
Research Article | DOI: https://doi.org/10.31579/2690-4861/455
1Army Medical Academy named after S.M. Kirov, St. Petersburg, Russia.
2North-Western State Medical University named after II Mechnikov, St. Petersburg, Russia.
3Municipal Multi-Profile Hospital № 2, St. Petersburg, Russia.
4The N.N. Petrov Research Institute of Oncology, St. Petersburg, Russia.
*Corresponding Author: Alexander V. Pechersky, DSc, Associate Professor, Shuvalovsky Pr., Apt. 51, St. Petersburg, Russia, E-mail: a_pechersky@mail.ru
Citation: Alexander V. Pechersky, Vadim S. Chirsky, Alexander A. Lisitsin, Vladimir N. Vilyaninov, Dmitry G. Korenkov, et al, (2024), The Role of Decreased Expression of Glucocorticoid Receptors in the Development of Itsenko-Cushing Syndrome, International Journal of Clinical Case Reports and Reviews, 17(3); DOI:10.31579/2690-4861/455
Copyright: © 2024, Alexander V. Pechersky. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 April 2024 | Accepted: 29 April 2024 | Published: 10 May 2024
Keywords: itsenko-cushing syndrome; glucocorticoid receptors; ACTH; cortisol; hyperplasia, adenoma and cancer of the adrenal glands
Background: Itsenko-Cushing syndrome is caused by unregulated excessive cortisol incretion by the adrenal cortex. The causes of increased stimulation of cortisol incretion by the adrenal cortex, leading to hyperplasia and tumors (adenoma and cancer) of the adrenal cortex, as well as to adenoma of the pituitary gland itself, remain unclear to date.
Materials and Methods: 6 patients with adrenal Itsenko-Cushing syndrome with adrenal cortex adenoma were under observation. The age of the patients ranged from 24 to 87 years. The patients underwent removal of the adrenal gland on the affected side. The control group consisted of 6 individuals who underwent surgical treatment of varicocele and hernias of various localization. In patients of the main group and control group, with their consent, a small fragment of skin from the edge of the surgical wound was taken for examination, which were fixed in a 10% formalin solution.
Results: The presence of adrenal Itsenko-Cushing syndrome in patients of the main group was confirmed by laboratory and instrumental studies, as well as characteristic clinical manifestations. The average Histochemical score of the expression of glucocorticoid receptors (GR) of the skin in patients of the main group with Itsenko-Cushing adrenal syndrome was 2.7 times less than the same value in the control group.
Conclusions: A decrease in the formation or absence of glucocorticoid receptors (congenital or acquired) blocks the negative feedback of cortisol suppression of corticoliberin production by the hypothalamus and ACTH-pituitary gland. The resulting excessive incretion of corticoliberin becomes the main link in pathogenesis of pituitary adenoma formation, and an excessive incretion of ACTH leads to the formation of cortical hyperplasia and tumors (adenomas, cancers) of the adrenal cortex. Unregulated excessive cortisol production by hyperplastic adrenal tissues or benign/malignant adrenal tumors leads to overcoming resistance to glucocorticoids and, according to the principle of negative feedback, suppresses the production of corticoliberin by the hypothalamus and ACTH-pituitary gland. As a result, the pituitary form of Itsenko-Cushing syndrome turns into an adrenal form with an unregulated increase in cortisol levels and a decrease in ACTH levels. Transfusion of the mononuclear fraction of peripheral blood obtained from healthy donors, which allows the pluripotent stem cells contained in it to partially replace the altered cells of all tissues of patients, is a promising method of treating patients with Itsenko-Cushing syndrome due to a hereditary decrease in the expression of glucocorticoid receptors.
ACTH, adrenocorticotropic hormone;
GR, glucocorticoid receptors;
KT, computed tomography
Itsenko-Cushing syndrome is caused by unregulated excessive cortisol incretion by the adrenal cortex [1]. Causes of increased stimulation of pituitary ACTH by hypothalamic corticoliberin (leading to pituitary adenoma and secondary increase in cortisol incretion in pituitary Itsenko-Cushing syndrome [1]), as well as increased cortisol incretion by the adrenal cortex (leading to hyperplasia and tumors - adenoma/cancers of the adrenal cortex in adrenal Itsenko-Cushing syndrome [1]) remain unclear. Accordingly, to date, no methodology has been developed for the prevention and etiopathogenetic treatment of Itsenko-Cushing syndrome.
