Published: 08 January 2026
Keywords: stroke; elevated blood pressure; impaired consciousness; hemiparesis; lmics, africa
Background: According to the World Stroke Organization (WSO) and the previous studies conducted by the Global Burden of Disease Analysis in 2021, it is estimated that there were 11.9 million incident strokes out of 93.8 million prevalent strokes. Hypertension was the main risk factor for stroke, contributing to around 90% cases [1]. To this risk factor, which subsequently requires adequate management, are added other clinical parameters such as the level of consciousness and the pyramidal deficit (Hemiparesis/hemiplegia), which also have a considerable impact on the prognosis of patients suffering from stroke. The situation gets worse when the focus shifts to sub-Saharan Africa. Following the example of Cameroon, where stroke outcome is characterized by high case fatality rates, with mortality rates around 25-30% within one month and over 30% within three months after a stroke event, and a particularly high recurrence rate.
Methodology: We carried out a retrospective descriptive study over a period of one year going from the 01st of January 2024 to 31st December 2024 at the YEC. We used the emergency department registers and looked for all files of patients admitted at the YEC and treated for Stroke-like conditions. We excluded any incomplete patient files and all cases with clear alternative diagnoses that explained the neurological deficits. The extracted data were entered and managed using a generated Google sheet. The demographic characteristics of our population, the risk factors, the symptoms and signs, the clinical presentation, the imaging used, the different types of strokes found, the different vascular regions affected, the different treatment and the outcomes of patients were extracted into an excel file. From these, we focused our attention on elevated blood pressure, hemiparesis/hemiplegia and impaired consciousness as presentation. Then using R Studio we analyzed the relationship between these presentations and the patient outcome.
Results: Impaired consciousness at presentation is the most powerful predictor of poor outcome in this cohort, with nearly half of affected patients dying during hospitalization. Hemiparesis is significantly associated with poorer recovery, reflecting more severe neurological injury. Elevated blood pressure at presentation is also significantly associated with outcome, suggesting a marker of systemic severity and possibly larger or more severe strokes. Overall, these results emphasize that neurological deficits and systemic severity markers at presentation are critical predictors of stroke outcome.
Discussion: Patients with elevated blood pressure were more likely to fall into less favorable outcome categories, suggesting that elevated blood pressure could be an indicator of more severe neurological injury or systemic stress. The presence of hemiparesis/hemiplegia corresponded to a higher proportion of patients who either passed away or achieved only partial recovery. Clinically, motor impairment reflects early cortical or subcortical damage involving the corticospinal tracts and is closely correlated with infarct volume and location. Patients presenting with reduced consciousness had disproportionately high rates of mortality and poor recovery. A GCS score ≤8 was significantly associated with increased mortality and functional dependence.
Conclusion: In acute stroke, elevated blood pressure, hemiparesis/hemiplegia, and impaired consciousness at presentation each have a statistically significant and moderate to strong association with patient outcomes. Impaired consciousness emerges as the most powerful predictor in this dataset. These findings support their continued use as rapid, bedside prognostic indicators and highlight the value of integrating simple clinical observations with formal outcome prediction models.
With a significant percentage of its burden now being focused on countries with strained economies, stroke continues to be one of the top conditions that claim lives and trigger chronic impairments. According to the World Stroke Organization (WSO) and the previous studies conducted by the Global Burden of Disease Analysis in 2021, it is estimated that there were 11.9 million incident strokes out of 93.8 million prevalent strokes.
Hypertension was the main risk factor for stroke, contributing to around 90?ses [1]. To this risk factor, which subsequently requires adequate management, are added other clinical parameters such as the level of consciousness and the pyramidal deficit (Hemiparesis/hemiplegia), which also have a considerable impact on the prognosis of patients suffering from stroke. As for stroke, most of the low and middle-income countries struggle to deal with its increasing incidence, but also with its management. The situation gets worse when the focus shifts to sub-Saharan Africa. Following the example of Cameroon, where stroke outcome is characterized by high case fatality rates, with mortality rates around 25-30% within one month and over 30% within three months after a stroke event, and a particularly high recurrence rate [2]. According to the World Health Organization (WHO), the global prognosis depends on geographical regions, access to healthcare, medical infrastructure; and especially in Low and middle-income countries, lower survival rates are due to the limited number of health care resources. These countries may have a 30-day survival rate close to 75%, while the one-year survival rate may be as low as 43% [3].
In order to further strengthen the understanding of the impact that the increase in blood pressure, the level of consciousness, and the presence of motor deficit (hemiparesis) can have on the outcome of stroke victims, a retrospective study has been conducted in a structure with limited resources: the Yaoundé emergency center (YEC), over a period of one year. It evaluated, on one hand, the impact of both on the presence of these clinical parameters and on the other hand, their relationship with the outcome in the short-term patients managed for stroke.
