
Research Article | DOI: https://doi.org/10.31579/2578-8868/282
National Brain Aneurysm & Tumor Center.
*Corresponding Author: ES Nussbaum, National Brain Aneurysm & Tumor Center.
Citation: LA Nussbaum, TM Janjua, ES Nussbaum (2023), The Potential Role of Peripheral Somatosensory Stimulation in the Treatment of Mental Health Symptoms following Traumatic Brain Injury, J. Neuroscience and Neurological Surgery, 14(2); DOI:10.31579/2578-8868/282
Copyright: © 2023, ES Nussbaum. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 14 November 2023 | Accepted: 01 December 2023 | Published: 08 December 2023
Keywords: anxiety ; depression ; neuromodulation ;PTSD ; somatosensory stimulation ; TBI ; trauma
Background
Patients with traumatic brain injury (TBI) may develop symptoms of post-traumatic stress disorder (PTSD), depression, and anxiety. Despite decades of research investigating treatment options, these mental health symptoms remain a major cause of quality-of-life impairment. In a series of patients with PTSD being treated with peripheral somatosensory stimulation (PSS), we further evaluated 3 patients who had suffered from TBI to detail their clinical response to therapy.
Methods
Three patients with TBI and PTSD underwent daily PSS therapy over a 4-week period. Patients were evaluated using a Veterans Affairs TBI scale of cognitive impairment and subjective mental health symptoms at baseline and then at the conclusion of the treatments. All data were obtained through a self-reported survey.
Results
Three men with TBI and PTSD completed one month of daily PSS therapy. No adverse events were described by the patients. All patients demonstrated improvement in terms of their scores assessing cognitive impairment and subjective symptoms. The Patients beginning with greater impairment appeared to derive more benefit from therapy.
Conclusions
PSS stimulation appeared to improve symptoms in three patients with TBI and PTSD. Symptoms related to both anxiety and depression were improved. We suggest that further investigation into the potential usefulness of PSS therapy in patients with TBI and mental health symptoms is warranted.
A significant percentage of patients with TBI will develop symptoms of PTSD, particularly following severe trauma [1-5]. These individuals may struggle with anxiety, depression, and even suicidal ideation in extreme cases. The mental health symptoms associated with PTSD in the setting of TBI result in a tremendous societal burden in terms of impaired quality of life, functional disability, medical costs, and unemployment [3-14]. It is estimated that more than 7 million Americans are diagnosed with PTSD every year. [2-5] In addition to pharmacotherapy and psychological interventions, treatment for PTSD has included various methods of relaxation including yoga and deep breathing exercises. [7-10,15] Peripheral somatosensory stimulation (PSS) therapy is a non-invasive technique which may be beneficial to patients with a variety of neurological disorders. [16-19] We recently evaluated the impact of PSS on symptoms in patients with PTSD. [20] Three of these patients had a history of TBI, and this report focuses on our experience with this small subset of TBI patients.
We treated 6 patients who had been diagnosed with and suffered from active PTSD symptoms with PSS using the NeuroGlove device. NeuroGlove is a non-invasive device that provides PSS stimulation in the form of pneumatic puffs of air directed at the volar surface of the distal forearm, the palm, and the fingers. Subjects used the device at home for 1 hour of therapy per day (30 minutes using each hand) for 4 weeks and were directed to synchronize their breathing to the firing (on/off cycle) of the machine to encourage relaxation during device use. The results of this trial have been previously reported. [20]
Of the six patients in the trial, 3 had a prior history of significant TBI. All felt that the TBI had at least in part contributed to their PTSD. We interviewed these patients to obtain detailed information regarding their response to treatment and analyzed the results obtained in this small subgroup of patients with TBI, focusing on their mental health symptoms of anxiety, depression, and general well-being to evaluate the potential usefulness of PSS in this subgroup of patients. We utilized the Veterans Affairs TBI Evaluation of Cognitive Impairment and Subjective Symptoms Scoring System [21]. This scale surveys patients in terms of their ability to function in 9 areas: memory and attention, judgement, social interaction, orientation, motor activity, visual spatial orientation, subjective symptoms, neurobehavioral symptoms (irritability, anxiety), and communication ability. Each of the 9 areas was graded based on an ordinal response as: 0 for normal, 1 for mild impairment, 2 for moderate impairment, or 3 for severe impairment.
