
Research Article | DOI: https://doi.org/10.31579/2641-0419/465
1Institute of Outcomes Research, Maria Sklodowska-Curie Medical Academy, ul. Żelaznej Bramy 10, 00-136 Warsaw, Poland.
2Department of Clinical Biochemistry, The Children's Memorial Health Institute, Aleja Dzieci Polskich 20, 04-730 Warsaw, Poland.
*Corresponding Author: Piotr Łojko, Institute of Outcomes Research, Maria Sklodowska-Curie Medical Academy, ul. Żelaznej Bramy 10, 00-136 Warsaw, Poland
Citation: Piotr Łojko, Aldona W. Rucińska, (2025), The Pivotal Role of the NT-proBNP Biomarker in Diagnosing Cardiac Dysfunction post- COVID-19, A Systematic Review and Meta-Analyses, J Clinical Cardiology and Cardiovascular Interventions, 8(7); DOI: 10.31579/2641-0419/465
Copyright: © 2025, Piotr Łojko. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 March 2025 | Accepted: 09 April 2025 | Published: 14 May 2025
Keywords: NT-proBNP; covid-19; cardiac dysfunction
NT-proBNP plays a key role in the diagnosis and monitoring of cardiac dysfunction in patients after COVID-19. Its use in clinical practice allows for early detection of complications, assessment of their severity and monitoring of treatment effectiveness. An increase in NT-proBNP levels, especially in patients with a severe course of COVID-19, requires a detailed cardiological evaluation, including imaging tests such as echocardiography or magnetic resonance imaging. Due to the increasing number of patients with cardiac complications after COVID-19, NT-proBNP is becoming an increasingly important diagnostic tool that helps doctors make therapeutic decisions and improve patient prognosis.
The SARS-CoV-2 virus affects the heart, even in patients who have been infected asymptomatically or with mild symptoms. In the face of a global pandemic that has affected millions of people worldwide, understanding the long-term effects of SARS-CoV-2 infection on the cardiovascular system has become a priority. NT-proBNP, previously known mainly in the context of heart failure diagnostics, has proven to be a valuable tool in detecting and monitoring cardiovascular complications associated with COVID-19 [1,2]. In this context, biomarkers such as NT-proBNP have become crucial for early detection and monitoring of potential heart damage. Their role in the care of patients after COVID-19 cannot be overestimated, especially in light of the increasing number of cases of the so-called "long COVID". NT-proBNP (N-terminal fragment of B-type natriuretic propeptide) has gained new, crucial importance as a biomarker in the diagnosis of heart dysfunction after COVID-19. NT-proBNP is produced by the breakdown of the prohormone BNP (brain natriuretic peptide), which is secreted by cardiomyocytes in response to increased stress on the heart wall. This process is key to understanding the role of NT-proBNP as a biomarker of heart dysfunction. When the heart is overloaded, whether due to increased blood pressure, excess fluid, or direct damage to the heart muscle, cardiomyocytes respond by increasing the production of proBNP. This prohormone is then split into two parts: the active hormone BNP and the inactive fragment NT-proBNP [3,4]. While BNP has physiological effects, helping to regulate blood pressure and fluid volume, NT-proBNP has no biological function. However, due to its longer half-life in the blood, NT-proBNP has become the preferred marker for diagnostic purposes. In the case of heart dysfunction after COVID-19, NT-proBNP levels can increase significantly, signaling heart muscle overload or damage. This increase may be due to the direct effect of the virus on heart cells, the body's inflammatory response, hypoxia associated with respiratory failure, or other pathophysiological mechanisms associated with SARS-CoV-2 infection [5,6]. The effect of SARS virus -CoV-2 on the human organism is closely linked to the membrane receptortore - converting enzyme 2 angiotensin (ACE2) and the renin-angiotensin-aldosterone (RAA) system. ransmembrane serin peptidase type 2 (TMPRSS2) assists in the active binding of viral envelope proteins to the host cell [7]. Expression of the ACE2 receptor has been demonstrated in many organs but the lungs are the main entry gateway for the SARS virus -CoV-2.4 In addition, membrane receptors for ACE2 are present in the vascular endothelium, myocytes and other organs, including the kidneys, increasing the likelihood of