
Review | DOI: https://doi.org/10.31579/2768-2757/180
Medical student, Faculty of Medicine, Omdurman Islamic University, Khartoum, Sudan.
*Corresponding Author: Abrar B. Elmalik., Medical student, Faculty of Medicine, Omdurman Islamic University, Khartoum, Sudan.
Citation: Abrar B. Elmalik, (2025), The Impact of Sleep Quality on Cardiovascular Health, Journal of Clinical Surgery and Research, 6(5); DOI:10.31579/2768-2757/197
Copyright: © 2025, Abrar B. Elmalik. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 July 2025 | Accepted: 25 July 2025 | Published: 31 July 2025
Keywords: cardiovascular health; sleep disorders; sleep cycle
This review investigates the influence of sleep quality on cardiovascular well-being, illuminating the consequences of insufficient sleep and recognizing the gaps in our understanding of its lasting effects. Typical sleep involves two primary phases: non-rapid eye movement (NREM) and rapid eye movement (REM). The majority of our sleep (75-80%) occurs in the NREM phase, with the remaining time allocated to REM. Suboptimal sleep quality has been associated with adverse psychological outcomes like anxiety, depression, aggression, altered cognitive function, and attention-deficit/hyperactivity disorder. The cardiovascular system plays a major role in regulating blood pressure and heart rate across distinct sleep stages. Blood pressure and heart rate rise during the early NREM stages, accompanied by reduced cerebellar blood flow. Connections have been established between sleep duration, coronary artery disease (CAD), and hypertension. Autonomic dysregulation during sleep might contribute to the onset of these conditions by disrupting sympathovagal balance. Additionally, various sleep disorders further impact cardiovascular health. Insomnia, prevalent among older individuals, correlates with an elevated risk of cardiovascular disease (CVD). Narcolepsy, restless legs syndrome (RLS), and obstructive sleep apnea (OSA) also associate with a high risk of cardiovascular complications. Despite identifying 84 different sleep disorders, our understanding of the prolonged effects of poor sleep on cardiovascular health remains incomplete. Comprehensive research is necessary to explore these associations and enhance our knowledge in this domain. Considering these findings, recommendations underscore the responsibilities of physicians and public health professionals in educating and raising awareness among patients about sound sleep hygiene. By imparting knowledge on the significance of sleep quality and its impact on cardiovascular health, healthcare providers can contribute to mitigating the overall burden of cardiovascular disease. Timely identification and management of sleep disorders also play a pivotal role in enhancing cardiovascular outcomes.
Sleep is a physiological state that is characterized by change in central nervous system in form of reversible loss of consciousness and changes in brain wave, change in respiration pattern, and other physiological functions. Sleep is considered to be occupying about one-third of humans’ lifespan and has main role in physical and mental wellness [1]. Previous Studies show that there is a negative impact due to poor quality sleep and sleep disorder on physical health such as type 2 diabetes, cardiovascular and neurological disease [1], chronic pain and higher levels of body mass index and other adverse consequences [2]. Also poor sleep quality has a negative psychological impact such as anxiety and depression, aggression, altered cognitive functioning, and attention deficit/hyperactivity disorder. [2]
Sleep Physiology
The sleep cycle is composed of two main stages : the nonrapid eye movement stage (NREM) and the rapid eye movement stage (REM). Both NREM and REM alternate with each other throughout sleep. Nonrapid eye movement stage divided into four stages that end up to REM sleep, so 75–80% of our sleep is in the NREM state and the remaining 20–25% is in the REM state [3]. The cardiovascular system plays an important role in regulating blood pressure and heart rate depending on the stage of the sleep cycle . There is increase in heart rate and blood pressure during the 1 st and 2 nd stages of NREM. In addition Cerebellar blood flow and metabolism are reduced during the NREM stage, on the other hand an increase in cerebellar blood flow is noticed with the limbic system and visual association. There is an association been established between sleep duration and the development of coronary artery disease (CAD) [3] and hypertension [4]. The pathophysiology for this can be related to autonomic dysregulation, which alters the sympathovagal balance during the sympathetic activity of sleep [3]. Nowadays, 84 different sleep disorders have been identified according to the International Classification of Sleep Disorder (ICSD-II) criteria [1]. Insomnia is a disorder that keeps people awake in night which lead to daytime drowsiness. About one in five old individuals was considered to have insomnia [5]. Insomnia patient may have 45% higher risk of CVD [6]. Narcolepsy is a disorder where the patient complains of excessive daytime sleepiness and has problem in regulating his sleep wake cycles. The estimated prevalence of narcolepsy in Europe was 47 patient per 100,000 persons and whereas the incidence was 0.64-1.37 per 100,000 [7]. They are susceptible for developing High blood pressure, Heart attack, Heart failure, Stroke [8][9]. Patient with restless legs syndrome (RLS) feel uncomfortable and unsettled especially at night because of periodic limb movement. The prevalence rises with aging and is estimated to be between 5% and 10%. RLS patient seem to be more susceptible for cardiovascular diseases [10]. Patient with obstructive sleep apnea (OSA) has trouble in breathing normally during sleep. The stop-and-start breathing may lead to decrease in oxygen saturation and disturbs sleep. About 34% and 17% of middle aged men and women, respectively, meet the diagnostic criteria for OSA. OSA has been linked to be more susceptible for High blood pressure, Stroke, Coronary artery disease, Heart failure [11]. This review explores the association between sleep quality and cardiovascular disease and the long term consequence of sleep disorders on cardiovascular health.
