
Review Article | DOI: https://doi.org/10.31579/2578-8868/280
1Neurology, Shandong Provincial Qianfoshan Hospital,Thousand Foshan street, jinan, 250000, shandong, China.
2Neurology, Yantai Yuhuangding Hospital,No.20, Yuhuangding East Road,Zhifu, District, yantai, 264000, shandong, China.
*Corresponding Author: Mengzhen Zhou, Neurology, Shandong Provincial Qianfoshan Hospital, Thousand Foshan street,jinan,250000, shandong, China.
Citation: Mengzhen Zhou, Rujia Liu, (2024), The Relationship between Sleep Disturbance and Early Alzheimer's Disease – Mild Cognitive Impairment, J. Neuroscience and Neurological Surgery, 15(1); DOI:10.31579/2578-8868/280
Copyright: © 2024, Mengzhen Zhou. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 06 November 2023 | Accepted: 27 December 2023 | Published: 08 January 2024
Keywords: sleep; mild cognitive impairment; alzheimer's disease; cognition; orexin dual receptor antagonist
During sleep, the brain can clear toxins related to Alzheimer's disease. Compared with the baseline without sleep disorder, subjects with sleep disorder have a 1.49-fold increased risk of Alzheimer's disease. There is a two-way relationship between sleep/wakefulness disorder and Alzheimer's disease pathology. Sleep plays an important role in memory consolidation. Research shows that sleep disorder may have an important impact on the symptoms and course of Alzheimer's disease. Therefore, we need to better understand the mechanism of cognitive and behavioral impairment related to Alzheimer's disease, and delay the progress of the disease by improving sleep. The risk of Alzheimer's disease in individuals with sleep disorder is higher than that in individuals without sleep disorder; Improving sleep can improve cognitive level and delay the development of cognitive impairment; DORA is an effective strategy to improve sleep disorder, neurodegeneration and cognitive impairment in patients with Alzheimer's disease.
Mild cognitive impairment (MCI) is a transitional state characterized by cognitive impairment between normal aging and early Alzheimer's disease (AD) [1]. The degree of cognitive impairment in MCI has not reached the level of dementia, but subjective and objective memory or functional impairment has existed[2, 3]. 10% ~ 15% of MCI patients can progress to dementia within < 1>The sleep disorders of AD patients mainly include insomnia, fragmented sleep, excessive somnolence, sleep breathing disorder, sleep wake rhythm disorder, etc. AD patients may have sleep disorders 10-15 years before dementia[8, 9]. It has become an important strategy to delay the progress of Alzheimer's disease by intervening risk factors[10]. This article reviews the role of sleep in the pathogenesis, treatment, management and future prospects of Alzheimer's disease. The current strategies for the treatment of sleep disorders in Alzheimer's disease were discussed with the aim of shifting from treatment to prevention.
2.1 Neuropathological mechanism of sleep disorder in AD
Research shows that in cerebrospinal fluid Aβ The change of concentration is closely related to sleep[11]. Pathological in the brain of people with short sleep time Aβ increased deposition, in cerebrospinal fluid Aβ The level increases during awakening and decreases during sleep, and the increase of slow wave sleep time can reduce A β gather. Current research confirms that Aβ in brain. The clearance routes of the blood brain barrier, lymphoid vascular system and intercellular fluid flow, etc., with the increase of age, accompanied by various diseases, sleep disorders and other factors, will affect the corresponding tissue structure degradation and dysfunction, leading to A β Deterioration of clearance capacity Animal experimental studies suggest that during sleep A β Is twice as clear as when awake, while after sleep deprivation, A β The deposition of the sediment increased obviously[12]. The gold standard of AD neuropathology is extracellular A β Senile plaques formed by deposition, intracellular nerve fiber tangles (NFTs) caused by p-tau. The abnormal double helix shape formed by p-tau and tubulin will aggregate to form NFTs and damage the microtubule structure of neurons. The study found that among people with normal cognitive function, there are A β Depositor ratio no A β The quality of sleep of the sedimenters was worse, and the number of awakenings after falling asleep increased; A β Deposition is associated with shorter sleep duration, more fragmented sleep, and lower sleep quality. The disorder of sleep structure will in turn cause A β The deposits further affect sleep. It can be seen that a vicious circle has been formed.