Study Design and Location: We carried out a retrospective descriptive study based on patient records over a one-year period. The research took place at the Yaoundé Emergency Center, located in Yaoundé, in the Centre Region of Cameroon. This medical facility comprises four departments: an Emergency Department (with 04 beds for non-trauma patients, 03 for trauma cases, and 01 bed for critically unstable patients), a Primary Care Unit (10 beds), an Intensive Care Unit (11 beds), and an Inpatient Ward (20 beds).
Study Population and Sampling Method: A total of 2,940 patient records, dated from January 1st to December 31st, 2024, were thoroughly reviewed to identify entries indicating possible stroke symptoms, diagnoses, or imaging results. From this pool, 318 records showed signs consistent with stroke-like conditions. These were selected for more detailed evaluation.
Inclusion and Exclusion Process: The 318 cases were assessed using established criteria to determine eligibility. After this screening, 189 cases met the requirements for inclusion.
Inclusion Criteria: Acute neurological symptoms such as weakness on one side of the body, facial drooping, speech difficulties, or sensory changes. Notes indicating a clinical diagnosis of stroke, cerebrovascular accident, or related terminology. Availability of adequate information in the file for meaningful analysis. All age groups were considered. Cases of transient ischemic attacks (TIAs) that resolved completely within 24 hours were also included.
Exclusion Criteria: Records lacking sufficient details. Cases where neurological symptoms could be attributed to other confirmed conditions such as trauma, post-seizure paralysis, brain tumors, or abscesses.
Final Sample Size: Following the inclusion and exclusion process, 189 patient records were selected for the final analysis.
Data Collection Process: A standardized Google Form was used to extract relevant data from the selected records. Information gathered included demographics (age and sex), known risk factors (e.g., high blood pressure, diabetes, smoking, atrial fibrillation), time of symptom onset and arrival at the facility, clinical signs and symptoms, available imaging results, documented diagnosis, treatments administered, and patient outcomes. From these, we focused our attention on elevated blood pressure, hemiparesis/hemiplegia and impaired consciousness as presentation. Then we analyzed the relationship between these presentations and the patient outcome.
Data Analysis: The data were entered and managed in a Google Sheet and analyzed using R Studio version 2025.5.1.513 on Windows 10/11. Descriptive statistics such as frequencies, percentages, means, and standard deviations were used to summarize the findings.
Ethical Considerations: This research adhered to ethical standards outlined in the Declaration of Helsinki. Approval was granted by the ethics committee of the University of Yaoundé I. Patient anonymity was ensured by removing all identifying information during data extraction and analysis.
Retrospective nature: The study depends on existing records, which may be incomplete or inaccurate.
Limited diagnostic tools: As the facility operates in a low-resource setting, access to advanced brain imaging was restricted, possibly affecting diagnostic accuracy.
Selection bias: Being a retrospective chart review, there is a risk of unintentional exclusion or misclassification of cases. No consistent follow-up: Lack of uniform follow-up data limited insights into long-term outcomes.
Study Importance: This study offers important observations about the relationship shared by elevated blood pressure, impaired consciousness and hemiparesis/monopoiesis and stroke outcome in a resource-limited environment. The results can help guide future efforts to improve stroke presentation.
Outcome distribution by clinical presentation
Table 1 shows the distribution of hospital outcomes by the presence or absence of hemiparesis, elevated blood pressure, and impaired consciousness at presentation. Outcomes are categorized as Discharged against medical advice (AMA), Fully recovered, partially recovered (including “Transferred for better care”), and passed away.
| Variable | Response | Fully recovered (n (%)) | Partially recovered (n (%)) | Passed away (n (%)) | Discharged AMA (n (%)) |
| Hemiparesis | No | 9 (15.3) | 30 (50.8) | 20 (33.9) | 0 (0.0) |
| Yes | 6 (4.6) | 87 (66.9) | 27 (20.8) | 10 (7.7) | |
| Elevated blood pressure | No | 10 (17.5) | 28 (49.1) | 14 (24.6) | 5 (8.8) |
| Yes | 5 (3.8) | 89 (67.4) | 33 (25.0) | 5 (3.8) | |
| Impaired consciousness | No | 13 (1.2) | 83 (71.6) | 14 (12.1) | 6 (5.2) |
| Yes | 2 (2.7) | 34 (46.6) | 33 (45.2) | 4 (5.5) |
Table 1: Outcome distribution and percentages by clinical variable
All three variables showed statistically significant associations with patient outcome (Table 2). Impaired consciousness had the strongest relationship (Cramér’s V = 0.39), followed by hemiparesis (0.28) and
hypertension (0.27). Fisher’s Exact Test was used for hemiparesis and impaired consciousness due to low expected counts in some categories; Chi-square was used for hypertension.