multi-organ damage[8]. ACE2 expression decreases with the moment the virus attaches. This leads to a local increase in angiotensin II (Ang II), which is a major subloss of ACE2, thus promoting stimulation of the RAA system. The exact mechanism of damage to the myocardium and vasculature (with particular-emphasis on the endothelium) by SARS virus -CoV-2 is under investigation [9]. A number of papers have observed an association between the cardiovascular system and cardiovascular disease, myocardial damage and death in patients with COVID-19. In a Chinese study of patients with COVID-19, 27% had elevated TnT levels, which showed myocardial damage [10,11]. In this group, mortality was significantly higher than in patients with normal TnT levels . It was noted that patients with underlying cardiovascular disease but with normal TnT levels during the course of the disease had a more favorable prognosis compared to patients with elevated TnT levels. The dynamic escalation of NT-proBNP and increased incidence of malignant arrhythmias over the course of the disease in patients with elevated TnT levels demonstrate that myocardial damage played a greater role in the fatal outcome of COVID-19 than the presence of underlying cardiovascular disease alone. Increased NT-proBNP levels and malignant arrhythmias were significantly more frequent in patients with elevated TnT levels, and NT-proBNP significantly correlated with TnT levels, suggesting that those with myocardial damage had cardiac dysfunction.
2.1.Selection criteria
Two independent reviewers (Piotr Łojko and Aldona Wierzbicka-Rucińska) analyzed all titles and abstracts, excluding minor studies. Studies that met the following conditions were qualified for analysis: (1) types of studies: retrospective, prospective, cross-sectional, observational, in which cardiac biomarkers (including NT-proBNP, CK, CK-MB, TnI, Myo or, LDH) were evaluated or the patient suffered acute cardiac injury due to COVID-19; (2) patient characteristics: patients should be diagnosed with COVID-19 and divided into moderate, severe or critical cases according to the protocol for diagnosis of new coronavirus-induced. Exclusion criteria were as follows: (1) types of studies: case reports, reviews, editorials, conference abstracts and discussion summaries, (2) patient characteristics: patients with a specific condition, such as oncological diseases.
2.2.Search strategy
This review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [7]. The scope of this systematic review was limited to clinical trials conducted in humans in the last 6 years (2019–2025). Six databases were selected for the literature search: Ebsco, Embase, Cochrane, Pub Med, Scopus, and Web of Science. The search and selection process was performed by two reviewers working independently and in parallel. Searches included a combination of MeSH terms and keywords, using quotation marks and field tags with BOOLEAN operators. Not all databases had the same query options (for example, selecting a clinical trial), so steps and phrases were created. Five primary exclusion steps were defined for all databases: (1) keywords (“NT-proBNP biomarker as cardiac dysfunction following COVID-19” OR “NT-proBNP and Covid 19” * OR NT-proBNP biomarker *); publication type (article); (4) language (English); (5) source type (journal). For nonmedical databases, the search was performed in the following areas: title, abstract, keywords (Scopus–Core Collection), topic (Web of Science–Medline), and Ebsco (all). The last search was performed in February 2025. Results from each database were exported to files with the appropriate CSV or Excel extension, and abstracts were created for each database containing publication information, including abstracts. The initial search yielded 23 studies. After removing publications and reviews in a language other than English and removing duplicates, 23 records were selected for abstract review. We did not exclude any publications according to the exclusion criteria, and the full text of 23 eligible studies was included—only studies involving human participants. Articles that reported genetic, pharmacological, or simulation studies were excluded from the review. Three independent reviewers reviewed the abstracts, and articles that did not meet the inclusion criteria were excluded through discussion. The literature search process is shown in Figure 1.