2.2 Alzheimer's Disease Brain A β Deposition, Tau protein phosphorylation
Sleep disorder will cause neuroinflammatory reaction, further increasing A β Protein deposition, and aggravate the pathological changes of senile dementia[13]. Sleep disorders can activate the body's inflammatory response, leading to the expression of inflammatory genes, the production of proinflammatory cytokines and further systemic inflammatory response[14, 15]. The change of sleep wake cycle may interfere with cognition, especially cause hippocampus related cognitive deficits. The sleep/wake cycle is controlled by the interaction between sleep promoting systems (including inhibition of GABA activity) and wake-up promoting systems (including orexin, acetylcholine and monoaminergic systems). New evidence suggests that sleep deprivation (SD) and circadian rhythm disruption (CRD) interact and increase the risk of Alzheimer's disease development[16]. Both may damage brain macromolecules (such as A β- Amyloid protein and microtubule associated protein tau's glymphatic vascular lymphatic clearance can increase local brain oxidative stress and reduce circulating melatonin levels[17, 18]. After a night of high-quality sleep, we will feel clear headed. Cortex, hypothalamus and cerebellum are involved in regulating cognitive and sleep wake processes. A series of changes occur in brain function during sleep deprivation, including changes in memory, attention and reward related brain regions. Sleep disorder increased by A β And tau protein levels increase the risk of dementia. Compared with individuals without sleep problems at baseline, those who reported sleep disorders had a significantly higher risk of developing all types of dementia.
2.3 Disorder of sleep wake cycle impairs cognition
Cognition and insomnia are mutually causal and have a two-way relationship. Some research results show that long-term chronic insomnia patients have impairment in memory, attention, executive ability, orientation and other cognitive areas. Sleep contributes to the recovery of nervous system function. The specific slow wave sleep defect of insomniacs is not conducive to the synthesis of proteins in the brain and the establishment of new synaptic connections, which in turn leads to changes in cortical cognitive potential, and ultimately causes cognitive function damage[19]. In addition, sleep disorder will lead to the decrease of blood flow in the prefrontal cortex, which is the main area regulating executive function, behavior and other cognitive activities. Sleep disorder damages cognitive function by affecting the prefrontal cortex[20]. Dendritic spines are the main part of synaptic transmission in the central nervous system, which are crucial to brain function and information processing and storage. Sleep disorders may affect brain expression in memory, cognition and emotion by changing the density and morphology of dendritic spines The study found that the rapid eye movement sleep (REM) of patients with MCI decreased compared with the control group, the synthesis of brain protein decreased, the recovery of energy and memory storage function decreased, thus affecting the learning and memory and working efficiency of the next day[21], and damaging cognition. The slow wave sleep (SWS) performance of the mild cognitive impairment group is also inferior to that of the normal subjects[22, 23]. The sleep quality and efficiency of MCI patients are also impaired to varying degrees. Low sleep efficiency often leads to headache, dizziness, tension, anxiety and other behaviors, which affect many cognitive areas.
2.4 Hippocampal atrophy in patients with Alzheimer's disease
The sleep structure of patients with Alzheimer's disease is disordered, and the volume of hippocampus shrinks. When the hippocampal atrophy reaches 10% - 20%, severe neurological headache and memory damage will be caused[24, 25]. The hippocampus of the brain is very fragile. With the increase of age, work and life pressure and other factors, the blood supply in the hippocampus will decrease, and the hippocampal neural stem cells will not get enough nutrition, and the hippocampus will gradually shrink[26]. Good sleep is the guarantee to keep the hippocampus equal in size and length. Good sleep can improve the formation process of AD cognitive impairment through the hippocampus.
The brain is known as the "human memory warehouse". The hippocampus in our brain is a small area less than 10 cm away from the end of our nose. The hippocampus is responsible for rapid learning and storage of instant information Sleep is a physiological activity necessary for the consolidation of learning and memory and the maintenance of normal brain function[27]. Sleep disorders affect synaptic plasticity by interfering with some neural pathways in the brain, especially GABA and cAMP circuits. The inhibition of hippocampal synaptic plasticity may be one of the mechanisms of cognitive impairment caused by insomnia. The bilateral hippocampus of insomniacs were significantly "smaller" than that of the control group. Other studies found that long-term sleep structure disorder reduced the excitability of neurons, resulting in reduced protein synthesis, which ultimately affected the length and transmission efficiency of synapses, the density and morphology of dendritic spines, leading to memory impairment.
