
Editorial | DOI: https://doi.org/10.31579/2578-8868/116
1* Medical and Surgical Investigation Hospital, Havana 10400, Cuba.
*Corresponding Author: Raúl Roberto Valdés Sedeño, Medical and Surgical Investigation Hospital, Havana 10400, Cuba.
Citation: Valdés Sedeño. RR., (2020) The investigation of Intraoperative Neurophysiological Monitoring and its relevance to Neuroethics. J.Neuroscience and Neurological Surgery. 6(3); DOI:10.31579/2578-8868/116
Copyright: © 2020 Raúl Roberto Valdés Sedeño, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 February 2020 | Accepted: 01 March 2020 | Published: 09 March 2020
Keywords: neuroethics; intraoperative neurophysiological monitoring; ethical investigation.
Intraoperative Neurophysiological Monitoring evaluates nervous system responses during surgery and classifies data as normal or abnormal. However it has been difficult to standardize Intraoperative Neurophysiological Monitoring results and to link intraoperative data to post-surgical outcomes, with alert criteria and concepts that contrast through laboratories and guidelines. Clinical Randomized Trials have not been applied for investigation because of ethical issues, but still more investigation is needed. Neuroethics and Intraoperative Neurophysiological Monitoring are related because the latter encompass patient’s post-surgical outcome and life quality. In this paper investigation methods proposed for Intraoperative Neurophysiological Monitoring are reviewed with consequent opinions. Moreover a quasi-experimental design for investigation is proposed, which is closer to Neuroethics and patients wellbeing.

Intraoperative Neurophysiological Monitoring (IONM) applies several Neurophysiological techniques during surgical intervention, evaluating nervous system results as normal or abnormal [1-3]. It has been stated that without application of IONM, neurosurgeons must rely in signals like respiratory rate, heart rate and blood pressure, which can bring late alerts concerning nervous system state during surgical intervention [4].
Generally, neurophysiological techniques implicated inside surgical room are Electroencephalogram (EEG), Evoked Potentials (EP) and Electromyography (EMG). Sensory evoked potentials like Brain Stem Auditory Evoked Potentials (BAEPS), Visual Evoked Potentials (VEP) and Somato-sensory Evoked Potentials (SEP) must be performed together with Motor Evoked Potentials (MEP) and other specific techniques for a multimodal neurophysiological approach [5, 6]
In the last 30 years IONM has become a regular technique for monitoring brain and spine around the world; moreover neck surgery is another important branch of monitoring [7]. In the United States IONM is highly used with guidelines for its application [8, 9]. In the last recent years Spain also reports high usage of IONM; this implies a process of rising sense of need [10]. Mexico is establishing guidelines for IONM implementation [11]. In Cuba its practice is increasing and highly demanded for spine and brain surgical interventions [12].
Benefits of performing Intraoperative Neurophysiological Monitoring surpass the risks.
In first place it must be understood that IONM is intended to protect nervous system during surgery [6]. Nevertheless this technique must be used with caution; one important aspect is that Neurosurgeons could try riskier surgical techniques trusting in Intraoperative Neurophysiological Monitoring protection [4]. Consequently there is one important thought: If bad Monitoring is going to be performed is better not to do it. Furthermore there are minor adverse reactions like: dental and lingual injuries when performing MEP. In addition seizures and arrhythmias can occur due to electrical stimulation [4].
Most investigations have shown the utility of IONM for detection of neurological damage during surgery [13-19] so without discussion the mere fact of having a technique notifying what is wrong inside someone´s body deserves attention and rank. But despite of positive data in worldwide investigations, predictive power of long term post-surgical clinical state of patients has been questioned [4].
Assuming this idea it can be understood that this modality is useful to detect eventualities inside operation room, but due to Nervous System complexity it can be observed restoration of functions and even normal nervous function in post-surgical phase despite IONM predicted during surgery it will be worst. Because of these enlightenments, discussion brings to light one simple answer: more investigation is needed.
Intraoperative Neurophysiological Monitoring must be refined.
International studies have reported that 76% of Neurosurgeons assumed IONM as an important tool for identifying risky surgical maneuvers; a minor group considers IONM as non-important [5]. Because of all this deliberation IONM software and hardware must be improved considering the important role it plays [20, 21].
Frist: refined methods like quantitative processing have been applied inside surgical room with good results [15-19], and still they are not being used in routine practice. In consequence the requirement for biomarkers of post-surgical evolution is still needed [12, 22]. Second: in order to achieve better results, good communication between Intraoperative Neurophysiological Monitoring staff is imperative [23]. Third: significant alarm criteria of evoked responses can change, so IONM personnel and investigators have to keep an open mind [24].
From Neuroethics to Neuroscience.
