
Research Article | DOI: https://doi.org/10.31579/2641-0419/057
1 Department of cardiovascular diseases, Faculty of Medical Sciences-LU, Beirut, Lebanon.
3 Medical students, Faculty of Medical Sciences-LU, Beirut, Lebanon.
4 Department of Internal Medicine diseases, Faculty of Medical Sciences-LU, Beirut, Lebanon.
5 Department of Infectious Diseases, Head of Internal Medicine Department of MEIH affiliated with the Faculty of Medical Sciences-LU, Bsalim, Lebanon
*Corresponding Author: El Murr Tony, MD, Department of Infectious Diseases, Head of Internal Medicine Department of MEIH affiliated with the Faculty of Medical Sciences-LU, Bsalim, Lebanon.
Citation: Boutros Y, Abi R. Nagi ., George B., Ricardo W., Joelle F., El M. Tony (2020) The Lebanese Geitawi Hospital-University Medical Center Heart Failure Registry. J. Clinical Cardiology and Cardiovascular Interventions, 3(5); Doi:10.31579/2641-0419/057
Copyright: © 2020 El Murr Tony, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 March 2020 | Accepted: 20 March 2020 | Published: 27 March 2020
Keywords: heart failure; registry; awareness; indicators; TTE; variables; quality improvement.
Heart Failure (HF) has become a major cause of death and hospitalization among people older than 60 year. Lack of available data and registries from different countries that may aid in understanding the burden of the disease does exist.
The aim of the lebanese Geitawi Hospital-University Medical Center (LGH-UMC) heart failure registry is to point toward the incidence of heart failure, in patients with suspected dyspnea, during a 7 months period in a single university medical center based on Trans-thoracic echocardiography (TTE) findings with emphasis on its etiology.
Study population
The LGH-HFR includes inpatients and outpatients (≥18 years) presenting for further evaluation of possible HF by performing a TTE after suspicious clinical findings. Patients with clinical impression of possible heart failure were reported to LGH-HFR by their doctors.
The final decision to register a patient in the LGH-HFR is made by a single cardiologist to ensure the validity of the clinical suspicion. Approximately 1422 patients with clinically suspicion HF were registered in the LGH-HFR between 1.1.2018 and 31.7.2018.
Main variables and descriptive data
Our study will be a retrospective cohort analysis of data collected from the LGH-HFR between 1.1.2018 and 31.7.2018. Our number of studied patients is about 1422. The main variables recorded in the LGH-HFR are related to the TTE findings: LVEDV, LVEF, presence of LVH, the presence of diastolic dysfunction, documentation of any valvulopathies, measurements of PAPs. Furthermore, pro-BNP level and basic patient characteristics (age and sex) will be recorded.
The findings then will be pooled according to the documentation of heart failure, either systolic or diastolic. Furthermore, specific TTE findings will be mentioned in each case after correlation with the HF type pointing toward the possible etiology of the cardiac function degradation.
Results of our study will be reported back to clinicians to promote awareness for HF and communicated with the HFRs of different hospitals and LSC in order to optimize the standards of care regarding HF and discussing the cost effectiveness issue if possible.
Conclusion
The LGH-HFR is a valuable tool for continuous improvement of quality of care in patients and awareness regarding HF in Lebanon. Furthermore, it will be an important resource for the Lebanese registry-based HF research once available.
Heart failure (HF) is an heterogeneous clinical syndrome in terms of symptoms (dyspnea, orthopnea, lower limb swelling), signs (elevated jugular venous pressure, pulmonary congestion), associated structural and/or functional cardiac dysfunction that may result in reduced cardiac output and/or elevated intracardiac pressures [1]. Both prevalence and mortality rate of HF have remained unacceptably high making its early detection so crucial in order to decrease the disease burden. Based on an 2013 update from the American Heart Association (AHA) we concluded that there were 5.1 million people with HF in the United States in 2006 [2] and 23 million people with HF worldwide [3]. These numbers reflect not only a major health issue but make HF a prime subject for cost/effectiveness debate. For example, its total annual expenditures in the USA are expected to rise to $70 billion by 2030 [4].
Despite improvements in medical therapy and techniques, the extent of this disease has not been identified with precision because the lack of population based studies or global heart failure registries that may point toward specific etiologies or medical therapy regimen leading to a new perspective to deal with this world health issue. In spite of the fact that there is no clear cut estimation, the prevalence of HF according to several studies is approximately 1–2% and rises to >10% among people over the age of 70 years [5]. These data were supported by the Framingham Study showing us that the prevalence of HF in men aged between 50 and 59 years is 8 per 1000, increasing to 66 per 1000 at ages 80 to 89 years; add that similar results exist in women [6]. The incidence of HF, as its prevalence, increases with age too as described by the same study (figure 1). For instance, the predicted number of new HF cases in the USA by 2040 will be around 774,000 raising the alarm for working on new policies in order to prevent and decrease the burden of this disease [7].