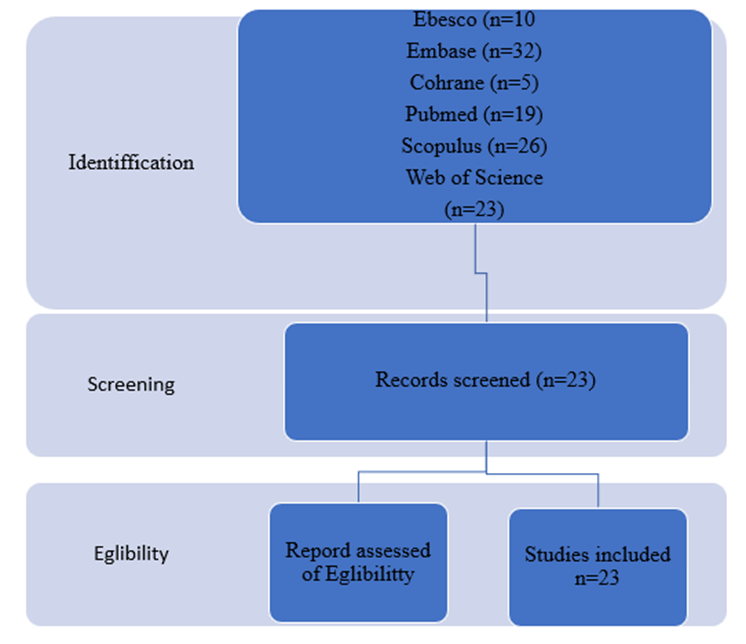
Figure 1: Identification of study via database.
Prisma flow diagram representing the screening strategy and selection process for research articles. Process of selecting eligible studies. We used the Jadad scale [8,9] to assess the quality and reliability of the study results in the selected clinical trials. According to the scale assumptions, attention was paid to three main categories: randomization (0 points for quasi-RCTs; 1 point if randomization was declared but without a detailed description of the generation of random numbers; 2 points if a valid method of generating random numbers was described), double-blind (0 points if blinding was not mentioned; 1 point if blinding was mentioned but efficacy was not described; 2 points if the study used a robust method, such as placebo, to ensure double-blindness), and withdrawals and abandonments (0 points if withdrawals were not described despite a smaller number of patients analyzed compared to those recruited). The Jadad scale classified scores of 0–2 as indicating low quality clinical trials, 3 as moderate quality, and 4–5 as high quality clinical trials.
NT-proBNP as a diagnostic tool in COVID-19 The studies by Caro-Codón et al. (2021) have significantly contributed to understanding the role of NT-proBNP as a diagnostic tool in the context of COVID-19[10]. They have shown that NT-proBNP is an extremely sensitive marker of myocardial damage in patients with COVID-19, even in cases where standard cardiological tests do not show visible abnormalities. Of particular importance is the fact that NT-proBNP can detect subclinical cardiac dysfunction. This means that this marker can signal heart problems before clear clinical symptoms or changes visible in imaging
studies appear. This property of NT-proBNP is extremely valuable in the context of COVID-19, where heart damage can develop slowly and initially asymptomatically. In addition, these studies have shown that NT-proBNP levels correlate with the severity of COVID-19 and the risk of cardiovascular complications. Patients with higher levels of NT-proBNP during the acute phase of the disease were more likely to develop serious complications, including heart failure, arrhythmia, and even death. COVID-19 can affect the heart through various mechanisms, and NT-proBNP plays a key role in detecting and monitoring these changes. The main mechanisms by which COVID-19 affects the cardiovascular system include:
NT-proBNP in monitoring heart dysfunction after COVID-19 The research by Sánchez-Marteles and colleagues (2024) has significantly advanced our understanding of the role of NT-proBNP in the long-term monitoring of patients after COVID-19 [11]. They showed that NT-proBNP is not only a valuable tool in the acute phase of the disease, but also during the convalescence period and long-term follow-up. Regular NT-proBNP measurements can help identify patients with progressive heart dysfunction, even in the absence of clear clinical symptoms [12,13]. This is particularly important in the context of “long COVID”, where cardiovascular complications can develop slowly and initially asymptomatically. These studies also showed that NT-proBNP levels can be a predictor of long-term outcomes in patients after COVID-19. Patients whose NT-proBNP levels remained elevated for a longer period after recovery from the acute phase of COVID-19 had a higher risk of developing chronic heart diseases, including heart failure. In addition, monitoring NT-proBNP can help assess the effectiveness of treatment. A decrease in NT-proBNP levels over time may indicate an improvement in heart function and the effectiveness of the applied therapy [14,15].
