
Research Article | DOI: https://doi.org/10.31579/2641-0419/157
*Corresponding Author: Hammam Shereef, MD. Department of Internal Medicine. Beaumont Health – Dearborn 18101 Oakwood Blvd, Dearborn, Michigan, 48124
Citation: Hammam Shereef., Ahmed S Yassin., Mowyad Khalid., Omeralfaroug Adam., Hossam Abubakar., (2021) The Medico-economic Impacts of Marijuana Use on the Outcomes and In-hospital Mortality in Patients with Atrial Fibrillation – Nationwide Database study. J. Clinical Cardiology and Cardiovascular Interventions, 4(11); DOI:10.31579/2641-0419/157
Copyright: © 2021 Hammam Shereef, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 March 2021 | Accepted: 20 May 2021 | Published: 27 May 2021
Keywords: atrial fibrillation; marijuana smoking; outcomes; mortality; length of stay; cost of hospitalization; nis database
Introduction
Cannabinoid users are at high risk of developing atrial arrhythmias. We sought to investigate the outcomes and the economic impact of marijuana use on patients with atrial fibrillation utilizing the National Inpatient Sample.
Materials and Methods
Patients with atrial fibrillation were identified in the National Inpatient Sample (NIS) database between 2012 and 2014 using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), who subsequently were divided into two groups, those with and without marijuana smoking. The primary outcome was all-cause in-hospital mortality in the two groups. Secondary outcomes were in-hospital morbidities, required procedures and complications. We also evaluated the length of hospital stay and the cost of hospitalization. Logistic regression model was performed to address potential confounding factors.
Results:
The marijuana-users group had no significant increase of in-hospital mortality (OR: 1.24; 95% CI: 0.51 - 3.01, p = 0.632). However, marijuana users were predominantly younger males and less likely to undergo cardiac surgery (OR: 0.54, 95% CI 0.37 - 0.78, p = 0.001). Moreover, marijuana users are more likely to have a lower cost of hospitalization when compared to non-users ($28,916 vs $32,303, p = 0.001).
Conclusion:
Cannabinoid use was not associated with an increase in mortality among patients admitted with atrial fibrillation. However, marijuana users were younger, had fewer comorbidities, and cardiac surgeries with associated lower hospitalization costs. Admittedly, given the growing popularity of these products, further large prospective studies are needed to investigate the safety and evaluate different integral associations of cannabis use with worse cardiac outcomes in atrial arrhythmias patients, particularly those with atrial fibrillation.
Atrial fibrillation is the most common documented cardiac arrythemia that is known to be associated with adverse outcomes across multiple large studies, with almost twice the risk of cardiovascular events including mortality[1-3]. Very little is known about the impact of marijuana smoking in patients with atrial fibrillation. Currently, Cannabinoids are being used as therapeutic agents for many medical conditions [4], it’s illegal use for decades is well recorded but less studied. Nowadays, we are moving toward legalization of these agents and the number of users is increasing by the day, especially among young and middle-age populations. The safety of marijuana needs to be established and challenged prior to its full legalization. Many studies were conducted to evaluate marijuana effect on cardiovascular system [5-7]. De Filippis et al. conducted a retrospective study in adults over 50 years old who presented with acute coronary syndromes (ACS), around 10% of the patients with STEMI had recently used cocaine or marijuana, and these patients were associated with worse all-cause mortality compared to patients without use [5]. Rezkalla et al. report in 2018 discussed the temporal relationship between marijuana use and a variety of cardiovascular events, where they reported effects like atrial fibrillation, ventricular tachycardia, acute coronary syndromes, congestive heart failure, accelerated hypertension, cerebrovascular disease, and even sudden death [7,8]. Yet the current evidence appears to be insufficient to conclude the effects of marijuana smoking on cardiovascular events. In our study, we aimed to evaluate the impact of marijuana smoking on the outcome of patients with atrial fibrillation.
Data source:
We conducted our study utilizing the National Inpatient Sample (NIS) database in the period between 2012-2014. The NIS is considered the largest all-payer database of in-hospital stays in the United States, developed by the Agency for Healthcare Research and Quality (AHRQ) as part of its Healthcare Cost and Utilization Project (HCUP) initiative [9]. The NIS includes more than seven million unweighted hospitalizations per year. Discharge weights provided within the database can be applied. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) coding used to provide 25 to 30 discharge diagnoses, depending on the year and 15 procedures on each hospitalization. NIS discharge records include diagnoses, basic demographics, procedures, insurance payers, length of stay, hospital characteristics, and hospital charges. As the data collected from NIS, no IRB approval was required to be obtained.