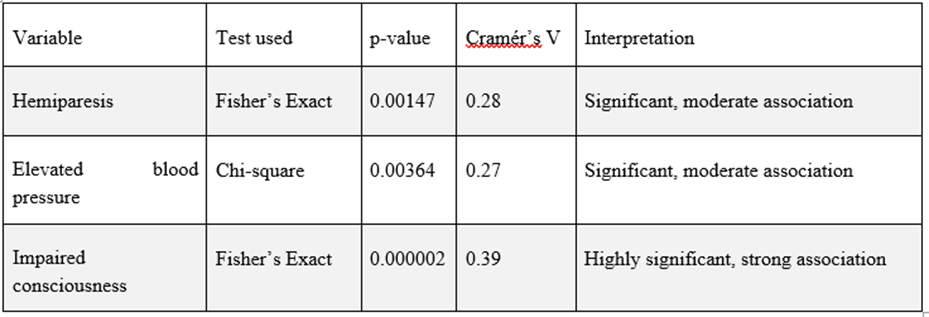
Table 2: Statistical association between Elevated blood pressure, Hemiparesis and impaired consciousness vs patient outcomes
Visual summary
Figures 1–3 present the outcome distribution for each clinical variable as stacked bar charts. Figure 1 (Hemiparesis): Presence of hemiparesis was associated with a higher proportion of partial recoveries and fewer full recoveries. Figure 2 (Elevated blood pressure): Elevated blood pressure
at presentation was associated with more partial recoveries and fewer full recoveries. Figure 3 (Impaired consciousness): Presence of impaired consciousness was strongly associated with increased mortality and reduced recovery rates.

Figure 1: Outcome distribution by hemiparesis (left) and its association plot (right)
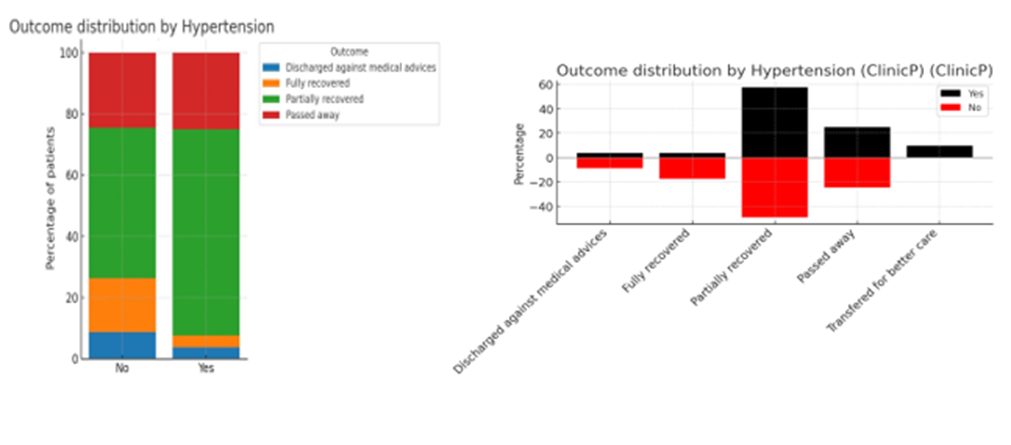
Figure 2: Outcome distribution by Elevated blood pressure (left) and its association plot (right)

Figure 3: Outcome distribution by impaired consciousness (left) and its association plot (right)
Key findings: Impaired consciousness at presentation is the most powerful predictor of poor outcome, with nearly half of affected patients dying during hospitalization. Hemiparesis is significantly associated with poorer recovery, reflecting more severe neurological injury. Elevated blood pressure at presentation is also significantly associated with outcome, suggesting a marker of systemic severity and possibly larger or more severe strokes. Overall, these results emphasize that neurological deficits and systemic severity markers at presentation are critical predictors of stroke outcome.

Figure 4: Proportion of patient with Elevated blood pressure, Impaired consciousness, and hemiparesis for each different outcome selected
This study investigated the association between selected clinical features at presentation—namely elevated blood pressure, hemiparesis hemiplegia, and impaired consciousness and patient outcomes following acute stroke. Outcomes were categorized into passed away, partially recovered (including transferred for better care), fully recovered, and discharged against medical advice. Statistical analysis used Pearson’s Chi-squared test for large-sample contingency tables and Fisher’s Exact test when cell counts were low, with Cramér’s V to estimate effect sizes and strength of association.
