
Research | DOI: https://doi.org/10.31579/2578-8949/087
1 Department of Dermatology, Royal Wolverhampton NHS Trust, Wolverhampton, United Kingdom.
2 Department of Health Promotion and Public Health, University of West London, London, United Kingdom.
*Corresponding Author: Mohammed S Al Abadie PhD FRCP, Department of Dermatology, Royal Wolverhampton NHS Trust, Wolverhampton, United Kingdom.
Citation: Mohammed S Al Abadie, F Asharaff, Dina Al Abadie. (2021) The Psychosocial impact of Rosacea in men: First quantitative study. Dermatology and Dermatitis. 6(4); Doi:10.31579/2578-8949/087
Copyright: ©2021 Mohammed S Al Abadie, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 September 2021 | Accepted: 25 October 2021 | Published: 30 October 2021
Keywords: rosacea; facial rash; emotional impact
Psychosocial impact of Rosacea in men has generally been a topic that in understudied in literature. We conducted a cross-sectional paper-based survey was conducted with male patients who have experienced rosacea for at least five years at the dermatology outpatient department at New Cross Hospital in Wolverhampton, England to determine the psychosocial impact of Rosacea on Men Quality of life and self-esteem. 52 % of the male population were noted to be “often” mentally pre-occupied by rosacea and frustrated due to rosacea. 85 % of the male population “never” used cosmetic camouflage. Mean function score is noted to be 6.81. This indicates that men are less in favour of coping mechanisms. Results from this study highlight that despite the emotional impact rosacea has on the male population, they do not frequently use coping mechanisms. This emphasises the psychosocial impact of rosacea on male population and the need for dermatologists to address the emotional impact on men as part of management as well as to raise awareness around this topic.
Rosacea is a common, chronic, inflammatory skin condition mainly affecting the central facial region (central part of forehead, chin, forehead and cheeks) [1]. The main features are recurrent episodes of facial flushing, persistent erythema, telangiectasia, papules and pustules [2]. Previously, rosacea has been categorised into four distinct clinical subtypes – Erythematotelangiatic, inflammatory papulopustular, phymatous and ocular). However, it is now found that patients can display signs of overlaps or transformation between these subtypes [3]. ROSCO (ROSacea Consensus) international panel of experts recommends a transition from a subtype classification to a more individualised, patient-centric approach depending on the presenting clinical characteristics to be able to appropriately address the spectrum of phenotypes [4].
Clinical research suggest that rosacea is three times more common in female population compared to male population. A global systematic review of 32 population based and secondary care studies with 26,519,836 adults revealed that prevalence of women and men were 5.41 % and 3.9 % respectively [5]. Despite the prevalence of disease in female population, it is important not to overlook male population affected as there is limited research around the topic of male rosacea in literature.
Rosacea presents with gender- and age-specific preferences with regard to lesion qualities. For example, rhinophyma nearly exclusively presents in the male gender [6]. In a large scale National Rosacea Society survey of more than 2,000 patients ( male and female population), it was found that men were more than twice as likely to experience an enlarged nose in a condition known as rhinophyma ( phymatous rosacea) [7]. As a result of this cosmetic deformity, the affected population tend to experience negative emotions such as depression, anxiety and embarrassment. These cause severe emotional distress which in turn impacts their self-esteem in social situations [8].
As male patients with rosacea are commonly perceived as chronic alcoholics, there is a huge stigma around rosacea in men as it is believed that their lifestyle choices ( ie, alcohol) has contributed to this disease [9]. This common public mispercepetion affects their self-esteem cause a profound impact on the patients’ psychosocial well-being [10].
Raising awareness amongst male patient population as well as public population and educating the target population that rosacea is a treatable dermatological condition would help reduce the stigma around the disease. Studying and understanding the psychosocial domains of rosacea will help dermatologists and psychologists formulate a more comprehensive patient-tailored treatment plan when it comes to treating rosacea as well as the psychological effects of the condition. This study aims to highlight the psychosocial effects of rosacea, specifically in the male population.
Study Design
This cross-sectional paper-based survey was conducted with male patients who have experienced rosacea for at least five years at the dermatology outpatient department at New Cross Hospital in Wolverhampton, England from January to June 2019. This survey screened for psychosocial effect of rosacea on male adults and captured data on clinical features as well psychosocial effects of Rosacea in Women. Clinical experts have contributed to this RosaQoL which is 5-point, 21- item likert scale questionnaire that targets the various psychosocial domains as a result of Rosacea. Rosenberg Self Esteem Questionnaire has also been adapted for use in this research.