Variables and outcomes:
NIS registry discharge from 2012 to 2014 studied in a retrospective cohort fashion. We used validated ICD-9 codes to include adults (≥18 years) hospitalized with a principal diagnosis of Atrial fibrillation. (Table 1) depicts the ICD-9 codes used. Patients’ demographics and baseline clinical characteristics are shown in (Table 2). Charlson comorbidity index calculated for comorbidities. Atrial Fibrillation patients with Marijuana use were compared to patients without Marijuana in characteristics, length of stay, acute kidney injury (AKI), venous thrombo-embolism (DVT/PE), ICU admission, cardiogenic shock, ventricular arrhythmias, cardiac arrest, need for permanent pacemaker, open-heart surgeries, and other vascular and cardiac complications. The primary outcome is in-hospital mortality.
Statistical analysis:
We used STATA 15 (Stata Corp, College Station, Texas, USA) to perform statistical analyses in our study sample. Categorical variables are expressed in percentages and continuous outcomes reported in mean +/- standard deviation (SD). We utilized Discharge weights and excluded patients with missing data. Chi-square test and student’s t-test used for categorical and continuous variables, respectively. To compare groups, we used logistic regression model for categorical outcomes, and linear regression for continuous outcomes. Statistical significance was determined based on the p-value of < 0.05. For outcomes, numeric results reported as mean and binary outcomes reported as an odds ratio.
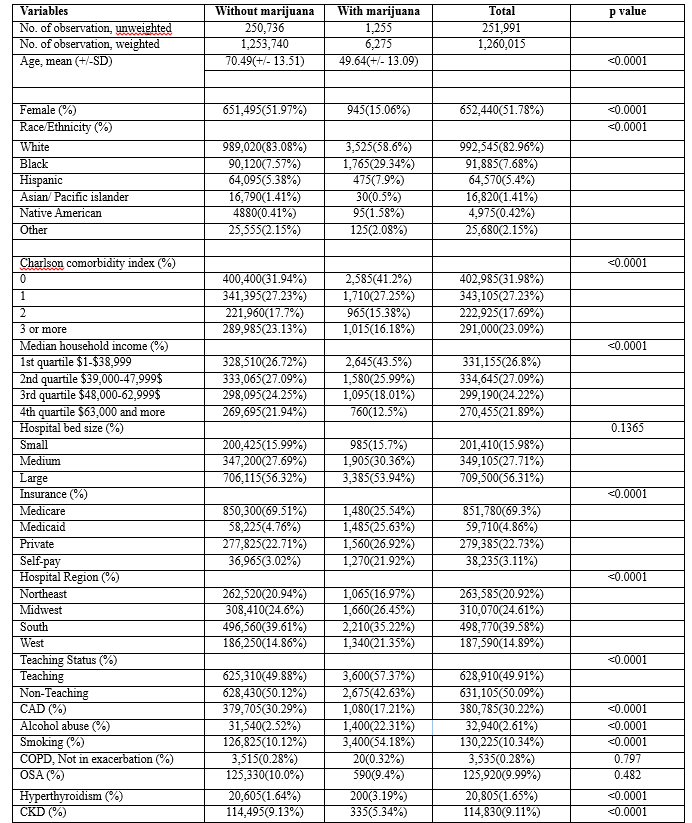
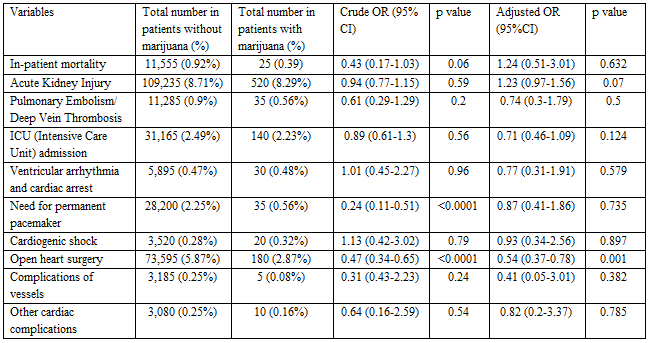
We studied 1,260,015 patients from the NIS registry between 2012 and 2014; patients were all hospitalized with principal diagnosis of atrial fibrillation divided into two cohorts with and without use of marijuana. We found a mean age of 70 ± 13 years in the non-marijuana users arm compared to significantly younger patients’ population in the marijuana use arm with mean age of 49 ± 13 years. Female to male ratio was calculated as 1:1 in the overall study subjects, yet more male predominance was found in the atrial fibrillation marijuana arm accounting for 84.94%. Our study claimed majority of white populations followed by African Americans followed by Hispanics with 82.96%, 7.68%, and 5.4% respectively, however we noted a higher percentage of African Americans and Hispanics in atrial fibrillation marijuana cohort as compared non-marijuana cohort; 29.34%, and 7.9% respectively. In analysis of patient’s geographical distribution, it was noted that majority of them were admitted to south region hospitals followed by Midwest then Northeast followed by west region; 39.58%, 24.61%, 20.92% and 14.89% respectively. We also depicted that more than two thirds of sample covered by Medicare, followed by private insurances followed by Medicaid: 69.3%, 22.73% and 4.86% respectively. Charlson’s index reported more than two-thirds of study subjects to have more than one co-morbidity and in further subgroup analyses we were able to show more frequencies of tobacco smoking, alcohol abuse and hyperthyroidism in marijuana users with atrial fibrillation versus non-marijuana group (54.18% tobacco smoking, 22.31% for alcohol abuse and 3.19% for hyperthyroidism compared to 10.12%, 2.52% and 1.64% respectively), however less frequencies of coronary artery disease (CAD) and chronic kidney disease (CKD) observed in the marijuana users compared to non-users (17.21% for CAD and 5.34% for CKD in comparison to 30.29% and 9.13% in the non-users group) all baseline demographics and clinical characteristics shown in (Table 1). After adjusting for patient-level characteristics, the crude and adjusted odds ratio by logistic regression model between the two groups in (Table 2), showed no significant statistical difference in in- hospital mortality between the two groups (OR 1.24; 95% CI: 0.51-3.01, P = 0.844). However, in regards to secondary in-hospital outcomes analysis we elicited fewer incidences of open-heart surgeries in marijuana cohort (OR 0.47; 95% CI: 0.37-0.78, P = 0.001). The length of hospital stay was not found to be statistically significant, however our data showed less hospital expenditure documented in marijuana admissions after adjustment for inflation; 28,916 USD as opposed to 32,303 USD in non-marijuana (Table 3).