Neuroethics studies the implication of Neuroscience in human being knowledge, like ethics and legal problems [25]. Neuroethics is named by the beginning of 21 Century, referring to ethics, legal and social matters related to Neuroscience development [26]. Neuroethics has been classified as a success [27], so investigators must assume that Neuroscience´s findings must be understood and handle in an ethic way, this is where Neuroethics plays its bigger role [28].
Magnetic Resonance Imaging and Electroencephalogram have contributed to the development of Neuroscience and Neuroethics. Transcranial Magnetic stimulation is an example of cortical function manipulation [27]. So remember: it has been stated that a great science brings a great responsibility, as a result Neuroscience receives responsibility through Neuroethics [25].
Intraoperative Neurophysiological Monitoring is related to Neuroethics.
The way that human being analyzed the environment depends greatly of the scientist and technique information of the precise moment. What people believe depends greatly on historic information. The puzzle of human thinking is constantly adding or rejecting information depending of its utility.
As a result of this same process Neurosurgery is highly sued because of bad practice [4]. It has to be considered that Neurosurgery is a complex specialty that works very close to sensitive and specialized neural structures. So the presence of Neurophysiological and Imaging techniques which brings help during surgical interventions is very reasonable.
It was mentioned before in this paper, that Neuroethics tries to define the way that Neuroscientists uses their knowledge and its legal implications [25]. Neuroethics encompasses IONM because when the latter is applied the health staff is trying to achieve the best neurological status of patients. In a scientist way of thinking IONM could contribute to Neurophysiologists understanding of central and peripheral nervous system functioning during stress situations. In an ethic way of thinking it is almost innocuous to patients and it has been cited as a nervous system protector [4]. To put it briefly IONM is just another tool that in sum with imaging techniques contributes to give the best Multimodal attention to neurosurgical patients. Furthermore, there have been discussions about what kind of personnel should be accurate to perform IONM and which modality of monitoring should be correct [29].
Analyzing the fact that IONM alarms must be promptly recognized in order to protect patients during surgery, monitoring staff can come to the conclusion that guidelines and further investigation are needed worldwide [30]. In front of a technique still in development and with essential implications in human health, responsibility lies in scientist’s shoulders. Therefore from a Neuroethics point of view, investigational processes concerning IONM must go on.
Intraoperative Neurophysiological Monitoring should be seen from an Investigative point of view.
An investigative point of view for IONM is proposed in this paper, developing quantitative methods and searching for the right quantitative and qualitative technique to bring better clinical outcomes. The idea is to gather patients receiving different Multimodal Intraoperative Neurophysiological Monitoring methods, thus some patients would obtain some combination of IONM techniques and some would obtain others, but none will be excluded from it. This could lead to a change in guidelines, which are obviously in need for a transformation and to open IONM staff minds to new opportunities.
Intraoperative Neurophysiological Monitoring should be seen from a Clinical point of view.
A clinical point of view for IONM is proposed in this paper, this mean that the staff in charge of IONM must have solid knowledge in Anatomy, Physiology and Pharmacology [29]. Moreover only this way it will be possible to correlate changes in signals with Anatomy shifts and other events that can arise during a surgical intervention. Correct motivation and communication between Neurosurgeons, Anesthesiologists and Neurophysiologists depends on IONM staff knowledge, otherwise there is no room for good arguments between IONM staff and surgery managers. Moreover taking into consideration that Anesthesiologists and Neurosurgeons are in charge of deciding which action is required to reduce or to eradicate neurological damage during surgery [31].
Intraoperative Neurophysiological Monitoring can be elucidated statistically.
As a result of discussion, it has been indicated that Observational Cohort Studies and Randomized Controlled Trials would be the right option for Intraoperative Neurophysiological Monitoring investigation [32]. Moreover some investigators have stated to only support randomized trials [33]. Examining IONM performance, results of investigation have been difficult to standardize [32].
Several factors can influence in the dissimilar results of IONM investigations. Neurosurgeons responses can be really different in front of the same Neurophysiological alarm, to do something or nothing at all depends on doctor´s knowledge, studies, believing, stress or remaining surgical time [34-36]. It has been mention before in this paper the discussions about which IONM model is the right to apply, consequently this could influence strongly in investigations results as well [29].
Randomized Controlled Trials follows ethics principles which cannot be surpassed like: patients must be entirely satisfied with their participation and this should be achieved with total free will and inform consent. In no way patients can ignore any risks of investigation. Patients have the freedom of retiring of investigation without giving explanation. Doctors must be prepared to apply corrective measures if side effects or complications derived from investigation appear. When investigation is finished all patients must receive the right and more favored treatment [37].
Patients should identify the IONM surgery team and might have the opportunity to discuss the qualification of professionals in care of monitoring [30].