Data from Lloyd-Jones DM, Leip EP, Larson MG, et al. Circulation 2006; 113:791.
Graphic 69663 Version 2.0
Signs and symptoms of heart failure consist of a wide range of manifestations that reflect either a decrease in heart contractility or conditions where demands overcome the ability of the heart to pump enough blood. One of the most common symptoms is shortness of breath which intensity may point toward a progressive decline in the left ventricle function.
The breathlessness occurring in heart failure patients has some features that make it well defined from other conditions which may lead to the same clinical profile. First, it occurs upon exertion and then it appears in recumbent position necessitating head elevation (by increasing the number of pillows while sleeping for example), progressing to paroxysmal nocturnal dyspnea not easily relieved by changing positions, ending up at rest interfering with daily life occupations .Other manifestations include palpitations, chest pain, pulmonary edema, confusion, oliguria found in patients as the disease progresses with markedly reduced left ventricular function.
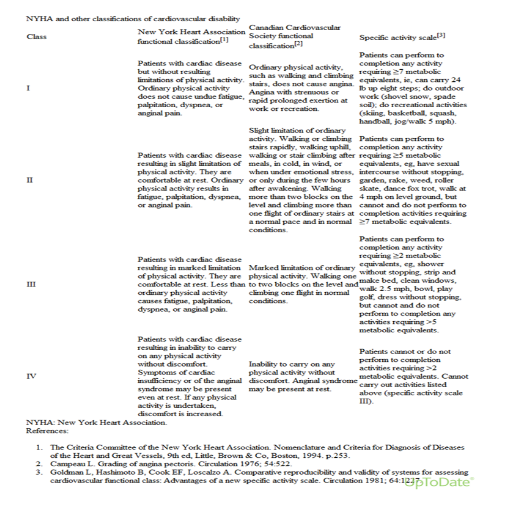
Concerning heart failure classification and staging, different systems have been issued making its diagnosis and prognosis easier to predict. The New York Heart Association (NYHA) for heart failure has four classes according to the degree of effort needed to provoke symptoms (table 1), complemented by the American College of Cardiology/American Heart Association
(ACC/AHA) heart failure stages that classify patients in four stages based on the presence or absence of a structural heart disease (figure 2).

Moreover, diagnosis of heart failure should be supported by objective data that confirm our clinical suspicion. It consists of complete blood count (CBC), serum iron level, electrolyte levels, and hepatorenal function studies. CBC (which usually is of little diagnostic help) may reveal a severe anemia causing or aggravating heart functions [8,9]. Serum iron deficiency is associated with a poor outcome and may lead to further deterioration in patient’s conditions by impairing the contractility of cardiomyocytes as stated by different experts opinions and published in a study establishing the fact that transferrin saturation (TSAT) up to 19.8% or a serum iron level up to 13 μmol/L were the cut points for selecting patients with the highest mortality rate associated with low serum ferritin level [10,11,12].
Some electrolytes disturbances may point also toward a regression in heart capacities. For example, dilutional hyponatremia (due to severe water retention and strict sodium restriction) or hyperkalemia (due to deterioration in kidney functions). Add that different factors can contribute to a reduction in GFR in patients with HF, including neurohormonal axis, renal hypoperfusion, increased renal venous pressure, and right ventricular dysfunction. Both lower GFR and higher blood urea nitrogen (BUN) have been associated with increased mortality in HF and make the diuresis of these patients a big issue [13-16].
Congestive hepatopathy is proven to be also an indicator of an increased risk of death in patient known to have HF. Usually it manifests by an elevation in serum concentration of total bilirubin (<3mg/dL) or mild elevation of LFTs and alkaline phosphatase [17].
In some cases, diagnosing HF appears to be challenging, that’s why more sophisticated testing would be highly recommended. So rapid measurement of B-type natriuretic peptide (BNP) or N-terminal proBNP (NT-proBNP) levels can guide clinicians in differentiating between cardiac and noncardiac causes of dyspnea especially upon atypical presentations. Usually, the major source of BNP is cardiac ventricles secreted after an overload in ventricular pressure or volume. Some studies have showed that BNP level aids in differentiating between systolic and diastolic heart dysfunction but contradictory data mention that it does not reliably differentiate between heart failure with preserved ejection fraction and heart failure with reduced ejection fraction [18-24]. In our study, we will correlate the level of serum pro-BNP to either systolic or diastolic heart failure based on TTE.
Chest radiography helps in supporting our diagnosis of HF by assessing the size and shape of the cardiac silhouette and edema at the lung bases knowing that 50% of patients with heart failure and documented elevation of pulmonary capillary wedge pressure (PCWP) do not manifest typical radiographic findings of pulmonary congestion.
One of the most used diagnostic tool in cardiac diseases is the EKG. In HF, there is no specific EKG findings. Q waves, non specific ST-T wave changes may be present in patients who suffer from a cardiomyopathy or already diagnosed with a prior myocardial infarction .