Three men with a history of TBI and active PTSD completed the trial. Mean age was 45 years; age range was 40-54. Compliance with the treatment protocol was excellent based on patient reporting and our ability to query the devices for a log of treatment times. All three patients enjoyed the treatments and stated that they looked forward to using the device. All patients were interested in continuing to use the device after the conclusion of the 4-week treatment regimen. No adverse events were reported related to device use.
The results of the evaluation based on the Veterans Affairs TBI Evaluation are shown in Table 1. All patients demonstrated overall improvement in their scores with the greatest effects noted in patients 1 and 3. Although patient 2 improved, his baseline total score was low suggesting that his symptoms related to TBI were minimal even at baseline. The greatest improvements were seen in patient’s subjective symptoms and orientation. The total scores at baseline compared to the conclusion of the trial are depicted in Figure 1.
| Category | Patient 1 Baseline - Conclusion | Patient 2 Baseline - Conclusion | Patient 3 Baseline - Conclusion |
| Memory | 3 - 1 | 2 - 2 | 3 - 2 |
| Judgement | 2 - 1 | 0 - 0 | 3 - 2 |
| Social Interaction | 2 - 1 | 0 - 0 | 3 - 2 |
| Orientation | 3 - 1 | 1 - 0 | 3 - 1 |
| Motor Activity | 2 - 1 | 0 - 0 | 3 - 2 |
| Visual Spatial Orientation | 3 - 1 | 0 - 0 | 3 - 2 |
| Subjective Symptoms | 3 - 1 | 2 - 1 | 2 - 1 |
| Neurobehavioral Effects | 3 - 1 | 0 - 0 | 3 - 2 |
| Communication | 2 - 1 | 0 - 0 | 3 - 2 |
| Total Score | 21 - 9 | 5 - 3 | 26 - 16 |
Table 1: Scores Obtained at Baseline and Conclusion of Treatments in 3 Patients with TBI and PTSD
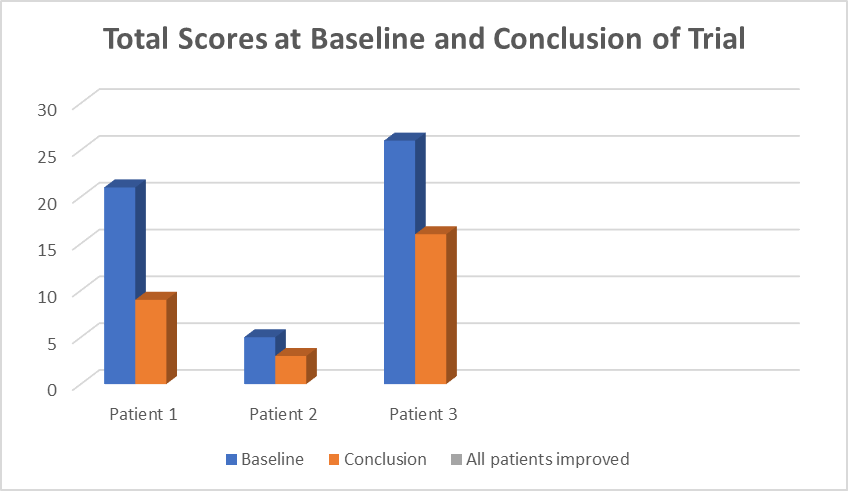
Figure 1: Bar graph comparing total scores at baseline and at trial conclusion
The relationship between TBI and symptoms of PTSD, depression, and anxiety has been well-described. [1-5] PTSD is a potentially disabling condition that appears to represent a form of anxiety disorder associated with hypervigilance and increased sympathetic output. [6-12] Although the mainstay of treatment for PTSD was originally pharmacologic, an increasing emphasis has been placed on psychological interventions and various relaxation techniques including yoga and deep breathing exercises. [8-12,15] Similarly, depression and anxiety are prevalent conditions with tremendous societal and personal costs [12-14].