NT-proBNP Index:
An Improved Diagnostic Tool introduced an innovative concept of the NT-proBNP index, which significantly improved the diagnostic accuracy of this biomarker [16,17]. This index takes into account not only the absolute level of NT-proBNP but also the patient's age and gender, which allows for a more precise assessment of the risk of cardiac dysfunction after COVID-19. This concept is based on the observation that the normal level of NT-proBNP may vary with age and gender. For example, older patients and women tend to have higher NT-proBNP levels even in health [18, 19] and trails are summarized in the meta‐analysis, and their characteristics are presented in table 1.
| Study | Data | Study design | Region and Country | Diagnostic criteria | n | predicting 30-day mortality. |
| 4 | 2020/01–2020/02 | retrospective, observational study | Beijing, China | coronary artery disease | 85 | 31% |
| 6 | 1991/02- 1993/02 | prospective observational study | The Danish | patients with symptoms or signs of coronary artery disease | 1078 | 1,5-4% |
| 8 | January 1 to January 28, 2020 | single-center case | Wuhan, China | novel coronavirus (2019-nCoV)-infected pneumonia (NCIP) | 138 | 4,3% |
| 15 | March 1st to April 20th, 2020 | observational study | Madrid, Spain | myocardial injury | 918 | 1,57–4,04 |
| 16 | February 27 to April 7, 2020 | single-center prospective study | Barcelona, Spain, | patients were diagnosed with COVID-19 | 923 | 7,4% |
| 17 | 2008-2012 | multi-center prospective study | USA | Patients with myocardial infarction with nonobstructive coronary arteries (MINOCA) | 2690 | 1-1,7% |
| 18 | January 20, 2020, to February 10, 2020 | single-center prospective study | Wuhan, China | patients with COVID-19 | 416 | 3,41% |
| 20 | 1987- 2013 | trial-level analysis of 16 phase III chronic HF trials | USA, Europe | heart failure (HF) | 48844 | 5% |
| 21 | 2003-2013 | observational study | Sweden | Patients with myocardial infarction with nonobstructive coronary arteries (MINOCA) | 9136 | 0,63-1,5% |
| 23 | 2020-2022 | retrospective analysis | China | patients diagnosed with COVID-19 | 2917 | 3,90% |
Table 1: The characteristics of the included studies
The NT-proBNP index takes into account these differences, allowing for a more personalized interpretation of the results. The NT-proBNP index is calculated by dividing the measured NT-proBNP level by the upper limit of the normal range for a given age and gender. An index value above 1 suggests an increased risk of cardiac dysfunction, with higher values indicating a higher risk. Studies have shown that NT-proBNP is a better predictor of clinical outcomes than absolute NT-proBNP values alone, especially in older patients. It can help identify high-risk patients who may require more intensive monitoring and treatment [20,21]. Challenges in Interpreting NT-proBNP Results Despite its diagnostic value, the use of NT-proBNP in the assessment of cardiac dysfunction after COVID-19 is associated with certain challenges that must be considered when interpreting results:
1. Nonspecificity of the marker: NT-proBNP levels may increase not only in heart disease but also in other conditions such as renal failure, hyperthyroidism, and chronic obstructive pulmonary disease. Therefore, it is important to interpret NT-proBNP results in the context of the patient's complete clinical picture.
2. Influence of age and gender: As mentioned earlier, the normal range of NT-proBNP levels may vary by age and gender. Older patients and women tend to have higher NT-proBNP levels, which must be considered when interpreting results.
3. Differences in measurement methods: Different laboratories may use different methods to measure NT-proBNP, which may lead to some discrepancies in results. It is important to consider the measurement method when comparing results.
4. Influence of other factors: Factors such as obesity, anemia, or the use of certain medications may affect NT-proBNP levels. This should be kept in mind when interpreting results.
5. Dynamics of change: A single NT-proBNP measurement may not be sufficient for a complete risk assessment. It is important to monitor changes in NT-proBNP levels over time.