In addition to all of the above , two-dimensional (2-D) echocardiography is recommended in the initial evaluation of patients with known or suspected heart failure [18,19]. Doppler imaging helps also in further assessment of diastolic heart dysfunction and it is a main clue in the whole diagnostic process as almost 50% of patients presenting with symptoms highly suggestive of HF have normal systolic function. The primary finding, based on TTE, that helps us to differentiate between systolic and diastolic HF is the EF. This detection is so crucial and done by taking accurate measurements while performing the echography in order to target different etiologies so that we can discuss appropriate therapy with our patient.
Other features discovered while performing Doppler and 2D-echocardiography are ventricular filling and pulmonary artery pressures, heart cavity diameters and volumes, LV systolic and diastolic function, valvular anatomy and kinetics.
Add that, transesophageal echocardiography (TEE) may be very useful in conditions where TTE is not diagnostic or technically difficult to perform (patients morbidly obese or on mechanical ventilation) [18]. Its helps us then to assess accurately the heart kinetics, EF, valvular motion, any abnormal communication between cavities leading us to an unambiguous diagnosis.
Multiple heart failure registries have been conducted in different countries but an effort should be made in order to have a global HF registry so that we can understand this disease burden and help in improving patients conditions after studying the effect of different factors (age, sex, race, prevalence, adherence to therapy, length of hospital stay…) during the whole process.
For instance, a heart failure registry in Asia published in the journal of cardiac failure (volume 22, Issue 9, Supplement, Page S153) showed that HF in Korea is a serious condition with in hospital mortality rate of 5%, length of hospital stay in the hospital around 9 days and 1-year mortality rate of 20%.
Another Heart failure registry done in Denmark has shown a substantial improvement in the DHFR process indicators from 2003 to 2010 among patients diagnosed with incident HF. In the same period, the 1-year mortality decreased from 20.5% to 12.8% [25]. The same registry has shown that HF in elderly population (>75years) is not diagnosed and treated adequately.
In our study, we correlate different TTE findings (LVEDV, LVEF, presence of LVH, the presence of diastolic dysfunction, documentation of any valvulopathies, measurements of PAPs) and pro-BNP level in order to estimate the percentage of HF and its possible etiology during a 7 months period so that we can initiate a nucleus for a heart failure registry in our university medical center and hopefully nationwide
We retrospectively analyzed the results of 1520 TTE performed for 1422 patients between January and July 2018 in a university medical center in order to assess the prevalence of HF and its possible etiology in patients with clinical suspicion of HF.
The data was collected from the medical records department of our tertiary care center in Lebanon (Lebanese Geitawi Hospital-University medical center), regardless sex, age or any other condition.
Our data was taken from hospital EMF at the echocardiography lab. Then we plotted all these data on an excel sheet and statistically analyzed them using SPSS according to different TTE parameters, age, sex and pro-BNP level.
All TTEs were done using the same machine “Vivid E9 General Electric” and performed by different cardiologists.. All retrieved and consolidated data were then statistically analyzed.
HF documentation was done using TTE findings correlated to the pro-BNP level of the same patient.
Most of the TTEs were performed using same technique and when necessary, more sophisticated visual assessment done by experts.
Most of the measurements were repeated many times once in doubt and pro-BNP level ordered in many patients for further investigation and documentation of the heart dysfunction.
The number of TTE analyzed for possible HF between January and July 2018 was 1520 cases. The majority was complete in term of necessary data to document HF. Data were plotted into the excel sheet then analyzed more sophistically using IBM SPSS statistics software version 22 according to different parameters (LVEDV , LVEF , presence of LVH , the presence of diastolic dysfunction , documentation of any valvulopathies , measurements of PAPs , pro-BNP level). Means, frequency, cross-tabulation tables were then generated based on chi-square Theory to detect the correlations.
The study population was of 1422 patients and 68 with full data.
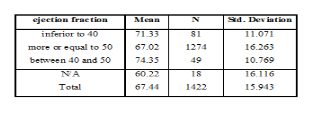
Patients age ranged between a minimum of 18 years and a maximum of 99 years, with a mean of 67.44 years (n=1422) and a standard deviation of 15.943.
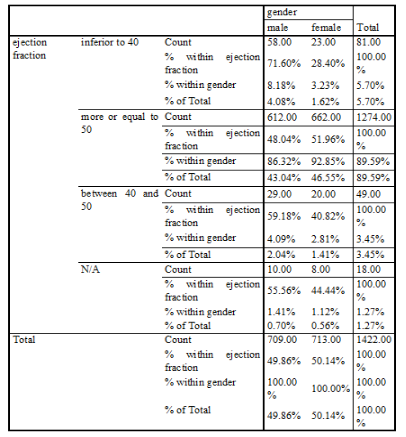
There were 709 males (49.86%) and 713 females (50.14%).