The application of Randomized Control Trials for IONM can be difficult considering these principles, is very unlikely that patients who know the risks of doing the surgery without monitoring will accept with total free will and inform consent to form a group without the best medical attention. Logically patients shall select the best and more complete option which will be surgery assessed with IONM, consequently a control group is difficult to gather. Moreover adding that wouldn’t be ethical for doctors doing so.
To this point it would be difficult to understand and accept Randomized Controlled Trials and leave patients unmonitored, even if the techniques in selected groups are long recognized as in need of improvement [32].
Observational Cohort Studies consist in observing two groups without a scientist intervention, one with the risk factor or treatment under observation and the other without it. Prospective Cohort studies though expensive can render good results because of its prospective character [37]. Observational Cohort Studies for IONM raises a few questions: if an Observational Cohort Study is intended and an Unmonitored group means: monitoring not ordered, monitoring never intended, monitoring not a part of the surgeon’s practice [32], it is obligatory to analyze these scenarios.
Assuming unmonitored groups like Monitoring not a part of the surgeon’s practice or Monitoring never intended it is perfectly understood that during the investigation the same surgeon or the same surgical group are not being investigated. Neurosurgeons generally follow IONM guidelines or have an idea of what monitoring should be done in front of different surgical scenarios and pathologies. Since important conclusions usually are done analyzing similar groups, these Observational Cohort Studies improbably would observe similar groups characteristics for monitored and unmonitored patients.
It is highly improbably that IONM would be applied randomly for similar tumor size, the same tumor localization in the central nervous system and similar surgical difficulty technique. So it is possible that important conclusions would not be achieved, since different tumors size, different tumor localization, different surgical techniques, different surgeons or even different surgical groups are being observed during this type of investigation. Nevertheless Observational Cohort Studies observes routine practice and acts like a branch of the same tree, identifying confounding factors perhaps like anesthetic and alert criteria variation [32]. Though incomplete this solution could be useful.
On the other way, it has been stated to apply Randomized Controls Trials to techniques like Motor Evoked Potentials which alarms have been in discussion [32, 38]. Further comments will be done ahead in this paper.
Multimodal, Quantitative and Clinical Intraoperative Neurophysiological Monitoring could be the solution.
In this paper it is indicated that the right solution for this very complicated neurophysiology modality is not to private patients from it, but to investigate several groups evaluated with different combination of techniques in order to validate IONM. Evaluating various techniques would allow knowing which combination is better for detecting neurological damage and consequent interventions. Principal idea is to find the right solution without causing any harm to patients if it is considered that animal investigations have found positive results for IONM[32]. Threshold alarm criteria of particular techniques could be another principle to gather patients in different groups.
Performing Multimodal Intraoperative Neurophysiological Monitoring techniques in each surgery should be the right approach. For example Dalvandi et al studied numerous techniques when monitoring posterior fossa tumors, and conclude that Motor Evoked Potentials was the more useful technique to predict nerve facial function [13].
The analysis of a representative group should lead to strong conclusions. Even if groups are evaluated with diverse Multimodal Intraoperative Neurophysiological Monitoring techniques, patients are still protected by the effects of Monitoring whether they are qualitative or quantitative techniques, furthermore if it is reckoned that Multimodal Intraoperative Neurophysiological Monitoring has been considered widely [6, 39-41]
Intraoperative Neurophysiological Monitoring can be linked to Neuro-ethical investigation.
Table 1 showsseveral examples the way IONM groups of patients can be organized for investigation.None of these groups are leaving without IONM and still an investigation is being done. These methods could prove which IONM technique is better or what combination of techniques is accurate.
Intraoperative evaluation of functional integrity of the Cortico-bulbar pathways, cranial motor nerves together with their nuclei and Brain Stem Reflexes.
Investigators have described a method for evaluating Blink Reflex in surgical room and under general anesthesia. This technique might allow evaluating the oligosynaptic reflex arc of Brain Stem as the stimulus travels through trigeminal afferents, brainstem connections between the trigeminal and facial nuclei, and the facial nerve. Same authors have informed a strong correlation between Blink Reflex and facial and/or trigeminal Cortico-Bulbar Motor Evoked Potentials in skull-base surgeries (posterior fossa), and have found it a predictor of clinical outcome [42].
This means there are other options to test functional integrity of Brain Stem (Pons) and Cortico-Bulbar tract, at least for facial and trigeminal nuclei which can be damaged during surgery of Cerebellar-Pontine angle Tumors for example. Blink Reflex is being used already inside surgical room [42]. Finally Masseter Reflex is another technique with stimulation and recording parameters described and under investigation, which can be of potential use. This reflex involves masseter and temporal muscles, together with masseter nerve that are part of trigeminal system [42]. Blink Reflex and Masseter Reflex include the evaluation of reflexes which are an important and vital function of the brain stem
Table 1 shows the way one can combine these techniques for functional evaluation of the integrity of the Cortico-bulbar pathways and cranial motor nerves together with their nuclei and Brain Stem Reflexes during surgery: one group would be evaluated only with Cortico-Bulbar Motor Evoked potentials of trigeminal and facial nerve and the other with a combination of Cortico-Bulbar motor evoked potentials of trigeminal and facial nerve + Blink Reflex + Masseter reflex techniques in order to identify if the latter combination render better results and consequently better postsurgical outcomes.