2.5 Sleep affects learning and memory in hippocampus
The hippocampus plays an important role in learning and memory. The hippocampus of the brain controls the sleep center, memory center and emotional center. The hippocampus circuit of the brain is an important part of the attention distribution center or the attention distribution execution center. Long term poor sleep quality and high pressure will cause excessive secretion of adrenocortical hormone. When the secretion of adrenocortical hormone is excessive, the hippocampus will be damaged, and people's memory ability will become worse. Their attention will be lax, and the brain's ability to perceive, remember, think and other learning and cognition will decline.
The status quo of severe sleep insufficiency or poor sleep quality in AD patients, accompanied by memory decline and inattention[28].The volume of hippocampus and related parts in patients with sleep disorder decreased, which indicates that the hypothesis supporting the reduction and damage of hippocampal neurons leading to sleep disorder is valid. The root cause of hippocampal atrophy is that the decrease of blood supply to this part leads to the reduction and atrophy of neuron volume, which leads to sleep disorder, memory decline, inattention, neurasthenia, and depression when the atrophy reaches 15%~20%[29, 30]. By preventing the development of hippocampal atrophy, these diseases can be treated and improved.
3.1 Alzheimer's disease and orexin
The dysfunction of cholinergic neurotransmission in neurodegeneration of Alzheimer's disease will lead to the up regulation of orexin system[31]. It has been reported that patients with moderate to severe Alzheimer's disease have higher average orexin levels, and sleep impairment at night is more serious[32, 33]. It was proved that the level of orexin in CSF was high Orexin immunoreactive neurons in the hypothalamus of patients with Alzheimer's disease are reduced by 40%[34]. It further confirmed the relationship between orexin and Alzheimer's disease. The expression of orexin in CSF is positively correlated with cerebral ischemia, which accelerates the progression of Alzheimer's disease. As an important factor affecting sleep, orexin may participate in the formation of cognitive impairment in Alzheimer's disease. Patients with Alzheimer's disease often have daytime sleepiness with multiple naps and waking fragments, especially in the moderate to severe stages of the disease[35, 36]. It is suggested that the level of orexin in CSF is low, and the insufficient neurotransmission is related to the increased number and duration of daytime naps in patients with Alzheimer's disease. The orexinergic system exhibits an activation pattern during waking and rapid eye movement, because it promotes arousal physiologically by activating the arousal monoaminergic group and deactivating the cholinergic network during rapid eye movement[37]. Correct orexin signaling is considered to be the key to ensuring the circadian rhythm of the entire sleep wake cycle. Sleep stability plays an important role in the occurrence and development of Alzheimer's disease.
3.2 Use of hypnotics
The study found that most of the elderly with MCI would choose to use hypnotic drugs to quickly improve their sleep status when they were troubled by sleep disorders. Many hypnotics are addictive and drug resistant. For example, the most common benzodiazepines can prolong the duration of shallow sleep and shorten the latency of falling asleep, but they are not conducive to A β Clear, even appear rebound and withdrawal symptoms, and then increase cognitive impairment[38].
Orexin is an excitatory neuropeptide produced by hypothalamus. It plays a role in regulating sleep awakening by activating OX1R/OX2R[39]. The level of orexin-A in plasma of patients with chronic insomnia increases, and A in cerebrospinal fluid of patients with early Alzheimer's disease Aβ The levels of orexin-A and orexin-A increased at the same time, while the levels of orexin-A in cerebrospinal fluid of patients with advanced Alzheimer's disease decreased. Overactivation of the Orexin system can lead to excessive arousal of the brain, leading to insomnia.
Orexin dual receptor antagonist (DORA) is an insomnia drug developed by Merck. It was approved by the US FDA in 2014 and is mainly used for the treatment of insomnia characterized by difficulty in falling asleep and/or maintaining sleep[40, 41]. Clinical experiments show that DORA can prolong sleep time and stabilize normal sleep structure. Studies show that DORA does not damage cognitive function. In addition to its impact on subjective and objective sleep initiation and maintenance, DORA also improves patients' perception of sleep quality[42]. Subjectively, DORA improves their mood significantly, and they feel refreshed in the morning. Therefore, more research will be needed on whether it is possible to stabilize sleep, reduce sleep fragmentation, and then delay the pathological progress of Alzheimer's disease and the impairment of learning and memory function by interfering with the orexin system.