Out of the 1422 patients, 5.7% of our patients have an EF less than 40%, 89.59% have an EF more than 50%, 3.45% have an EF ranging between 40 and 50%, 1.27% of patients had no cut value for the EF.
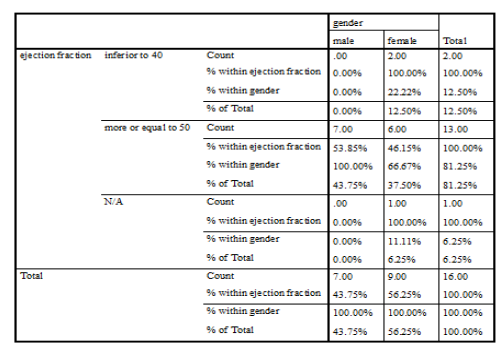
For the group of patients with EF less than 40% (HFrEF), their mean age was 71.33 years with a SD of 11.071 and 71.6% were male while 28.4% were female. Their distribution on our studied parameters is as the following:
For the group of patients with EF more or equal to 50% (HFpEF), their mean age was 67.02 years with a SD of 16.263 and 48% were male while 52% were female. Their distribution on our studied parameters is as the following:
For the group of patients with EF ranging between 40 and 50%, their mean age was 74.35 years with a SD of 10.769 and 59.2% were male while 40.8% were female. Their distribution on our studied parameters is as the following:
Our records showed that 16 of our patients had prosthetic valves, 10 of them aortic while the remaining were mitral. Among these patients, the minimum age was 31 and the maximum age was 87. Thus, 43.8% were male while 56.3% were female. Their distribution on our studied parameters is as the following:
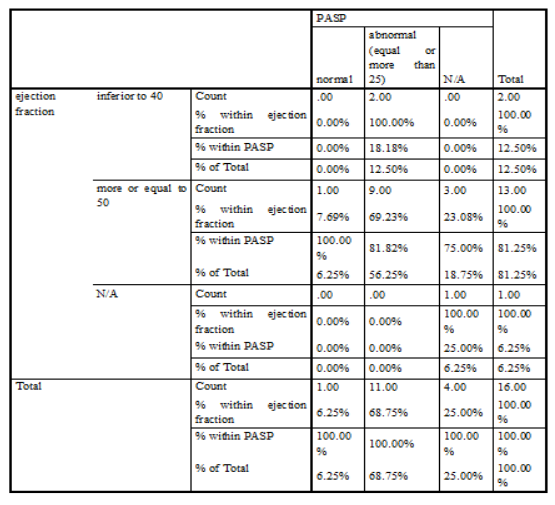
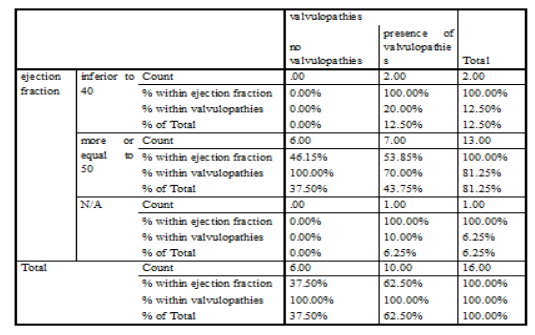
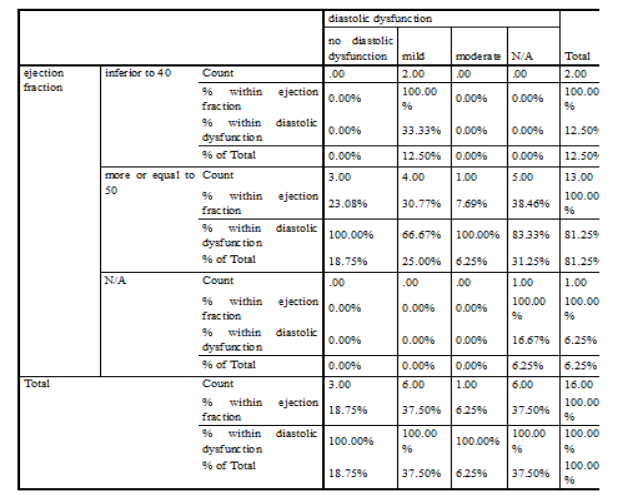
- 12.5% (2 patients) had an EF less than 40% (HFrEF), among them 100% were female, 100% had a mild diastolic dysfunction, 100% had valvulopathies, 100% had a LVH, 100% had an elevated PASP, 100% had no documentation for the pro-BNP level while half of them had a LVEDd more than 55mm and the other half had a LVEDd less than 55mm.