The main body:
*Sleep stages:
Sleep consists of two distinct phases—non-rapid eye movement (NREM) and rapid eye movement (REM) sleep. NREM sleep is categorized into three stages (Stages 1, 2, 3), gradually deepening with associated larger and slower brain wave activity. The classification of sleep stages is based on electroencephalography (brain wave activity), electro-oculography (eye movements), and electromyography (muscle tone). Upon entering sleep, the electroencephalogram (EEG) pattern transitions from low amplitude, high-frequency (>15 hertz [Hz] or cycles per second) wakefulness activity to Stage N1. Stage N1 represents a transitional phase between drowsiness and sleep, marked by a shift from EEG alpha waves (8–12 Hz) to relaxed wakefulness, low-voltage theta (4–8 Hz) or vertex sharp waves, and the absence of other sleep stage indicators. Typically, individuals spend only a few minutes in Stage N1 before progressing to Stage N2 sleep. Stage N2 is characterized by specific EEG waveforms, namely sleep spindles (12 and 14 Hz) and K complexes (large slow waves of <1>
*Nrem-Rem Cycle:
NREM sleep and REM sleep persist in alternating cycles throughout the night. Typically, REM sleep episodes lengthen as the night progresses. The duration of Stages 3 and 4 sleep decreases in the second cycle and may even vanish from subsequent cycles, with stage 2 sleep expanding to encompass the NREM phase of the cycle. The initial NREM-REM sleep cycle averages around 70 to 100 minutes, while the second and subsequent cycles have an average length of approximately 90 to 120 minutes. Over the course of the night, the average duration of the NREM-REM cycle ranges from approximately 90 to 110 minutes. [12]
*N1 Stage:
The initial phase of sleep in a typical young adult starts with stage 1 sleep, lasting usually for a brief period of 1 to 7 minutes at the onset of sleep. Stage 1 sleep can be easily disrupted, for instance, by softly calling a person's name, a light touch, quietly closing a door, and similar stimuli. Thus, stage 1 sleep is linked to a low arousal threshold. Besides its role in the transition from wakefulness to sleep, stage 1 sleep serves as a transitional stage throughout the night. An indication of severely disturbed sleep is often marked by an increase in the duration and proportion of stage 1 sleep. [13]
*N2 Stage:
Following this short episode of stage 1 sleep, stage 2 sleep, identifiable by sleep spindles or K-complexes in the EEG, ensues and persists for approximately 10 to 25 minutes. In stage 2 sleep, a more substantial stimulus is required to elicit arousal compared to stage 1 sleep. The same stimulus that led to arousal from stage 1 sleep often results in an evoked K-complex but does not prompt awakening in stage 2 sleep. [13]
*N3 Stage:
Stage 3 NREM sleep, characterized by high-voltage (at least 75 μV) slow-wave (2 cps) activity constituting more than 20% but less than 50% of the EEG activity, is the subsequent phase. Stage 3 sleep typically lasts only a few minutes in the initial cycle. [13]
*REM sleep
REM sleep typically constitutes around 20% to 25% of the sleep cycle, manifesting in four to six distinct episodes [13]. The identification of REM sleep involves observing saccadic eye movements during periods with low-voltage, mixed-frequency EEG and minimal submental EMG activity. Additionally, REM sleep can be recognized in epochs characterized by low-voltage, mixed-frequency EEG with sustained low submental EMG levels, even in the absence of eye movement. Transitional phases before and after clear REM sleep are considered, with smoothing rules applied to overlook minor shifts, based on the assumption that REM sleep represents a consistent central nervous system organizational state distinct from wakefulness and NREM. [14]
*Sleep Disorders:
1. Narcolepsy and Cataplexy:
Narcolepsy is characterized by an uncontrollable urge to sleep in inappropriate situations and locations, with sudden and brief attacks unless the patient remains undisturbed. Cataplexy involves a sudden loss of postural tone, causing the patient to collapse while consciousness is retained. Emotional triggers, such as laughter or crying, can induce cataplexy episodes.