3.3 Application of orexin dual receptor antagonists in corresponding fields or clinical trials of drugs.
Orexin plays a central role in regulating wakefulness. Studies have shown that mice with the orexin gene knocked out are less likely to develop Alzheimer's disease. This may mean that orexin and sleep debt may be upstream drivers of Alzheimer's disease. In normal animals, the activity of orexin shows diurnal changes, increasing when awake and decreasing when sleeping[43]. The elucidation of the role of orexin in regulating arousal shows that orexin receptor antagonists can provide a new way to treat insomnia by blocking orexin mediated arousal. Experiments on rodents have shown that orexin receptor antagonists promote slow phase sleep (NREM) and rapid eye movement sleep (REM), do not interfere with the quantitative spectrum (EEG) of specific sleep stages, allow fuzzy sleepiness in normal sleep[44, 45], and do not damage the ability to selectively respond to and stimulate significant emotional auditory stimuli, similar to natural sleep. If the treatment shows that it is more effective to reduce insomnia at night without bringing residual sleepiness during the day, the patient will benefit.
DORA connects the ventrolateral preoptic area (to promote sleep) and the brain stem (to promote wakefulness) in maintaining a long and consolidated state of consciousness, and by activating the wake-up area during wakefulness to stabilize the behavioral state, it prevents the unnecessary transition between wakefulness and sleep when the orexin neurons in the body are released during wakefulness, and stops discharging the role of orexin receptor antagonists during sleep, which can theoretically induce sleep and reduce the nocturnal wakefulness of insomnia patients. Compared with the subjects taking placebo, those taking DORA fell asleep faster, woke up less at night and woke up faster the next day. In the follow-up survey, the patient was well tolerated without serious safety problems, rebound or drug withdrawal reaction[46, 47]. Combined with DORA's unique mechanism of action, low addiction and other advantages, DORA shows considerable application prospects.
3.4 Efficacy and safety of orexin dual receptor antagonist
The results of two three month randomized, double-blind, placebo- controlled studies, two key phase III studies published at the annual meeting of the United Professional Sleep Association, showed that the experimental insomnia drug DORA could effectively increase the sleep efficiency (SE) of patients with mild to moderate Alzheimer's disease dementia, and significantly shorten the persistent sleep latency (LPS). Total sleep time (TST) was significantly longer[48, 49]. It reduces the waking time after falling asleep (WASO), and can slightly increase the proportion of rapid eye movement sleep (REM) sleep in patients with insomnia[50].
The study found that DORA improved the onset and maintenance of sleep for more than 3 months at night[51, 52]. Compared with the placebo, DORA did not seem to significantly change the underlying sleep structure characteristics. In addition to its impact on subjective and objective sleep onset and maintenance, DORA also improved the patients' perception of sleep quality. Subjectively, DORA significantly improved their emotional improvement and felt refreshed in the morning. The clinical benefits of these DORA for night sleep improvement are reflected in the overall assessment of disease severity and improvement by patients and clinicians.
The most common (≥ 5%) adverse events with a higher incidence in the DORA high-dose group were somnolence and headache. The number sign replacement test (DSST) showed that DORA had no significant objective residual effect on the next day compared with placebo[53, 54]. The tolerance of DORA was good, and there was no rebound or drug withdrawal effect after drug withdrawal. When somnolence occurs, its severity is generally mild to moderate, and it rarely requires interruption of treatment. The risk of sleepiness and related AEs seems to be dose related.