The aim of the study is to confirm the hypothesis that the main cause of the development of Itsenko-Cushing syndrome is a pathology of glucocorticoid receptors, leading to compensatory increased stimulation of cortisol incretion by the adrenal cortex (accompanied by hyperplasia and tumors - adenoma / cancer of the adrenal cortex).
Patients with adrenal Itsenko-Cushing syndrome who had adrenal cortex adenoma (n=6) were under observation. All patients had unregulated excessive cortisol incretion, confirmed by a short test with dexamethasone, and reduced adrenocorticotropic hormone (ACTH) incretion, as well as obesity, hypertension, impaired glucose tolerance, purple blush on the face, red-purple striae on the abdomen and thighs. The diagnosis of adrenal cortex adenoma was confirmed by ultrasound, computed tomography (KT) and histological examination of the surgical material [1]. The age of the patients ranged from 24 to 87 years. The patients underwent removal of the adrenal gland on the affected side. With the consent of the patients, a small fragment of skin was taken from the edge of the surgical wound, which was fixed in a 10% formalin solution.
The control group consisted of individuals who underwent surgical treatment of varicocele and hernias of various localization (n=6). In the control group, with their consent, a small fragment of skin was taken from the edge of the surgical wound, which were fixed in a 10% formalin solution.
The criteria for inclusion in the main group were: the presence of Itsenko-Cushing syndrome in patients, indications for surgical treatment of adrenal cortex adenoma [1], and satisfactory general condition. The exclusion criteria were contraindications to surgical treatment of adrenal cortex adenoma [1].
The criteria for inclusion in the control group were: correct physique, normal skin color, normal blood pressure, satisfactory general condition, age from 18 to 35 years, indications for surgical treatment of diseases not related to endocrine pathology. The exclusion criteria were: the presence of endocrine diseases [1], age over 35 years or under 18 years.
Determination of hormone content
The determination of the content of ACTH and cortisol in blood serum, as well as free cortisol in daily urine, was carried out by immunochemiluminescent analysis using SIEMENS equipment (IMMULITE 2000 systems) and diagnostic kits (IMMULITE 2000 ACTH, REF L2KAC2 and IMMULITE 2000 Cortisol, REF L2KCO2); venous blood was taken in the morning and evening, on an empty stomach, at a fixed time (at 09.00 and at 21.00). During a short test with dexamethasone, 1 mg of dexamethasone was administered orally to all patients of the main group at 23.00 the day before [1].
The sensitivity and coefficient of variation for cortisol were 5.5 nmol/l and 7%, respectively. The sensitivity and coefficient of variation for ACTH were 1 pmol/l and 8%, respectively.
Immunohistochemical studies
The determination of glucocorticoid receptors (GR) was carried out using rabbit polyclonal antibodies (Anti-Glucocorticoid Receptor antibody ARG40891 arigobio.com) in a dilution of 1:1000. Antigen unmasking is high-temperature using EnVision FLEX Target Retrieval Solution High pH. Detection system: EnVision FLEX+ agilent.com. The results of the identification of GR were evaluated using the semi-quantitative Histochemical score method [2].
All data in the text and tables are presented in the form of averages and standard deviations (M±σ). The expression data of GR of the experimental and control groups were analyzed by comparing the two groups using the Student' s criterion (t) [3].
The serum cortisol content in the patients of the main group was increased in the morning and did not decrease in the evening. During a short test with dexamethasone, there was no suppression of cortisol incretion, and the content of free cortisol in daily urine exceeded 250 micrograms (Table 1). The content of adrenocorticotropic hormone (ACTH) in the blood serum was reduced (Table 2). The data of laboratory and instrumental studies, supplemented by characteristic clinical manifestations, indicated the presence of adrenal Itsenko-Cushing syndrome in patients [1].
| Cortisol | ||||
9-hours, blood serum, nmol/l
| 21-hours, blood serum, nmol/l | 9-hours, dexamethasone sample, blood serum, nmol/l | Free cortisol of daily urine, mcg/day | |
µ ± σ, n=6 | 609.3 ± 162.9
| 671.5 ± 224.5
| 626.5 ± 108.8
| 488.3 ± 245.2
|
Table 1: Cortisol content in blood serum and daily urine in patients with adrenal Itsenko-Cushing syndrome
| ACTH, 9-hours, pmol/l | |
µ ± σ n=6 | < 5>
|
Table 2: ACTH content in blood serum in patients with adrenal Itsenko-Cushing syndrome
In patients of the main group with Itsenko-Cushing syndrome, the expression of glucocorticoid receptors of the skin was weak or absent, and in representatives of the control group it was pronounced (Figures 1, 2).