The potential for ethical issues for this questionnaire was taken into consideration. Patients were provided with an information leaflet before participation and the authors identified no such ethical concerns.
Study population
A total of 21 male patients voluntarily participated in this survey. We have classified the patients according to their age groups.
Study variables
Rosenberg 1965 Self Esteem Questionnaire. Responses were scaled on a 4-point balanced likert scale (Strongly Disagree, Disagree, Agree, Strongly Agree). It is a 10-item uni-dimensional scale that measures global self-worth by measuring both positive and negative thoughts and self-perception. All items are answered using a 4-point Likert scale format ranging from strongly agree to strongly disagree. We had to take into consideration that certain items on the Rosenberg questionnaire- 2, 5, 6, 8, 9 were reverse scored [11]. Scores were kept on a continuous scale and ranged from 0-40, 40 indicating the highest possible score.
Rosacea related quality of life was assessed using the Rosacea specific Quality of Life questionnaire. It is a 21 item likert scale that evaluated the impact of rosacea on the quality of life of patients across three main domains-Emotion, symptom and function. The score of each RosaQoL questionnaire was obtained by averaging the responses to the 21 items. The answers to the items were “never”, “rarely”, “sometimes”, “often” and “always”. Responses were recorded on the scale of 1 (never) to 5 (always).

Inclusion Criteria
Age range: Divided into three groups- 41-50,51-60, >61
Male patients who have had rosacea > 5 years
Exclusion Criteria
1) Patients who did not complete the entire questionnaire
2) Patients who have been diagnosed and treated for rosacea for <5>
Statistical Analyses
Descriptive statistics have been used to describe survey data with Microsoft Excel. For categorical variables, frequencies have been reported. The data was then collated and entered into a spreadsheet ready for analysis. RosaQOL and Rosenberg 1965 Self-Esteem questionnaire were scored based on the guidelines set by the instrument developers. Descriptive statistics were reported for scale scores in the sample population.
Sample Characteristics
A total of 21 male patients were involved in this study. The final sample obtained fulfilled the criteria of duration the patient has been experiencing rosacea for more than 5 years . These are patients who are under the care of dermatologists at the New Cross Hospital and obtaining medical treatment. Results of the pooled survey are described in the results section in this paper.
Socio-demographic Characteristics
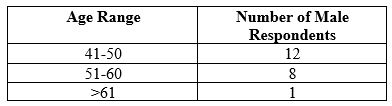
Out of the 21 male patients who responded to the questionnaire, 12 patients were between 41-50, making up the majority of the sample population. 8 of the sample fell into the category of 51-60 and one patient was more than 61.
Functional Domain (Coping mechanism)

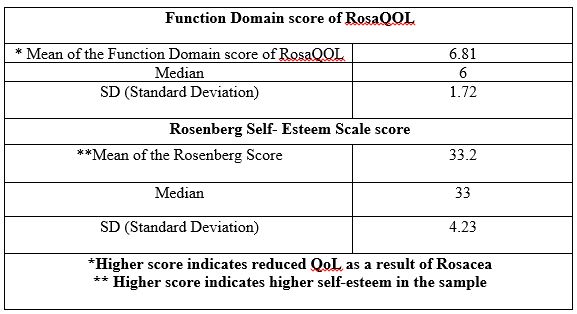
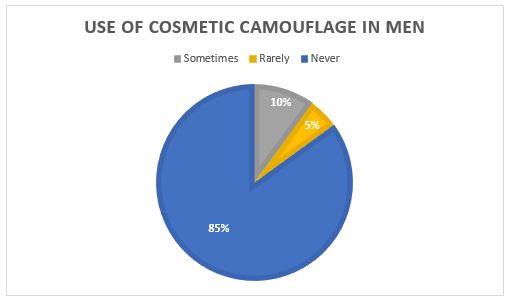
Function score is the cumulative score of the questions in the “function” domain which are coping mechanisms adapted by male rosacea patients, as illustrated by table 3. Standard deviation of 1.72 in the function domain indicates that the individual scores are close to the mean score (6.81). Maximum score in the function domain was noted to be 10, while the median score was noted to be 6. Higher score indicates increased use of coping mechanisms (make up, avoiding food or environmental triggers). It was noted that use of cosmetic camouflage was an unpopular option among est men. 85 % of the male population “never” used cosmetic camouflage, as illustrated by figure 1.