The Narcolepsy/Cataplexy Tetrad:
Only 10% of patients exhibit the complete tetrad. It predominantly affects males, with a prevalence of 1 in 2000. Onset typically occurs in adolescence or early adulthood, and while the disorder is lifelong, its impact tends to diminish with age. Narcolepsy may have a familial link or be associated with factors like head injury, multiple sclerosis, or hypothalamic tumors. Pathological studies indicate early loss of hypothalamic neurons producing hypocretin/orexin, a neurotransmitter associated with wakefulness.
Diagnosis:
A suggestive history is complemented by EEG studies. The Multiple Sleep Latency Test (MSLT) is diagnostic, revealing the onset of REM within 15 minutes of sleep onset in 2 out of 4 short naps.
Treatment:
The non-amphetamine stimulant Modafinil, known for promoting wakefulness, effectively reduces daytime sleepiness. While amphetamines are more potent, they come with the risk of habituation. Sodium oxybate, a newer agent, enhances nighttime sleep and diminishes cataplexy. Selegiline, partially metabolized into amphetamine, exhibits a stimulant effect and may provide relief. Clomipramine and SSRIs (selective serotonin reuptake inhibitors) are also viable options. Occasionally, lifestyle modification through strategic "cat-napping" may prove sufficient. [15]
2. Obstructive Sleep Apnea:
Recurrent episodes of upper airway collapse and obstruction during sleep characterize obstructive sleep apnea (OSA), leading to arousals with or without oxygen desaturation. The collapse of the oropharynx at the back of the throat results in arousal, oxygen desaturation, or both, causing fragmented sleep. [16]
3. Sleepwalking and Night Terrors:
Manifesting primarily during the initial episode of slow-wave sleep but possible at any NREM sleep stage, sleepwalking and night terrors lack specificity in hypersynchronous delta activity, previously considered a somnambulism hallmark. Altered consciousness during these episodes is revealed through post-arousal EEG activity. The pathophysiology involves predisposing factors, genetically determined tendencies for deep sleep; facilitating factors deepening sleep and increasing slow-wave sleep; and triggering factors causing sleep fragmentation, such as stress, environmental stimuli, and stimulants. [17]
4. Sleep Paralysis:
An uncommon neurologic phenomenon, sleep paralysis is described as brief episodes of limb, speech, and eye movement inability upon awakening (hypnapompic or postdormital sleep paralysis), or more rarely, when falling asleep (hypnagogic or predormital sleep paralysis). The patient remains fully aware with complete recall, occasionally accompanied by vivid, terrifying hallucinations. Rarely preceded by cataplexy, the paralysis abruptly disappears, either spontaneously, after the patient's effort to break it, or following sensory stimulation, such as touch or speech. Episodes typically last a few seconds but may extend to a few minutes. (18)
*Cardiovascular Disease Risk Factors:
According to the World Health Organization, heart disease and stroke are primarily linked to behavioral risk factors such as poor diet, physical inactivity, tobacco use, and excessive alcohol consumption. Behavioral risk factors can manifest as increased blood pressure, elevated blood glucose, abnormal blood lipid levels, overweight, and obesity. These "intermediate risk factors" are indicators of a heightened risk for heart attack, stroke, heart failure, and other related consequences, often assessable in primary care settings. Scientific evidence supports the effectiveness of interventions such as reducing salt intake, increasing fruit and vegetable consumption, regular exercise, and abstaining from alcohol to lower the risk of cardiovascular disease.
1. Uncontrolled Blood Pressure and High Cholesterol:
Over the period between 1999–2000 and 2009–2010, there was a notable decrease in the prevalence of both uncontrolled high blood pressure and elevated levels of LDL cholesterol among U.S. adults. The decline was 7.6 percentage points for uncontrolled high blood pressure and 9.3 percentage points for uncontrolled high LDL-C. Despite this improvement, smoking prevalence did not significantly decrease during this 12-year span. In 2009–2010, among adults aged 20 and over, 25.1% were current smokers, 23.3% had uncontrolled high LDL-C, and 11.8% had uncontrolled high blood pressure. [19]
2. Diabetes Mellitus:
Numerous clinical trials have explored the effects of intensive hyperglycemia management on reducing cardiovascular risk in recent decades, yielding varied results in both Type 2 Diabetes (T2D) [20] and Type 1 Diabetes (T1D) [21].
3. Alcohol:
Research indicates that the association between binge drinking and cardiovascular death meets established criteria for causality. Future investigations into alcohol-related harm should not only consider the quantity consumed but also examine the drinking pattern [22].
4. Obesity:
The prevalence of obesity has seen a global increase in recent decades, irrespective of gender, age, or the developmental status of the country. In the general population, there is a consistent and robust correlation between obesity and, particularly, severe obesity (BMI≥35 kg/m2) with an elevated risk of incident Cardiovascular Disease (CVD) and CVD mortality [23].