Analysis of biomarkers (markers of myocardial damage, inflammation and prothrombotic status) in SARS-CoV-2 infected patients with pre-existing cardio-vascular disease is currently the subject of research and discussion. However, the importance of myocardial damage, defined as cardiac troponin levels above the 99th percentile of the normal range, regardless of new electrocardiographic and echocardiographic abnormalities, during SARS-CoV-2 infection is emphasized. Elevated troponin levels (myocardial damage) and a positive correlation between hs-TnI levels and mortality. was observed in elderly patients and burden of cardiovascular disease, such as hypertension (59.8% vs. 23.4%), diabetes (24.4% vs. 12.0%), ischemic heart disease (29.3% vs. 6.0%), cerebrovascular disease (15.9% vs. 2.7%) and heart failure (14.6% vs. 1.5%) [30]. Patients with cardiovascular disease and other comorbidities are at greater risk of myocardial damage during COVID-19. In patients with cardiovascular disease, including hypertension, coronary artery disease and cardiomyopathy, viral disease can further damage myocardial cells through several mechanisms, including direct damage by the virus, systemic inflammatory reactions, destabilization of the coronary plaque and increased hypoxia [31].
Although the exact pathophysiological mechanism underlying COVID-19-induced myocardial damage is not fully understood, it draws attention to the possibility of direct damage to cardiomyocytes by SARS-CoV-2 virus. Viral particles spread through the respiratory mucosa and simultaneously infect other cells, which can trigger a cytokine storm and a range of immune responses. Highlighted that in patients with COVID-19, an imbalance of T helper 1 and T helper 1 responses caused a cytokine storm that can contribute to myocardial damage. The release of inflammatory cytokines after infection can result in reduced coronary blood flow, reduced oxygen supply, coronary plaque destabilization and microthrombogenesis [32,33]. NT-proBNP peptide has been recognized as an effective biomarker not only for diagnosis and risk stratification, but also for treatment optimization and prognostic evaluation in patients regardless of HF classification. Higher levels of NT-proBNP in patients on admission were associated with a worse prognosis, while lower levels of NT-proBNP reflected relatively better myocardial health. As NT-proBNP is released by the myocardium, it is thought to affect the activation of the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system. Studies have shown that NT-proBNP levels were strongly correlated with left ventricular dimensions, volumes and functions, and were seen as useful tools for identifying actual cardiac hemodynamic conditions.
The role of NT-proBNP in the diagnosis and monitoring of cardiac complications after COVID-19 is still evolving. Further research in this area may contribute to: Establishing optimal cut-off points for different patient groups: Further studies are needed to determine the optimal NT-proBNP thresholds for different age and gender groups in the context of COVID-19. Developing algorithms combining NT-proBNP with other biomarkers: Combining NT-proBNP with other markers, such as troponin or CRP, may increase diagnostic and prognostic accuracy. Creating personalized strategies for monitoring patients after COVID-19. Studies may help develop individual monitoring protocols based on NT-proBNP levels and other risk factors. Better understanding of the long-term effects of COVID-19 on the heart. Long-term studies using NT-proBNP may help understand how COVID-19 affects the heart in the long term. Development of new therapies: Understanding the role of NT-proBNP may lead to the development of new strategies for the treatment of cardiac complications after COVID-19.
NT-proBNP has proven to be an extremely valuable diagnostic tool in the assessment of cardiac dysfunction after COVID-19. Its use allows for early detection of cardiac complications, optimization of treatment strategies and monitoring of patients in the long term after infection. Key advantages of using NT-proBNP in the context of COVID-19 include: Early detection of subclinical cardiac damage. Ability to predict the severity of COVID-19 and the risk of complications. Help in monitoring disease progression and treatment efficacy. Ability to identify patients requiring long-term cardiac care. Further research on this biomarker may contribute to a better understanding and treatment of cardiac complications associated with COVID-19, which may have great public health implications in the post-pandemic era. As our knowledge of the long-term effects of COVID-19 increases, the role of NT-proBNP as a key tool in the care of patients after COVID-19 will likely become increasingly important.
None declared
Conceptualization PŁ, AWR.; methodology PŁ, AWR,: validation, PŁ, AWR ; formal analysis, P.S and AWR. writing—original draft preparation, PŁ, AWR supervision, PŁ, AWR All authors have read and agreed to the published version of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