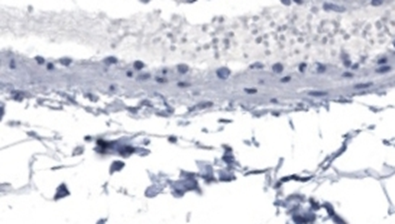
Figure 1: Absence of GR [removed]H-Score 0) of the skin in patient with Itsenko-Cushing syndrome (main group)
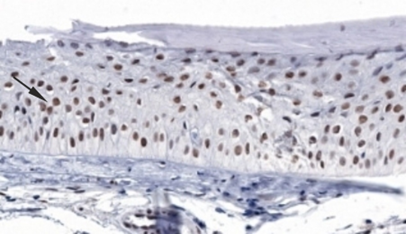
Figure 2: The expression of GR (H-Score 194,2) of the skin is normal (control group)
The average Histochemical score of the expression of glucocorticoid receptors (GR) of the skin in patients of the main group with Itsenko-Cushing syndrome was 2.7 times less (p<0> 56.9 ± 31.6 GR, Histochemical score µ ± σ, skin, patients of the main group with Itsenko-Cushing syndrome, n=6 µ ± σ, skin, individuals of the control group, n=6 154.5 ± 33.2 t 3.012 p p<0>
Table 3: Expression of GR of the skin in patients with Itsenko-Cushing syndrome and in the control group
The receptors that receive the signal and the increted hormones are a single interdependent system [4]. Cortisol deficiency may be due to pathological changes not only in the enzymes synthesizing it and its precursors [1], but also in the glucocorticoid receptors with which they bind. Due to congenital or acquired causes (in autoimmune or viral damage, for example, Epstein-Barr virus [1]), there may be a decrease in the amount of glucocorticoid receptors up to the absence, and there may also be a decrease in the affinity of binding of glucocorticoid receptors to cortisol.
With an insufficient number or absence of glucocorticoid receptors (manifested by a decrease or absence of their expression) (Table 3), the negative feedback mechanism of cortisol suppression of corticoliberin incretion in the hypothalamus and ACTH in the pituitary gland is weakened or blocked. Increased stimulation of ACTH leads to excessive cortisol incretion and to the development of pituitary Itsenko-Cushing syndrome. Weakening or blocking the action of cortisol initiates excessive incretion of corticoliberin by the hypothalamus and ACTH by the pituitary gland, as the main link in the pathogenesis of the formation of pituitary adenomas, hyperplasia [1] and tumors (adenomas, cancers) of the adrenal cortex. In particular, this caused the development of adrenal adenomas in the observed patients of the main group forming an excessive amount of cortisol (Table 1). Confirmation of this conclusion is an even greater increase in the production of ACTH and cortisol in patients with Itsenko-Cushing syndrome when they are prescribed a glucocorticoid receptor blocker (mifepristone), whose binding affinity to glucocorticoid receptors is 18 times higher than that of endogenous cortisol [5, 6, 7].
In addition to the excessive incretion of corticoliberin, ACTH and cortisol in Itsenko-Cushing syndrome, secondary ectopic production of ACTH and cortisol by tumors and normal tissues occurs. The hormonal activity of non-endocrine tissues is due to their participation in compensatory and adaptive reactions that develop in response to the insufficiency of the action of the corresponding hormones or their receptors [8, 9]. Potentially, any cell of the body that has a nucleus (containing genetic information about all biological processes of the body) can have hormonal activity. Examples of such ectopic hormonal activity are the extrahonadal production of testosterone with partial age-related androgenic deficiency [8, 9], synthesis of pituitary hormone analogues by prostate cancer cells [10], extrahonadal production of estrogens by adipose and other tissues in women [11] during menopause, renin synthesis by myocytes of the wall of the bearing arteriole transformed into epithelioid cells, and mesangiocytes of the kidney with pronounced, prolonged ischemia of her tissues [12]. Non-endocrine cells and tissues, which manifest hormonal activity during the formation of compensatory and adaptive reactions, form a diffuse endocrine system (APUD system). Compensatory hormone incretion by non-endocrine cells and tissues (including tumor cells) [1, 4, 12] is unregulated and inadequate. Due to the fact that this compensatory adaptive reaction reaches its greatest severity with malignant transformation of the tissues involved for this purpose [8, 9], the ectopic production of ACTH and cortisol in Itsenko-Cushing syndrome increases the risk of malignant tumor transformation of non-endocrine tissues that incret these hormones.