* The Link Between Inadequate Sleep and Cardiovascular Disorders:
Insomnia, the most prevalent sleep disorder in the United States, shows a high comorbidity with various cardiovascular diseases (CVDs). Over the past decade, numerous observational studies have highlighted the association between insomnia and the incidence of cardiovascular disease (CVD) morbidity and mortality, encompassing hypertension (HTN), coronary heart disease (CHD), and heart failure (HF). Despite some variations in the literature arising from differences in defining and measuring insomnia, current data consistently suggest that insomnia, particularly when coupled with a short sleep duration, correlates with an elevated risk for HTN, CHD, recurrent acute coronary syndrome, and HF. Proposed mechanisms are likely linked to the dysregulation of the hypothalamic-pituitary axis, heightened sympathetic nervous system activity, and increased inflammation [24, 25, 26, 27, 28, 29, 30, 31].
*Sleep Apnea:
Sleep apnea, causing a significant surge in sympathetic activity during sleep, results in increased heart rate, blood pressure, and temporary disruption in venous return to the heart [32].
* Excessive Daytime Sleepiness:
Highly prevalent among adults in the United States, excessive daytime sleepiness is independently linked to an approximately two-and-a-half-fold increased risk of cardiovascular mortality in a sizable national sample.
Tips for Better Sleep:
To enhance your sleep quality, refrain from the following activities three to four hours before bedtime:
- Consuming caffeinated drinks like soda, tea, and coffee.
- Using tobacco.
- Consuming alcohol.
- Taking naps after 3 p.m.
- Eating chocolate.
- Having heavy meals [33] [34].
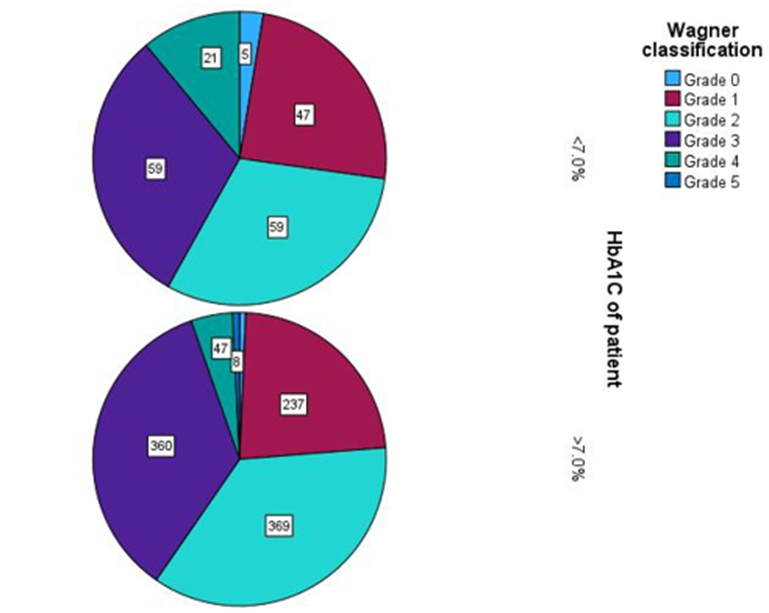
Figure 1: The relation between Wagner classification and Hba1c.
In review that discusses the majer effect of sleep on cardiovascular system, it is emphasis that sleep is a complicated sets of neurological processes that necessary to meet several physiological demands, and getting healthy & adequately sleep interval has been consider as an essential public health matter [35]. Cardiovascular diseases is one of majer life-threating diseases in developing world. However, the connection between sleep duration deficiency and cardiovascular diseases incidence might be due the influence of not enough or imperfect sleep periods on cardiovascular biological risk agents such as high serum cholesterol, elevation of blood pressure, presence of diabetes, & developing of excess weight relating diseases [36] [37]. On other side the relation between prolonged sleep period and cardiovascular diseases incidence may be demonstrate by prolonged sleep duration being the first manifestation of clinical symptoms prior the disease [36]. At overall, prolonged and shortened sleep duration were Independently related with high cardiovascular diseases and mortality rate [38]. But prolonged sleep period especially between those with bad sleep quality could be related with more higher mortality rate from cardiovascular diseases [39]. That means, sleep quality is a necessary part in the normal recovery of body during sleeping, so to prevent cardiovascular diseases it is important to get perfect sleep quality [40]. The most important strength point in this study it is showing that; the sleep quality can alter the relation between cardiovascular events and sleep duration [41]. Therefore, prolonged and shortened sleep periods may not be consider as cardiovascular health hazards for those with perfect sleep quality and vise versa for those with bad sleep quality [41]. So we recommend future workups should also focused on sleep quality as well as sleep duration for better approach of cardiovascular health.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