- 81.25% (13 patients) had an EF more or equal to 50% (HFpEF), among them 53.85% were male and 46.15% were female, 23.08% had no diastolic dysfunction, 38.46% had no documentation and the remaining had a diastolic heart dysfuntion; 46.15% had a valvular disorder while 53.85% had none; 69.23% had elevated PASP, 7.69% had normal pressures while the remaining had no documentation; 61.54% had no LVH and 38.46% had a LVH; 30.77% had a LVEDd more than 55mm while the remaining had a diameter less than 55mm; 7.69% had a positive pro-BNP level while the remaining had no documentation





Although HF is caused by a myocardial dysfunction, but it may occur in the presence of near-normal cardiac function. To maintain this function, our heart may use different compensatory mechanisms (increasing in HR, blood volume, filling pressures,…) leading sometimes to a progressive decline in its ability to either contract or relax.
Epidemiologic studies indicate that HF occur with either a reduced (≤40%) or preserved (≥50%) EF and up to 50% of patients with heart failure have a preserved ejection fraction, knowing that this proportion has increased over time [26]. Clinical trials have showed that outcomes are better in HFpEF group and death of non cardiovascular causes are more
common in this group of patients who have heart failure with a preserved ejection fraction[27-29].
Concerning the main causes of HF, hypertension and CAD were on top of the list by 1970 but different statistical analysis have showed that diabetes and CAD (mainly MI) have become responsible for this issue due to improvement in management and early detection of hypertension and valvular disorders[6,31-34].
Conditions commonly associated with HFpEF and HFrEF include older age, hypertension, coronary disease, and diabetes mellitus. Some of these factors (age, hypertension, obesity, female gender, atrial fibrillation, increased urinary albumin excretion, and increased cystatin-C ) favour HFpEF for HFrEF which main etiologic factors are male sex, smoking, hs-TnT, and prior MI. The predictors of these two types of HF were evaluated in the PREVEND community-based, cohort study of middle-aged subjects[30].
In one review, the prevalence of HFpEF increased proportionally with age. It was 15 per cent for patients aged less than 50, 33 per cent for those aged between 30 and 50 and 50 per cent for those aged above 70. Add that systolic dysfunction contributed a little bit in the heart malfunction in few of these patients especially the elderly[35,36].
So studies have confirmed that aging may lead independently to a HFpEF. For instance, both the Baltimore Longitudinal Study on Aging and the Framingham Heart Study showed that age plays a major role in diastolic heart failure. Comorbid conditions may occur also with age such hypertension complicating our aim to clearly understand the etiology of HFpEF [37-39]. Our registry disclosed that the mean age of our patients (either with preserved or reduced EF) is 67.44 years with a standard deviation of 15.943 divided as follow: 71.33 years (with a SD of 11.0711) for patients with EF less than 40% and 67.02 years (with a SD of 16.263) for patients with EF more or equal to 50%.
Same studies confirmed the fact that blood pressure elevation above or equal to 160/100, after age of 40 especially, double the lifetime risk of development of HF in these subjects.
In a Mendelian randomization study, a relation of causality between high BMI and HF was made focusing on younger population (hazard ratio, 1.19 per BMI-unit increase, 95% CI 1.03-1.39) [40], so this entity of obesity related HFpEF has been growing over years especially in people with metabolic disorder making promises in the development of new regimen that may reduce both morbidity and mortality of this entity of HF(mineralocorticoid receptor antagonists, neprilysin inhibitor, SGLT2 inhibitor).
Different other studies indicated that women are more likely to be affected with HFpEF than men[41] as confirmed in our registry. This finding was based on different facts (greater aortic stiffness and arterial pulsatility in older postmenopausal women than men, higher indexed LV wall thicknesses[42], higher elastin deposition and lesser collagen production in arteries due to estrogen impregnation in premenopausal women[43], greater general adiposity and circulating inflammatory cells)[44]. These numerous risk factors explain the greater risk of development of HFpEF in women than in men so specific sex-based therapy for HF should be issued in order to reduce both morbidity and mortality of this HF entity[45]. In our registry, for the group of patients with HFrEF, 71.6% were male while 28.4% were female and for the patients who suffered from HFpEF, 48.04% were male while 51.96% were female.
On another hand , HFrEF may occur after a massive MI or multivessel disease(first described by Killip in the 1960s)[47] due to the impairment of myocytes to contract properly. This condition may be reversed if restoration of blood flow is made as soon as possible [46]. This latter form of HF has shown to be reduced after the introduction of primary PCI as suggested by the HORIZONS-AMI cohort of 3602 patients recruited between 2005-2007 treated with PPCI (8% of patients developed HF as Killip II-IV upon presentation, reduced to 4.6% at day 30 then rising to 5.1% at 2 years) [48].
Different diagnostic laboratory tools and imagery may aid in the diagnosis of HF as mentioned above. One of the most useful laboratory hormone level in HF are BNP and NT-proBNP useful in distinguishing HF from other causes of dyspnea.