Intraoperative evaluation of functional integrity of the optic nerve:
There has been a lot of debate about the utility of Visual Evoked Potentials inside surgical room as a result of poor correlation between changes of potentials during surgical intervention and pot-surgical outcomes. Sasaki et al. used high-luminosity red LEDs and Electro-retinography to study this issue. Electro-retinography and particular characteristics of stimulator along with high-luminosity allow them to know whether changes in Visual Evoked Potentials inside surgical room were due to deviation of the light axis of the retina or due to surgical maneuvers. They obtained reliable evoked potentials during surgery and correlates their intraoperative findings with postoperative visual function [43].
Another technique has been described for evaluating visual system during surgery; stimulation of the optic nerve has shown to be useful in surgery of central skull base tumors. Authors have obtained cortical potentials applying electrical stimulation to the optic nerve; reproducible waves were recorded through surgery with amplitude changes relating to optic nerve or chiasm manipulation due to surgical maneuvers. Reversible amplitude changes were related to good post-surgical outcome [44]. Recently Visual Evoked Potentials has gained more visibility [45].
Table 1 shows the way one can combine these techniques for functional evaluation of the optic nerve during surgery: one group would be evaluated only with High Intensity Flash Visual Evoked Potentials + Electro-retinography and the other with a combination of High Intensity Flash Visual Evoked Potentials + Electro-retinography + Electrical stimulation of the optic nerve techniques in order to identify if the latter combination render better results and consequently better postsurgical outcomes.
Intraoperative evaluation of functional integrity of Brain Stem with Sensory techniques.
Somatosensory Evoked Potentials and Brain Stem Auditory Evoked Potentials are two techniques that can evaluate only 20% of the brain stem total area. These techniques have been reported as useful for documenting but not for preventing neurological injury to the somatosensory and auditory pathways [42]. Trigeminal somatosensory-evoked potentials have been applied during clinical studies and its application in patients under general anesthesia has been described. Although more investigation is needed is just another sensory technique that allows exploring functional integrity of a portion of the brain stem, altogether with SEP and BAEPs [42].
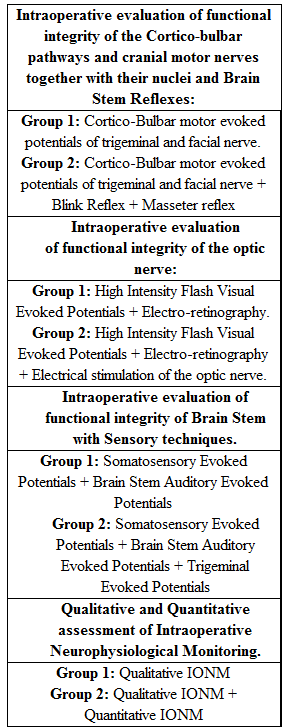
Qualitative and Quantitative assessment of Intraoperative Neurophysiological Monitoring.
Finally, Quantitative Intraoperative Neurophysiological Monitoring has shown positive results and the combination of this modality of monitoring with qualitative conventional methods as well as its implementation, could lead to a high level of IONM [15-19].
Table 1 shows the way one can combine these techniques for Qualitative and Quantitative assessment of Intraoperative Neurophysiological Monitoring and its improvement: one group would be evaluated only with: Qualitative IONM and the other with a combination Qualitative IONM + Quantitative IONM in order to identify if the latter combination render better results and consequently better postsurgical outcomes.
A Quasi-experimental design for IONM investigation.
As a result in this paper a quasi-experimental design investigation for IONM is proposed, including IONM techniques implemented in surgical routine practice associated with other novel techniques [46]. This could allow selecting the best combination of techniques rendering most useful results and higher effectiveness in monitoring. Furthermore this design has already been apply for IONM [13].
IONM is a developing branch of Neuroscience, which has shown to be useful. Nevertheless, investigation and refinement of techniques are still needed. Clinical Randomized Trials are difficult to apply considering their ethical consequences in this particular field. Observational Cohort Studies could lead to useful but incomplete conclusions. Therefore IONM investigation and Neuroethics are nearly connected. In this paper it is proposed a Quasi-experimental design investigation as a solution that could improve the utility of IONM and still protect patients during investigational processes.
Valdés Sedeño RR as the first author conceptualized the idea and writes the manuscript.
This research has not acquired funding from any source.
Conflicts of Interest
Corresponding author declares that there is no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