Rosenberg self-esteem scale was noted to have standard deviation of 4.23 which indicates a wider range of response from the male population.
Correlation coefficient (r) between these two variables (Rosenberg score and Function score) was noted to be -0.17, as calculated on Microsoft excel software. A negative linear relationship as shown in figure 2, indicates that the higher the self-esteem of patient (higher score of Rosenberg score), the lower the function score (less likely to adapt coping mechanisms such as make up and avoiding environmental triggers of rosacea).

Clinical characteristics of rosacea (Symptom Domain)
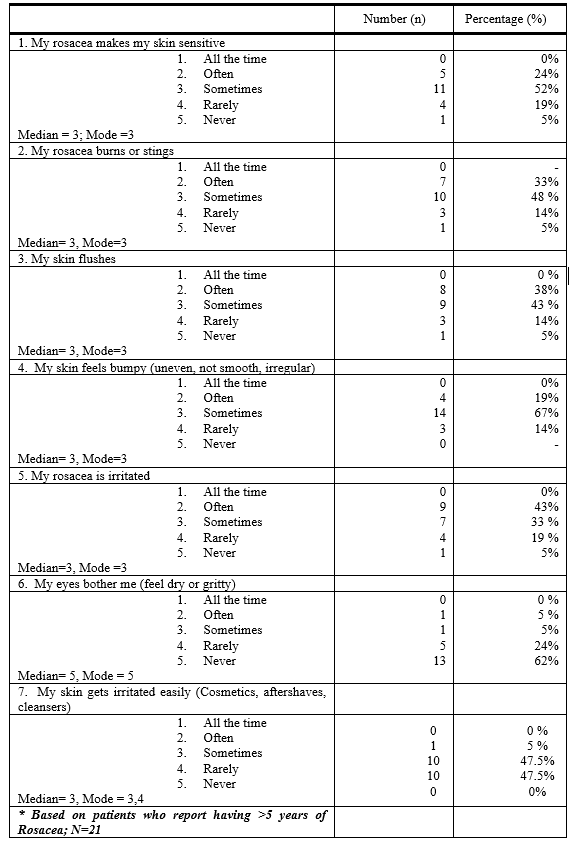
Clinical characteristics are described in Table 5. More than half of the sample population (52%) reported that they “sometimes” experienced sensitive skin due to rosacea. 48% of them reported they “sometimes” experience burning or stinging of the skin. 67% of the sample population felt that their skin was bumpy, irregular “sometimes” as a result of rosacea.
47.5% of the population “sometimes” or “rarely” experienced irritation of their skin after using various skin products (Cosmetics, aftershaves, cleansers).
However, ocular symptoms were least reported amongst all the clinical symptoms. 62 % of the sample population never experienced any ocular symptoms. Median and mode was noted to be 5. This indicates that majority of the population did not suffer from ocular type of rosacea.
Emotional Domain
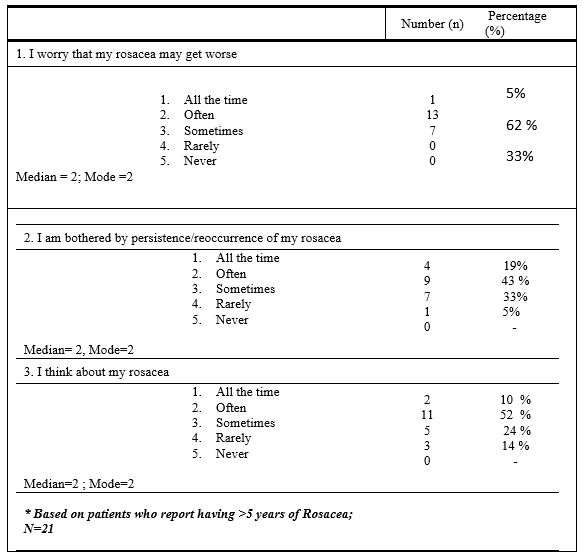
52 % of the male population were noted to be mentally pre-occupied by rosacea “often”. 24% of them “sometimes” thought about their condition. 43 % of the population was bothered by the persistence or recurrence of their rosacea “often”. None of the population were noted to be “never” affected by the persistence and thoughts of their rosacea.