Measurement of plasma BNP or NT-proBNP is recommended by the 2013 American College of Cardiology/American Heart Association guidelines as well as the 2010 Heart Failure Society of America, 2012 European Society of Cardiology, and 2012 Canadian Cardiovascular Society guidelines [49-52] when the diagnosis of HF is uncertain.
Although NT-proBNP level is fourfold higher than BNP in patients with LV dysfunction, their level are similar in normal subjects[53]. Most symptomatic HF patients have a BNP level above 400 pg/mL while values less than 100 pg/mL have higher negative predictive value for HF[54]. Our pro-BNP level shows the following values for non-heart failure population:
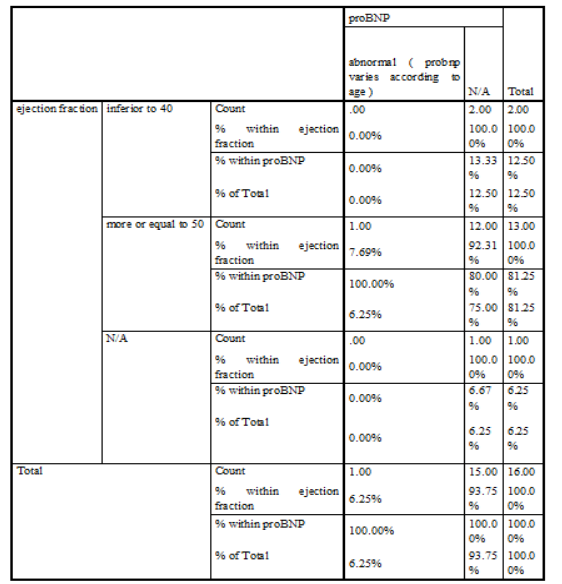
According to our statistics, the pro-BNP level was performed on 129 patients with 23 patients presented a normal level (21 patients with EF>or equal to 50%, 1 patient with EF between 40 and 50 and 1 patient with an undefined EF) and 106 patients presented an abnormal level according to our reference range (21 patients with EF<40, 76 patients with EF>or equal to 50, 8 patients with an EF between 40 and 50 and 1 patient with an undefined EF). So, none of our patients showed a normal level of pro-BNP with an EF less than 40% and its level was fourfold in HFpEF than in HFrEF(76 vs 21 patients).
In contrast, the NT-pro-BNP level required to diagnose HF varies with patient’s age and concentrations less than 300 pg/mL have high negative predictive value of 98% to exclude HF as cause of dyspnea. For instance, a normal level of NT-proBNP, based on Cleveland Clinic’s Reference Range is less than 125 pg/mL for patients aged 0-74 years and less than 450 pg/mL for patients aged 75-99 years. In case of heart failure, NT-proBNP levels that mean an unstable heart function are higher than 450 pg/mL for patients under age 50 and higher than 900 pg.mL for patients age 50 and older[55-57].
Since heart failure diagnosis is based mostly on the clinical presentation of the patient, TTE is performed to suggest possible etiologic factors of this condition (valvulopathies, systolic vs diastolic heart dysfunction…). Some of these findings studied in our registry include LVEDV, LVEF, presence of LVH, presence of diastolic dysfunction, documentation of any valvular disorder, measurements of PASP.
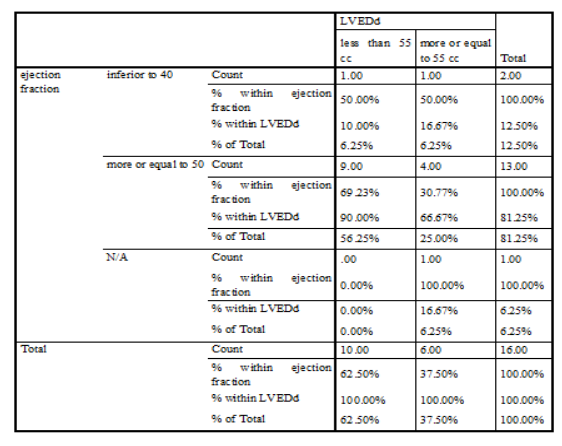
Since diastolic dysfunction results from impaired ventricular relaxation and filling patterns leading to a higher end-diastolic pressure for a given end-diastolic volume, LVEDd and LVEDV should be evaluated using ultrasonography for further investigation of the HF. Usually, its normal value is between 36 and 55mm at end diastole and between 23 and 40 at end systole in healthy subjects. Our numbers showed that 445 patients have a LVEDd more or equal to 55mm divided as following: 55 of them have an EF<40%, 344 with an EF>or equal to 50%, 36 with an EF between 40 and 50%, 10 patients with an undetermined EF.
