
case report | DOI: https://doi.org/10.31579/2690-8816/070
Loma Linda University Health - Faamily Medicine Department.
*Corresponding Author: Ecler Jaqua, Loma Linda University Health - Family Medicine Department
Citation: Genovez M, Tran MN, Jaqua EE. (2022). May. The Importance of the Respiratory Physical Exam: A Case Report. J. Clinical Research Notes. 3(6); DOI: 10.31579/2690-8816/070
Copyright: © 2022 Ecler Jaqua, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 May 2022 | Accepted: 15 May 2022 | Published: 18 May 2022
Keywords: Case report; physical exam; pneumothorax; cornerstone; imaging
A 34-year-old male with a history of quadriplegia following a spinal cord injury presented to the clinic endorsing persistent dry cough and mild chest pain for the past three weeks. The patient appeared comfortable, in no acute distress, and with stable vital signs during the visit. His physical exam was unremarkableexcept for no air movement in the right lung. An urgent in-house chest X-ray showed a large pneumothorax with a small layering fluid component and near-complete right lung collapse. The physical exam has been the cornerstone of medical practice since its inception. This tradition has been passed down from physician educators to learners for centuries. Our case is unique because patients with severe pneumothorax usually exhibit urgent symptoms, such as respiratory distress and desaturations at presentation. However, our patient presented with only mild non-specific symptoms and did not have significant risk factors.Therefore, performing a thorough physical exam is essential to help uncover life-threatening pathologies even in patients with no severe symptoms.
Unfortunately, several recent studies show that the new generation of physicians underutilizes the physical exam.1 In addition, as technology advances and with the current COVID-19 pandemic, physicians are becoming less confident in performing a comprehensive physical exam and questioning the value and importance of what many physicians call "the cornerstone of medicine [1,2]. Furthermore, the increased dependence on images and laboratory testing, the time restriction for each patient encounter, and the growth of telehealth have encouraged physicians to skip the physical exam and rely only on the history and other diagnostic tools [1,2]. Through this case, our purpose is to demonstrate the importance of a physical exam in diagnosing deadly disorders in a patient with normal vital signs and mild, non-specific signs and symptoms. "This case report was prepared following the CARE Guidelines [3].
Timeline
| Table 1. Timeline | |||
Relevant Past Medical History and Interventions A 34-year-old male with a history of methamphetamine use, stab wound to the neck, spinal cord injury to C1-C7, intraventricular hemorrhage, and quadriplegia. | |||
| Date | Summaries from Initial and Follow-up Visits | Diagnostic Testing (Including dates) | Interventions |
| 1/27/2022 | The patient was complaining of a 3-week history of persistent dry cough. The patient inquired about getting an anti-tussive as his coughing was associated with chest pain in the last twoweeks. An examination revealed right-sided absent breath sounds. An urgent chest x-ray was ordered. | A chest x-ray showed a massive right-sidedpneumothorax.
| The patient was called and was asked to go to the ED immediately for further management of his right-sidedpneumothorax.
|
| 1/27/2022 | ED visit: The patient was evaluated by the ED physician. A chest x-ray confirmed the right-sidedpneumothorax | Chest x-ray re-demonstrated massive right-sidedpneumothorax | A pigtail chest tube was inserted in the second intercostal space. |
| 1/29/2022 | The patient's pigtail became dislodged. A repeat chest x-ray was ordered. | Chest x-ray showed interval resolution of his pneumothorax. | The patient was informed regarding interval resolution of his pneumothorax and was asked whether he wanted re-insertion of the pigtail chest tube, but the patient declined. |
| 1/30/2022 | The patient was discharged home and asked to follow up with his primary care physician. The patient'svitals were within normal limits. | ||
Case Narrative
A 34-year-old male with a history of subarachnoid hemorrhage, methamphetamine use, quadriplegia secondary to a thoracic spine injury from a stab wound, and consequently wheelchair-bounded presented to the family medicine residency clinic with a chief complaint of mild chest pain and persistent cough for the past three weeks. The patient described the cough as dry and constant and aggravating by prolonged talking. He also reported a choking feeling in his throat when talking excessively. His chest pain started one week ago and was intermittent, occurring several times a day, lasting fifteenminutes each time, usually after coughing. The pain was rated as 5/10, and he believed it was secondary to excessive cough.
During the visit, the patient was comfortable in no acute distress. His vital signs were within normal limits, and he had an oxygen saturation of 98%
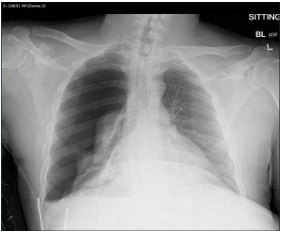
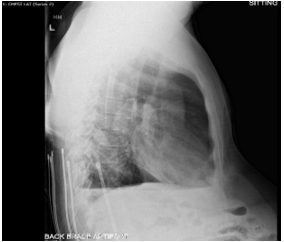
on room air. His physical exam was significant for no air movement in the right lung. The left lungwas clear to auscultation without wheezing or rales. There was no evidence of tracheal tugging or intercostal usage. An urgentchest x-ray was ordered in-house, and it showed a large pneumothorax with a small layering fluid component and near-complete right lung collapse (Figure 1). There was no evidence of a significant midline shift to suggest tension physiology (Figure 2). The results were communicated to the patient immediately, and he was sent to the nearest Emergency
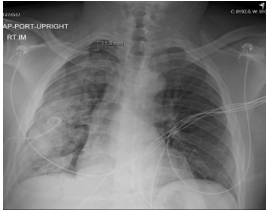
Department (ED) for further management. Pneumothorax was resolved via
a pigtail (Figure 3).