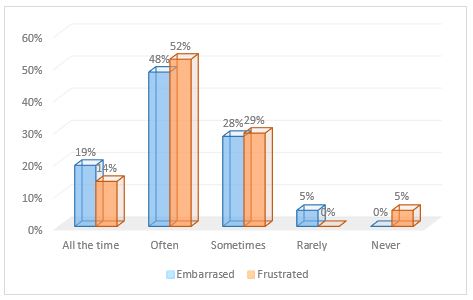
Figure 3 illustrates that 52 % of the sample population were “often” frustrated due to rosacea. 48 % of the population were “often” embarrassed by their condition. 19 % of the population were embarrassed “all the time” and 14 % of them were noted to be frustrated “all the time”. It is also important to note that none of the participants have “never” experienced embarrassment.
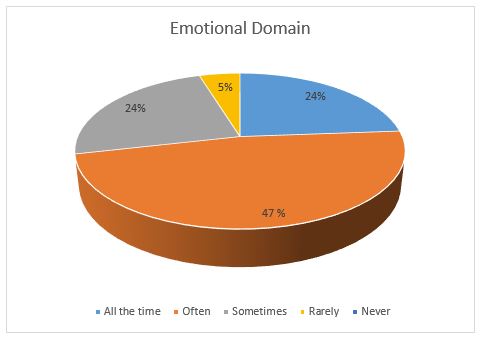
As illustrated by figure 4, 24 % of the male patients were annoyed by their rosacea “all the time”. A huge proportion of the population (47 %) were annoyed by it “often”. 24 % of them were feeling annoyed by their rosacea “sometimes”. 5% of the population rarely experienced this emotion. This indicates that a huge percentage of the male population were emotionally affected by their rosacea.
This study has been designed to explore the psychosocial impact rosacea has on male population. This will help patients as well as dermatologists to understand the psychological burden of rosacea. This study has explored the various psychosocial concerns (Function, emotional and clinical domains) experienced by male rosacea patients. This is the first cross-sectional survey based study on the psychosocial effect of rosea on men. It is a follow up from a study based in female population.
This specific study highlights the importance of acknowledging the psychosocial distress associated with rosacea. The Rosenberg self-esteem score as well as the function score noted in the male population indicates the need to address psychological factors such as embarrassment and frustration in the male population. A 1995-2002 analysis collected by the National Ambulatory Medical Care Survey and the outpatient component of the National Hospital Ambulatory Care Survey, which are both nationally representative surveys of healthcare visits in the U.S.A shows that 65.1% of patients with rosacea with a comorbid psychiatric diagnosis also experienced depression [12]. This is in line with the findings of current study in which a large proportion of male population were noted to be psychologically affected by rosacea due to embarrassment and frustration. It is important to note that our study highlights that men had stronger negative responses in the emotional domain as opposed to the clinical domain. Mode was noted to be three (sometimes) in the clinical section while the mode was noted to be two (Often) in the emotional domain. Thus, it is important for dermatologists to identify the emotional vulnerability in their patients and treat them according to their individual needs.
Coping strategies are very important in helping patients adapt to their clinical condition. In our current study, it is revealed that cosmetic camouflage is a very unpopular coping mechanism amongst men. A 2012 study which involved a search of the Medline and Scopus databases was performed to identify articles documenting the emotional benefit of cosmetic camouflage revealed that cosmetic camouflage provides a significant emotional benefit for patients with facial skin conditions [13]. However, it is noted from our study that male population do not use make up as a coping mechanism as much as female population. Further research will need to be done to explore this domain. One limitation of this study is that the data has been generated using quantitative questionnaire. Using a qualitative questionnaire will be useful in understanding male patient’s perspective. This will be helpful in understanding the reason behind the lack of adaptive coping mechanisms amongst male patients.
Given the small sample size, the reliability of the study may be affected as it may lead to biasness. Furthermore, a smaller sample size is less representative of the general population.
Results from this study sheds light on the need for further research in male population affected by rosacea. Given that there is a huge stigma surrounding male rosacea and the reluctance of male rosacea patients in using coping mechanisms , research around this topic will be very useful in further understanding this target population. It is important that awareness about rosacea in men is created to eliminate the stigma around it or to clear the misperceptions. Given that male population are psychologically vulnerable, it is important for dermatologists to collaborate with mental health professionals to treat the patients as well as to create public awareness. Social websites can be a very useful platform not just to raise awareness but to also help the men affected with rosacea.
This study is an initial step in identifying the psychosocial burden specifically in male population. Research focused in identifying the differences in male and female population is currently ongoing [14]. Future research should focus on the interventions (ie, social media) required to raise awareness around the topic of rosacea to eliminate stigma around this disease.
An informed consent was obtained from all the patients participating in the survey.
The authors declare that they have no conflict of interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