Moreover, one of the most important and valuable variable measured while performing an echocardiography is the EF which plays a pivotal role in the diagnosis, risk stratification and therapeutic guidance of any suspected cardiac disease especially in term of HF. Although some clinical trials used to define HFpEF with an EF ranging between 40 and 55% but current guidelines recommend a cut value of 50% and an ejection fraction between 40 and 49% would be considered as gray area, while a “recovered hear failure with reduced ejection fraction” is the term given for HF in patients who had an EF less than 40% but recovered under medical therapy. As indicated by epidemiologic studies and HF registries, half of patients have a preserved ejection fraction and this proportion has increased over time [18,19]. Back to our numbers and for the 7 months period during which our study was conducted, we realize that 5.7% of our patients have an EF less than 40%, 89.49% have an EF more than 50%, 3.45% have an EF ranging between 40 and 50%, 1.27% of patients had no cut value for the EF. So, HFpEF is an emerging condition in our Lebanese society, as in other societies, that has been evolving over time.
Another commonly assessed echocardiographic feature is the presence of a left ventricular hypertrophy which may be caused by severe uncontrolled hypertension, aortic stenosis, hypertrophic cardiomyopathy or less commonly ventricular septal defects. Although EKG is a useful and cost-effective tool in detecting LVH, its moderate sensitivity or specificity due to different diagnostic sets, points toward the TTE or cardiac MRI for further confirmation[58-59].
LVH is defined as an increase in the mass of the LV obtained by 2D-echocardiography and is defined by the following criteria issued by the the American Society of Echocardiography, with the European Association of Echocardiography:
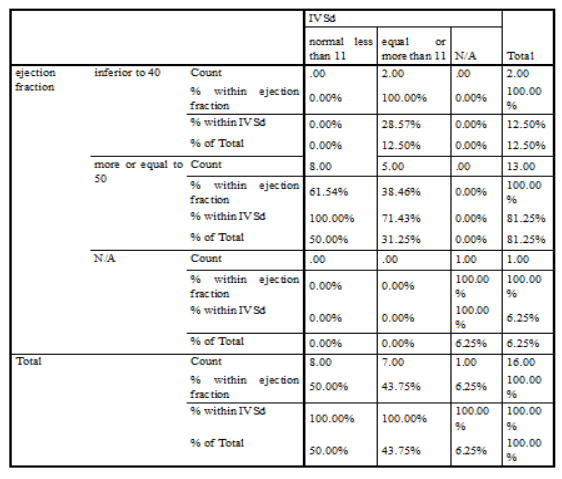
In our study, LVH is defined as IVS at the very end of diastole more or equal to 11 mm.
Patients with LVH may suffer from different cardiovascular complications such as heart failure and arrhythmia as shown by the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) study, where ST-T changes ("strain") on the baseline ECG in concert with voltage criteria for LVH increased the five-year risk of HF by more than threefold and the risk of HF-related mortality by fourfold, add that all-cause mortality were increased due to LVH in the middle aged population as shown by a large prospective study “ARIC”. Further studies confirmed the major role of echocardiography in detecting the risk for either atrial or ventricular arrhythmias caused by the LVH[61-64]. Our statistics showed that for the group of patients with EF less than 40%, 33.33 % had a LVH, 54.32% had no hypertrophy and 12.35% had no measurement; while for the group of patients with EF equal or more to 50%, 48.12 % had a LVH, 46.94% had no hypertrophy and 4.95% had no measurement.
Left ventricular diastolic dysfunction is one of the major features analyzed in our study. It should be suspected in any patient with symptoms suggestive of heart failure or even asymptomatic patients previously diagnosed with hypertension in whom screening with echocardiography may help us predicting complications or even death due to HFpEF. Thus, assessment of diastolic dysfunction should be considered an important step while evaluating a patient with suspicion of heart failure.
Patients with LVEF <50 percent, either symptomatic or not, may have diastolic dysfunction due to impaired LV relaxation while patients with LVEF >50 can have normal or abnormal diastolic function. For echocardiographic features that help us in diagnosing diastolic dysfunction, we consider the following criteria described in the 2016 American Society of Echocardiography and European Association of Cardiovascular Imaging guidelines:
The following rules are applied to determine if diastolic dysfunction is present:
-If <50 percent of measurable parameters for a patient meet the criteria above, then diastolic function is deemed normal.
-If >50 percent of measurable parameters meet the criteria above, then diastolic dysfunction is deemed present.
-If 50 percent of measurable parameters meet the criteria above, then the diagnosis of diastolic dysfunction is indeterminate [65].
In our study, we divided the diastolic dysfunction into three different categories:
We found that for patients with an EF less than 40%, 17.28% had no diastolic dysfunction, while 65.43% had it, 2.47% with uncategorized diastolic dysfunction and data not fully clear for 14.81% of this population. While for patients with an EF more than 50%, one quarter of them showed no diastolic dysfunction and more than the half had one (the majority as grade I).