Pneumothorax occurs when the air between the lung and the chest cavity causes the lung to collapse. This is relatively common and can happen to patients at any age. A study by Bobbio et al. in 2015 estimated the prevalence of pneumothorax at 23,000 per 100,000 people in the US yearly.4 Pneumothorax management depends on symptoms, size, and degree of impairment to cardiac and respiratory system.5 Patient presentation can range from mild pleuritic chest pain to life-threatening medical emergency due to its potential to lead to respiratory failure and hypoxia.5 Furthermore, it could also lead to cardiovascular instability by increasing pulmonary arterial pressure [6].
Pneumothorax can be divided into primary spontaneous pneumothorax (PSP), secondary spontaneous pneumothorax (SSP), and traumatic pneumothorax. PSP mainly occurs in two age groups, before 20 years old without underlying lung pathologies and after 50 years old with underlying chronic lung disease.4 These occur predominantly in men with a women-to-men ratio of 1:3.30.4 The exact incidence is uncertain, but the yearly frequency has been reported to be 18-29/100,000 for males and 1.2-6/100,000 for females [5].
SSP usually occurs in patients with a history of underlying lung disease or current smokers older than 45 years.7 Many lung conditions predispose patients to SSP, with the chronic obstructive pulmonary disease being the most common.5 These lung conditions include obstructive airway disease (COPD, asthma), suppurative lung disease (bronchiectasis, cystic fibrosis), malignancy (lung cancer), interstitial lung disease (pulmonary fibrosis, sarcoidosis, lymphangioleiomyomatosis, histiocytosis X, extrinsic allergic alveolitis), infectious (pneumonia, tuberculosis) and other causes (adult respiratory distress syndrome, Marfan syndrome, Ehlers Danlos syndrome, catamenial, rheumatoid arthritis, connective tissue disease).5 Traumatic pneumothorax is caused by direct injury to the chest. These injuries can be accidental or iatrogenic. A penetrating chest injury or a rib fracture damaging the visceral pleura are common causes of unintentional injuries.5 There are many causes of iatrogenic injuries, including insertion of central vein line, pleural tap, transbronchial biopsy, fine needle aspiration, acupuncture, intravenous drug users, intubation barotrauma.5 These injuries can, in turn, lead to a tension pneumothorax where there is a mediastinal shift and cardiac collapse [5].
A chest X-ray (CXR) is part of the traditional imaging modality of choice, with computed tomography (CT) as the gold standard.8 CXR shows absent lung markings from visceral pleura to chest wall but can be misinterpreted due to artifact.5 CT scan is usually done to distinguish unclear cases, such as lung disease or large bulla.5 Both of these modalities require the patient to be moved and exposed to radiation. Because of these limitations, lung ultrasound is an emerging modality that could be more useful in the acute trauma setting at the bedside with point-of-care ultrasound.8 Lung ultrasound has reported better sensitivity for non-traumatic pneumothorax [9].
Pneumothorax treatment depends on the severity, size, and other underlying lung diseases.5 According to the guidelines from the British Thoracic Society, the pneumothorax size of small (<2>28%) to preserve oxygenation,but caution should be taken in the cases with COPD, who may retain carbon monoxide [5].
In the United States, traditional management of a PSP involves a large-bore chest drain to decompress the collapsed lung rapidly. Chest drain insertion is preferred over simple needle aspiration [5]. In a randomized trial, immediate success demonstrated by pneumothorax resolution occurred in 62% of patients with needle aspiration versus 68% having a chest drain inserted.10 Nevertheless, recent treatment includes more conservative practices such as smaller pigtail catheters or observation for a small SSP pneumothorax.8 These changes in practices would help decrease the length of stay, complications,and pain.8 There is still a 20% chance for recurrence despite these treatments, and patients should be warned to monitor for symptoms.5 With persistent cases or patients at high risk of recurrence, referral to thoracic surgery may be necessary for definitive treatment.5 Because these clinical practices vary, there are not many high-quality clinical trials to establish a consensus standard of treatment.
A patient with pneumothorax commonly presents as a young, tall, thin man with no predisposing factors with sudden onset shortness of breath and pleuritic pain. Physical exam findings include reduced breath sounds, reduced ipsilateral chest expansion, tracheal shift, tachycardia, tachypnea, and even hypotension.5 However, our patient was not in respiratory distress and maintained appropriate oxygen saturations despite having half of his respiratory system collapse. Utilizing the physical exam via lung auscultation was critical to uncoveringthe lack of airflow of his right lung. Our patient's lack of symptoms may have occurred due to his quadriplegic state, which did not allow for his body to be tested under high oxygen demand situations such as physical activity.
Consistent data shows that physical exam deficiencies lead to missed diagnosis and increased morbidity and mortality.1,11 For example, Verghese et al. demonstrated that of a cohort of 208 physicians, 63
Typically, pneumothorax is recognized easily if the classic signs and symptoms are present. However, this case illustrates the need for a thorough physical exam to uncover signs that are not readily evident upon a patient's initial presentation. In our case, to reach the correct diagnosis, a more detailed physical exam was needed. In addition, a chest X-ray would not have been ordered if a comprehensive physical exam were not performed, and a fatal diagnosis would have been missed. Therefore, don't overlook your physical exam; it can save lives.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