Elevated blood pressure
Elevated BP plays a dual role in stroke pathophysiology as a major etiologic factor and as a dynamic hemodynamic parameter influencing prognosis. In this study, uncontrolled elevated BP at admission demonstrated a statistically significant and moderate association with patient outcomes (Pearson’s Chi-squared test, p = 0.0037; Cramér’s V = 0.27). Patients with elevated blood pressure were more likely to fall into less favorable outcome categories, suggesting that elevated blood pressure could be an indicator of more severe neurological injury or systemic stress. Moreover, excessive elevation in systolic BP (>180 mmHg) is associated with increased risks of hematoma expansion, cerebral edema, and early neurological deterioration, particularly in intracerebral hemorrhage (ICH) [1,2]. The prognostic relevance of BP variability during hospitalization was also emphasized by Zhou et al. [3], who showed that fluctuations in mean arterial pressure (MAP) are linked to increased risk of infarct progression and poor neurological recovery. These findings align with the AHA/ASA guidelines that recommend careful BP management in acute stroke, balancing perfusion preservation with hemorrhagic risk [4].
Hemiparesis/Hemiplegia
Motor deficits, particularly hemiparesis/hemiplegia, was also significantly associated with outcomes (Fisher’s Exact test, p = 0.0015; Cramér’s V = 0.28), indicating a moderate strength of relationship. The presence of hemiparesis/hemiplegia corresponded to a higher proportion of patients who either passed away or achieved only partial recovery. Clinically, motor impairment reflects early cortical or subcortical damage involving the corticospinal tracts and is closely correlated with infarct volume and location [5,6]. Such deficits often imply prolonged rehabilitation needs and reduced chances of full recovery. Studies by Wahab et al. [6] and Brahimi et al. [2] support the prognostic utility of initial motor severity scores in predicting functional dependency, prolonged hospitalization, and long-term disability. In the acute setting, severe hemiplegia is often a proxy for large-vessel occlusion or extensive middle cerebral artery infarction, both of which are associated with poor prognosis in the absence of early reperfusion therapies.
Impaired Consciousness
Among the three variables studied, impaired consciousness, measured using the Glasgow Coma Scale (GCS), exhibited the strongest association with outcome (Fisher’s Exact test, p = 1.88 × 10⁻⁶; Cramér’s V = 0.39). Patients presenting with reduced consciousness had disproportionately high rates of mortality and poor recovery. A GCS score ≤8 was significantly associated with increased mortality and functional dependence, consistent with prior findings in African and global cohorts
Clinical Implications
The findings reinforce that these three clinical signs—hypertension, hemiparesis/hemiplegia, and impaired consciousness—are not only readily identifiable at the bedside but also strongly associated with patient trajectories. Their presence should prompt clinicians to anticipate increased care needs, closely monitor for deterioration, and engage early in multidisciplinary planning, including consideration for higher-level neurocritical care when resources permit.
Limitations
While the statistical associations are compelling, this analysis is observational and cannot establish causality. Blood pressure elevation, motor deficit severity, and impaired consciousness may be markers rather than direct drivers of poor outcome. Additionally, the study does not account for treatment variables, timing of intervention, or pre-stroke comorbidities, all of which could influence both presentation and outcome.
Taken together, these three parameters GCS, admission BP, and motor status form a pragmatic clinical trial that can guide early decision-making in settings with limited access to neuroimaging or laboratory markers. This triad aligns with recent calls from the World Stroke Organization and the AHA to promote simplified clinical tools for rapid triage and tailored care in LMICs [9,16].
Nonetheless, our study presents certain limitations. Its monocentric design and the lack of post-discharge follow-up limit generalizability. We were unable to account for potential confounders such as pre-stroke functional status, time-to-presentation, thrombolytic use, or post-acute rehabilitation. Additionally, although in-hospital endpoints provide valuable insight, they do not fully capture long-term stroke burden, especially in low-income populations with limited access to secondary prevention.
Despite these limitations, our findings are consistent with prior studies from Sub-Saharan Africa, North Africa, and Southeast Asia, reinforcing the need to systematically incorporate these bedside clinical markers into routine stroke management protocols. Early identification of high-risk patients could facilitate timely referral, resource allocation, and integration of neurocritical care principles even in under-resourced hospitals.
In acute stroke, Elevated blood pressure, hemiparesis/hemiplegia, and impaired consciousness at presentation each have a statistically significant and moderate to strong association with patient outcomes. Impaired consciousness emerges as the most powerful predictor in this dataset. These findings support their continued use as rapid, bedside prognostic indicators and highlight the value of integrating simple clinical observations with formal outcome prediction models.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