Although some studies provided evidence that cannabinoids have noticeable hemodynamic and possible arrhythmogenic effect, the impact of marijuana smoking on clinically significant arrhythmias remains unclear. The most reported finding is tachycardia that lasts few hours after smoking, due to possible enhanced sinoatrial tissue automaticity and reduced parasympathetic tone [10-12]. In one study utilizing the National Inpatient Sample (NIS) database, it was found that cannabis use has been linked to increase inpatient admissions with arrhythmias [13].
Our study aimed to evaluate the impact of marijuana use in atrial fibrillation population using a (NIS) database. The usage of such databases allow for inclusivity of larger number of patients and utilization of logistic regression model will allow correcting for confounders. Also, the clinical relevance of such study is important considering the increased thromboembolic risk associated even with short periods AF, especially in patients with other risk factors for thromboembolism [14]. Recent report by Desai et. al. has used NIS to study marijuana-smoking relation to atrial arrhythmia as a whole than a specific type in particular [15]. Korntzopoulos et al, speculated a possible mechanisms of marijuana smoking causing AF, summarizing multifactorial scheme of neurohormonal factors and flow effects as sympathetic system activation, ischemia, impaired coronary microcirculation, increased pulmonary vein ectopy, enhanced atrial electrical remodeling, and increased dispersion of refractoriness [16]. From this we concluded that marijuana smoking impact of patients with atrial fibrillation warrants further studying and evaluation.
Our study showed that there is no increase in in-hospital mortality among marijuana smokers when they present with atrial fibrillation. However, most of the marijuana users were younger and with less co-morbidities. Another issue that the marijuana smoking status might be more prevalent in the labeled nonsmokers’ group than reported, this is since not all smokers would admit usage and marijuana urine testing is not routinely conducted in clinical settings outside the scope of employment screening.
It’s not completely clear why the marijuana smoking group requires less open-heart surgeries, possibly their young age, and their scarce co-morbidities especially the lower rates of coronary artery disease (CAD) incidence noted in the baseline characteristics. Same group was also found to require lower cost of hospitalization that can be explained by their less complexed admission compared to more older individuals who require more aggressive therapies including procedures, surgeries, and intensive care stay.
There are several recognized limitations of our study to be considered. First, the NIS database does not capture variables related to atrial fibrillation (e.g., CHADVAS score, chronicity, underlying structural heart disease, atrial diameter, previous trails of cardioversion or ablation) and marijuana smoking (e.g., chronicity, poly-substance use) or the treatment provided to the patients. Second, the use of a registry database to calculate the prevalence and the impact of marijuana smoking is well known to be at risk of coding errors. Various studies have shown that disparities in coding practice and documentation can significantly affect the observed prevalence and outcome of any condition in the NIS database. Finally, the outcome data are limited to in-hospital events and long-term impact and outcomes could not be assessed. Despite these recognized limitations, the NIS database is a valuable tool and has been widely used and validated.
Cannabinoid use was not associated with an increase in mortality among patients admitted with atrial fibrillation. However, marijuana users were younger, had fewer comorbidities, and cardiac surgeries with associated lower hospitalization costs. Admittedly, given the growing popularity of these products, further large prospective studies are needed to investigate the safety and evaluate different integral associations of cannabis use with worse cardiac outcomes in atrial arrhythmias patients, particularly those with atrial fibrillation.
Conflict of interest: None of the authors have any conflicts of interest to declare.
Disclosure of funding: None of the authors have any source of funding to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
