
Opinion Article | DOI: https://doi.org/10.31579/2768-0487/057
Department of Internal Medicine B, Ziv Medical Center, Azrieli Faculty of Medicine, Safed, Bar-Ilan University, Israel.
*Corresponding Author: Raymond Farah, Department of Internal Medicine B, Ziv Medical Center, Azrieli Faculty of Medicine, Safed, Bar-Ilan University, Israel.
Citation: R Farah. (2022). The Potential Therapeutic Effect of Hypertonic Saline Solution (HSS) for the Management of Refractory Acute Decompensated Heart Failure (ADHF). Journal of Clinical and Laboratory Research. 5(2); DOI:10.31579/2768-0487/057
Copyright: © 2022 Raymond Farah. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 October 2021 | Accepted: 30 November 2021 | Published: 06 January 2022
Keywords: heart failure; hypertonic saline; diuretics; hyponatremia; renal failure
Patients with acute decompensated heart failure (ADHF) have high rates of mortality and morbidity despite recent improvements in diagnosis and treatment. Still patients with significant heart failure and especially with NYHA class III -IV HF and low blood pressure with or without hyponatremia and renal failure are considered severe patients with reduced response to standard treatment with high mortality rates and high re-hospitalizations as they are associated with worse prognosis. Several works and meta -analysis have shown the importance and benefit of treatment with the infusion of hypertonic saline solution (HSS) in these patients and in different conditions of cardiovascular collapse. Current evidence indicates that the infusion of hypertonic solution in heart failure patients can provide clinical and hemodynamic improvement. The investigators are testing the hypothesis that the infusion of hypertonic solution in association with diuretics may prevent the occurrence of renal dysfunction in patients with ADHF and can reduced the re-hospitalizations rate. Our experience in treating several patients has been successful and has shown significant improvement in symptoms and weight loss and improvement in renal function, due to the small size of the sample we were unable to perform a controlled study. We hypothesize that HSS, treatment should be adopted practically and a treatment protocol should be built in patients with intractable ADHF, especially with hypotension, hyponatremia with/without renal failure and overloaded.
Acute decompensated heart failure (ADHF), with an incidence of 1-2%, is a clinical syndrome with significant morbidity and mortality despite therapeutic advancements and ongoing clinical trials [1]. A recent therapeutic approach to patients with ADHF includes combination therapy with hypertonic saline solution (HSS) and furosemide, based on the hypothesis that resistance to loop diuretics occurs because of achievement of plateau in water and sodium excretion in patients receiving long-term loop diuretic therapy [2]. The proposed treatment is not known among most physicians and institutions, and is not performed routinely or standardly, in addition there is no uniform protocol that describes the methods of treatment. Some studies, case reports and meta- analyzes have researched the topic,most of them have proven the effectiveness of the treatment, to the best of our knowledge there are no large double blind randomized controlled studies. In previous years they were published some initial studies, that were followed by a series of small studies: in 2000, 2003, 2005, and culminated with 2011’s SMAC-HF study [3]. SMAC-HF was a single center randomized blinded-study (N=1927) comparing HSS with furosemide and a moderate sodium diet (120 mmol or 2760 mg) versus furosemide alone and a low sodium diet (80 mmol equivalent or 1840 mg). The HSS group had a shorter hospitalization (3.5 vs 5.5 days), improved NYHA class, lower readmission rate (~19% vs ~34%), and reduced CV mortality (~13% vs ~24%) [3]. The earliest work was an exploratory study from 1999 about treating heart failure with 150 ml of hypertonic saline (NaCl 1.4–4.6%) according to serum sodium values plus 250 mg IV furosemide twice a day [4]. They showed that this strange concoction was both safe and tolerated. The rationale behind this combination was to overcome diuretic resistance by using the HSS to draw water from the interstitial compartment, thus improving effective arterial blood volume and renal blood flow and counter the deleterious effects of furosemide by suppressing rather than activating the RAAS.
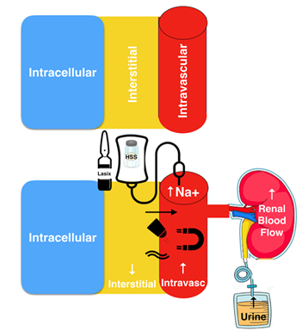
Recently the use of HSS was proposed as a treatment for refractory heart failure associated with high dose diuretic therapy, with promising results [5]. Most of the data were generally from patients with cardiogenic shock resulting from right ventricular infarction [6]. Another repot also evaluated the use of hypertonic saline as an adjunct therapy in an ADHF patients and indicated that HSS had positive effects on renal function [7]. Other experimental models HSS improved myocardial contractility [8]. The proposed mechanisms included volume expansion by hypertonic saline as a resuscitation fluid leading to the mobilization of fluid to the intravascular compartment followed by increased urine output (Figure 1). Additional effects include enhanced myocardial contractility, peripheral vasodilatation, improved neuro-hormonal profile, and increased renal blood flow. It is also hypothesized that the sodium chloride increase sensed by the macula densa may also play a role in increased diuresis. A meta-analysis was conducted to evaluate the efficiency of combination HSS plus furosemide therapy in patients with ADHF in terms of mortality, readmissions, length of hospital stay, kidney function, urine output, body weight, and B-type natriuretic peptide (BNP) [9]. 14 studies-four observational and ten randomized studies (total 3398 patients)-were included in the meta-analysis whose results demonstrate the superiority of combination HSS plus furosemide therapy over furosemide alone in terms of kidney function preservation (mean creatinine difference - 0.33 mg/dL; P < 0 xss=removed xss=removed> These surprising results from this unconventional treatment caught my attention. Maybe sodium was like beta-blockers in heart failure, a treatment that was contraindicated for years before someone give it a chance and now has become an evidence-based treatment widely recommended.
We hypothesize that HSS administration exerted a beneficial effect on the patient's myocardial contractility and improved his cardiac output and blood pressure, therefore HSS may be an alternative therapeutic option for the initial management of ADHF, despite the heterogeneity and possible risk of bias among the studies, results appear promising on multiple aspects. In summary, we need stronger evidence to better understand the effects of HSS therapy the optimal dose and duration of treatment. A future adequately powered, multi-centre, placebo controlled, randomized, double dummy, blinded trial also is needed to assess the benefit of hypertonic saline in patients with renal dysfunction, in diverse patient populations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