Many other studies are ongoing on patients with mild cognitive impairment and mild Alzheimer's disease. In the preclinical phase, there is a consistent commitment to immunotherapy to remove amyloid or prevent the formation of pathological morphology Importantly, a series of studies have shown that the relationship between Alzheimer's disease and sleep disorders may be complex and bidirectional. In fact, extracellular neuronal protein amyloid (A β) The accumulation of β - lactamase leads to changes in sleep wake behavior in mice and humans. At the same time, the disorder of normal sleep wake cycle may also promote the onset of Alzheimer's disease. Orexin not only promotes wakefulness, but also contributes to a higher level of in the brain Aβ It is also relevant to Aβ Dynamics has a direct impact. A series of studies have shown that the relationship between Alzheimer's disease and sleep disorders may be complex and bidirectional. The impairment of sleep wake cycle is not only the result of the pathology of Alzheimer's disease, but also aggravates the pathology of Alzheimer's disease. The loss of neurons and the impairment of cognitive function are both related to Aβ accumulation correlation. Sleep disorder is another important factor that accelerates the onset of Alzheimer's disease. For example, amyloid plaques and tau protein tangles are also common in brain regions that are critical to the regulation and regulation of sleep wake cycles
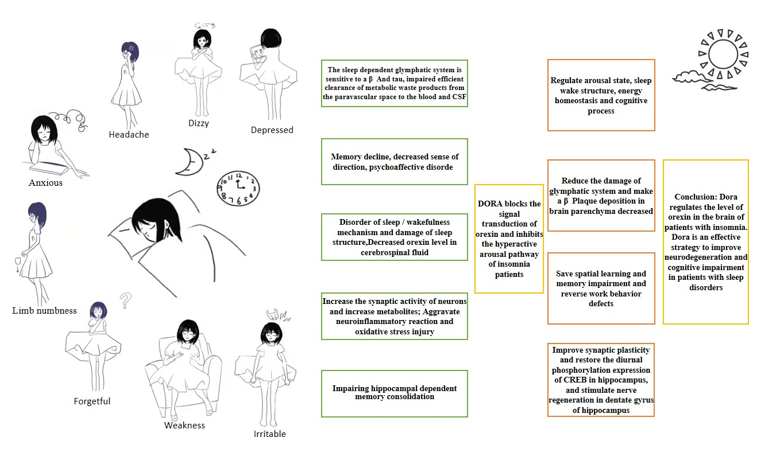
Figure 1: There is a twoway relationship betweensleep/wakefulness disorder and Alzheimer's diseasepathology. Sleep plays an importantrole in memory consolidation.
Significant changes in the quality and quantity of REM sleep have been evident in the stage of mild cognitive impairment of Alzheimer's disease, which is the first sign of sleep disorder in the pathology of Alzheimer's disease. For a long time, sleep disorder is very common in the process of Alzheimer's disease, which may be related to cholinergic consumption. In fact, it has been proposed that the impairment of cholinergic network in Alzheimer's disease neurodegeneration may be the cause of sleep interruption and NREM/REM sleep change[55]. Mild cognitive impairment is considered to be the precursor of dementia. Early and effective intervention of sleep quality can delay the development of dementia. At the early stage of the course of disease, when cognitive ability is not impaired, sleep impairment has become a predictive indicator of AD, which may be prevented from becoming AD or delayed to become AD, reducing the economic burden of society. For patients with newly emerging sleep disorders, screening cognitive scale, head MRI, polysomnography (PSG), and regular follow-up of changes in cognitive function and sleep may become the trend of AD prevention in the future[56]. We can assume that the use of orexin dual receptor antagonists as potential preventive, therapeutic or neuroprotective drugs, targeting the down-regulation of orexinergic system, is not only to manage sleep disorders in Alzheimer's disease, but also to improve sleep to slow down the neurodegenerative process of Alzheimer's disease and slow down its cognitive impairment.
Author Contribution
The first author ** obtains, analyzes or interprets the data of the work; The second author ** drafted works or made critical modifications to important knowledge content. ** has made significant contributions to the conception or design of the work, and finally approved the version to be published, and agreed to be responsible for all aspects of the work to ensure that problems related to the accuracy or completeness of any part of the work are properly investigated and resolved.
Article writing and subject research process, no conflict of interest, no ethical conflicts involved content
I and other authors declare that this article does not involve any ethical conflict
Data openly available in a public repository. The data that support the findings of this study are available in repository name e.g “figshare”at http://doiorg/[doi] reference number [reference number].
We thank all authors who contributed data to our analyses, and the foundations and committees that supported this study. And thanks for language assistance during the preparation of this manuscript. Two authors participated independently in the design, implementation, and evaluation of the article and had formal training.
Articles have been scrutinized with a professional anti plagiarism literature detection system prior to publication. Article statistical methods have been approved by Shandong First Medical University Graduate School Biology. Statistical expert review. This is an open access article which, under the terms of the Creative Commons license (4.0) (attribution 1 noncommercial share identical by descent), permits others to edit, adapt, and expand on the original article for non-commercial purposes, provided that the article is read, downloaded, copied, transmitted, printed, retrieved, hyperlinked by any user, and building for indexing, to be used as input data to the software or for any other legitimate use.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