Excessive unregulated cortisol production by hyperplastic adrenal glands, benign/malignant adrenal tumors, or other tissues leads to overcoming glucocorticoid resistance (similar to overcoming by high levels of insulin the insulin-resistance in type 2 diabetes) - to suppression of corticoliberin incretion by the hypothalamus and ACTH pituitary gland by a negative feedback mechanism. Overcoming receptor resistance is due to the ability of high hormone levels to bind to receptors of other hormones similar to them in structure [13], with their manifestation of their action. Thus, the initial pituitary form of the Itsenko-Cushing syndrome passes into the next stage - the adrenal form of this syndrome. Accordingly, patients with the adrenal form of Itsenko-Cushing syndrome [1] have normal or reduced levels of ACTH. In patients of the main group, the level of ACTH was lowered (Table 2).
The appointment of glucocorticoid receptor blockers and cortisol synthesis enzymes in Itsenko-Cushing syndrome allows you to control the negative effects of an excess of glucocorticoids, but does not restore hypothalamic-pituitary-adrenal regulation and does not prevent the progression of pituitary adenoma growth [14]. These drugs lead to the resumption (in the adrenal form) or to an increase (in the pituitary form) of excessive ACTH incretion [14], causing hyperplasia, adenoma and cancer of the adrenal cortex (due to decreased suppression of corticotropin and ACTH incretion by cortisol).
A promising method of treating Itsenko-Cushing syndrome caused by a hereditary decrease in the expression of glucocorticoid receptors is transfusion of the mononuclear fraction of peripheral blood (harvested from healthy donors of the same sex and blood groups with patients), which allows pluripotent stem cells containing it to partially replace the altered cells of all tissues of patients [15, 16, 17]. In case of autoimmune damage to glucocorticoid receptors, desensitization with the appointment of peptide preparations containing their tissue-specific antigens may be a promising treatment method [15, 16, 18]. Since the development of the Itsenko-Cushing syndrome begins with blocking the glucocorticoid receptors of the hypothalamus and pituitary gland, it is necessary to prescribe peptide preparations made from animal brain tissues (containing, among other things, tissue-specific antigens of the glucocorticoid receptors of the hypothalamus and pituitary gland). In case of viral damage to glucocorticoid receptors, the prescription of peptide drugs will contribute to the redistribution of migration of stem cells directed to the restoration of the corresponding affected tissues. These methods of treatment, aimed at eliminating the causes of the development of Itsenko-Cushing syndrome, are potentially capable not only of leading to the reverse development of the disease at the initial stage, but also to increase the effectiveness of surgical and / or radiation treatment of benign / malignant tumors of the pituitary gland and adrenal glands.
Insufficiency of the number of glucocorticoid receptors up to their complete absence, as well as other pathological changes in glucocorticoid receptors (congenital or acquired) are the main causes of the development of Itsenko-Cushing syndrome. The pituitary and adrenal forms of Itsenko-Cushing syndrome are stages of the same disease, and the developing ectopic form of Itsenko-Cushing syndrome is a consequence of attracting other tissues to additional ectopic formation of cortisol and, possibly, ACTH, corticoliberin. Depending on the causes of the development of the Itsenko-Cushing syndrome, promising methods of etiopathogenetic treatment of this disease may be: partial replacement with pluripotent stem cells (harvested from healthy donors of the same sex and blood groups with patients) the altered cells of all patient tissues (including tissues of the hypothalamus and pituitary gland), as well as desensitization or stimulation of tissue renewal (regeneration) with appropriate peptide preparations.
The authors declare that they have no conflicts of interest.
None
The author's team thanks Prof. Boris K. Komyakov, Dr. Anton L. Pavlov, Ms. Marina M. Urchakova and Mr. Alexander A. Plushev for their assistance in conducting scientific research.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