Our previous work demonstrated a statistically significant improvement in symptoms of PTSD, anxiety, and depression with the use of PSS. [20,22] The scientific bases for such improvement may be related to the role played by sensory processing in anxiety, depression, and PTSD. PTSD has been associated with a variety of physiological alterations within the brain, and increasing evidence suggests that impaired sensory processing may play a critical role in the development and pathophysiology of this disorder. [23] Haricharichan et al postulated that alterations in the neural pathways important for processing sensory input have a cascading effect on the ability to perform higher cognitive functions implying that abnormal sensory processing may be contributory and associated with PTSD [24]. In addition, it has been shown that individuals with PTSD have decreased prefrontal cortex activation resulting in impaired sensory integration and emotional regulation [25-7]. Engel-Yeger et al identified reproducible patterns of sensory hypersensitivity in patients suffering from PTSD [28].
Interestingly, a variety of physiological alterations within the brain have been associated with anxiety and depression, and increasing evidence suggests that impaired sensory processing may play a critical role in these disorders [29-34]. Of note, various sensory inputs have been shown to impact symptoms in patients with depression and anxiety; auditory stimulation with music, olfactory stimulation with particular odors, and gustatory stimulation with particular foods have all been shown to improve mood and relieve anxiety [35-38]. Transcranial magnetic stimulation and vagal nerve stimulation have also been used to ameliorate anxiety and depressive disorders [39-40]. Based on these findings, we hypothesized that tactile PSS might be beneficial in patients with the mental health symptoms related to TBI.
It should be noted that PSS has been shown to be of therapeutic benefit in a variety of neurological disorders. PSS has shown promise in humans after stroke and also in rodent models of cerebral ischemia where PSS can actually prevent ischemic injury if applied early enough. [41-43]. The mechanism for this protection remains unclear but may include enhanced neuronal reorganization encouraging neuronal recovery and/or improved regional cerebral perfusion through the recruitment of local collateral blood supply [44]. Interestingly, similar benefits have been demonstrated in patients with Parkinson’s disease, and PSS has also shown promise following traumatic brain injury and in inflammatory, auto-immune conditions such as multiple sclerosis [45-49].
Based on this, we analyzed a small subgroup of 3 patients with PTSD and TBI who were treated with one month of PSS on a daily basis. All three patients were evaluated using the Veterans Affairs TBI Evaluation, and all showed improvement in their scores over the course of the 4-week trial. As noted above, patient 2 appeared to have minimal symptoms related to TBI and showed limited improvement. It is notable that the other two patients had significant impairment at baseline, and both showed meaningful improvement in their scoring by the conclusion of the trial.
We describe our experience with 3 patients with TBI who underwent one month of PSS treatment on a daily basis. This is a very small group of patients precluding significant conclusions regarding efficacy of PSS on patients with TBI. Nevertheless, this study was meant to evaluate in very preliminary fashion the potential usefulness of PSS in patients with TBI, potentially forming the basis for a larger study. All patients showed improvement in their symptoms suggesting that further investigation into the potential use of PSS in the treatment of patients with TBI is warranted.
The study was approved by the Western (WCG) Institutional Review Board (protocol code: 20233103, date of approval: 7/19/2023).
This study was registered with clinicaltrials.gov prior to initiation any work or patient enrollment. The trial number is NCT06050590.
Drs. Leslie and Eric Nussbaum are shareholders in Neuro Glove, LLC
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