Moreover, registries have made valve disorders an important cause of heart failure either with preserved or reduced ejection fraction. For instance, the Euro Heart Survey showed that 69.8 % of patients with significant VHD (most commonly aortic stenosis and mitral regurgitation) presented with HF symptoms and 19.3 % of people with severe AS undergoing surgical aortic valve replacement (SAVR) had LVEF <50 % [66]. Further data from the German aortic valve registry indicated that 26.6% of patients presented for SAVR had an EF less than 50% [68] while the American Transcatheter Valve Therapy (TVT) registry showed a prevalence of 25.6% of patients with LVEF less than 45% among those who underwent a TAVR [69]. Last but not least, a survey involving huge number of patients with suspected HF 14% of patients suspected with HF and referred to echocardiography for confirmation showed moderate to severe coexistent valvular heart disease [67].
In one study involving 70,043 patients with suspected HF referred for echocardiography, MR of any severity was found in 12.5 % and moderate or severe MR in 3.1 % of patients [67]. In comparison to our numbers, we found that among patients with an EF less than 40%, 71.6% of them had a documented valvular disorder and the remaining ones had none. Add that half of our patients with an EF more or equal to 50% showed a valvulopathy regardless its severity, while the other half were valve disorders free.
The last measured parameter in our study is the pulmonary artery systolic pressure (PASP). Its estimation is done by applying the following equation (based on the simplified Bernoulli equation): PASP ≈ RVSP = 4(peak TRV2) + RAP (estimated at 5-10mmHg).
When the TR signal is not reliably interpretable, echocardiography should be investigated for other parameters that may be responsible for pulmonary hypertension (right heart cavity sizes, non-TR-dependent estimators of PAP..).
Pulmonary hypertension (PH) is defined as an elevated mean arterial pressure ≥25 mmHg at rest and it is divided into 5 different categories by the World Health Organization (WHO) according to its etiology:
Identification of patients with PH-LHD is highly recommended because it is associated with a high rate of morbidity and mortality; patients may have either a HFrEF or HFpEF.
Most of series have indicated that 70 percent of PH is caused by LHD based on TTE [72]. PH-LHD is defined hemodynamically as an mPAP ≥25 mmHg and a pulmonary capillary wedge pressure (PCWP) ≥15 mmHg [73].
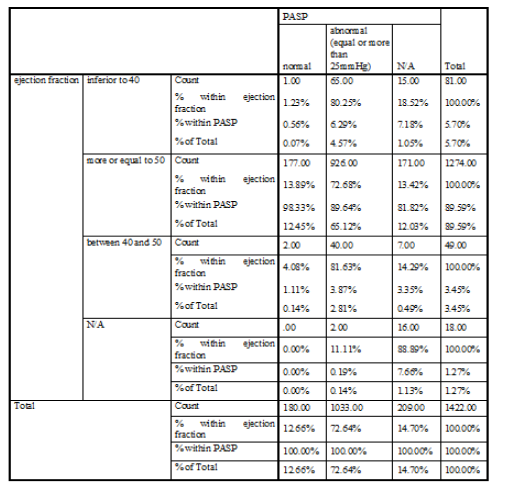
In some conditions, PH-LHD is confused with PAH that’s why investigating other factors (age, hypertensive, obesity,..) and TTE features of diastolic dysfunction favor HFpEF over PAH. Our numbers revealed that 80.25% of patients with EF less than 40% have an abnormal PASP (more or equal to 25mmHg) while only 1.23% have normal PASP. For patients with EF more or equal to 50%, 72.68% of them have an abnormal PASP and 13.89% have a normal pulmonary pressures.
LIMITATION AND PERSPECTIVE
The main limitation is that our study was conducted in only one medical center in Lebanon (LGH-UMC), which renders the generalization of the results to the Lebanese population rather difficult. But this makes the results more reliable in terms of echocardiography measurements as it is operator dependent.
Furthermore, patients information were taken from the EMF from the hospital and from the patient himself (before referring him to TTE) which reduces the likelihood of the results being biased.
Moreover, the cardiac sonography was performed by using the same machine by all the cardiologists and expert opinion was taken once in doubt which lead to a homogenous medical and imaging outcom
In this study, the prevalence of HF and its possible etiologies have been reviewed. As showed by numbers, aging play a major role in development of HF especially after the age of 65 years. The availability of cardiac sonography which is considered the most important tool in diagnosing HF, makes it easier to detect any possible disturbance that may lead to deterioration of the heart function, helping us in fighting either development or progression of a pre-existant HF and detecting its possible causes.
Add that, HFpEF should be deeply investigated while evaluating a patient with suspicion of HF because as our number showed its prevalence has been increasing over time in our community and in the international one.
All of this leads to a deduction in the overall cost by minimizing the rate of hospitalization and drug abuse while confirmation of HF is done using TTE which is available in almost all Lebanese hospitals.
We would like to thank everyone who made this work possible and paved the road for us.
Therefore we would like to thank very much the medical director who has reviewed this project.
Last but not least, we would like to thank the staff of the LGH for their constant help.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
