
Research Article | DOI: https://doi.org/10.31579/2690-4861/204
1 Pediatric Allergy & Immunology, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
2 Pediatric Immunology & Allergy, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
*Corresponding Author: Emadia Alaki, Pediatric Allergy & Immunology, Research Centre of King Saud Medical City, Kingdom of Saudi Arabia.
Citation: E Alaki, A Donques, Abdulwahab A-Ayoubi, Ghannam A Ghannam, Abdul A Alsayegh. (2022). The Impact of Lockdown Restrictions on Family with Children of Asthma and Allergy during Covid-19 Pandemic, in KSMC, Riyadh, Saudi Arabia-A Retrospective Study. International Journal of Clinical Case Reports and Reviews. 10(5); DOI: 10.31579/2690-4861/204
Copyright: © 2022 Emadia Alaki, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 January 2022 | Accepted: 08 March 2022 | Published: 11 March 2022
Keywords: COVID-19; pandemic; asthma; allergy; lockdown
To describe the impact of the COVID-19 pandemic and lockdown on pediatric asthma housings and on disease burden in patients and their family.
To study the effect of minimizing outdoor allergen exposure that done by the effect of lockdown and the compliance to give the inhalers because of availability of the parents in decreasing the bronchial asthma attacks. To improve clinical practice post COVID-19, not default to the past.
According to the Saudi Initiative for Asthma, the prevalence asthma is not known among adults and the prevalence in Saudi children ranges from 8% to 25% based on studies conducted over the past three decades [1].
Asthma affects more than 2 million people and majority of them have uncontrolled asthma ranged from 45% up to 64% [2,3]. Asthma is a serious public health issue globally and nationally. The World Health Organization (WHO) Global Asthma Report that 334 million people worldwide. Approximately 14% of the world's children have asthma [4].
What are the implications for asthma management in children and for the asthma community as lockdowns are eased COVID-19 is generally a mild disease in children compared with adults [5], and although a few children get a severe respiratory or systemic disease, most do not need intensive care unit.
Given the dramatic drop in ED utilization during the pandemic period, the researchers suggest several areas for future investigation. Some study was reported a 76% drop in emergency visits for asthma during COVID-19 pandemic [6].
This decrease in emergency visits is need further analysis unlikely to be accounted for simply by parents managing mild attacks at home, and adherence [7].
However, analyzing the impact on asthma symptoms of person-to-person transmission of conventional respiratory viruses, such as rhinovirus and respiratory syncytial virus, and reduced exposure to outdoor seasonal vs. indoor allergens, and traffic and industrial pollution [8], a well-established factor in asthma attacks [9].
The social challenge is that these huge reductions in asthma attacks have been achieved not with expensive new drugs but by behavioral changes. Can we maintain this post COVID-19 pandemic [10]. At the very least, we need to challenge ourselves about being more rigorous in preventing transmission of respiratory viruses Before the COVID-19 pandemic and lockdowns around the world.
We planned in this study to understand the effect of lockdown on the health of patients with Allergic diseases and determine the challenges faced by them what are after COVID19? Concurrent, the COVID-19 pandemic introduced a need to change clinical practice, Concurrent, the COVID-19 pandemic introduced a need to change clinical practice, such as virtual clinic, Telemedicine and alternative delivery of aerosolizing procedures. A need for guidelines in the context has been expressed; however, this is challenged we are facing [11].
With these circumstances, pediatric asthma services around the world are being reorganized to face the new, uncertain, reality of this pandemic. Pediatric asthma experts from all around the world, aims to develop recommendations that will improve patient care [12].
To identify and share best practices, and in collaboration with the World Allergy Organization Pediatric Asthma Committee, we assessed the impact of COVID-2019 on pediatric asthma services and their patients through a survey addressed to large pediatric asthma clinics worldwide [4].
We recommended multinational real-life studies with detailed information on asthma phenotype and medication usage in patients with a confirmed diagnosis of COVID-19 and outcome in all aspects, medical, social, economic and psychological. The aim from study to looks after the effect of the COVID-19 lockdown on our pediatric asthmatic and allergic patients in 3 months period.
Retrospective cross sectional survey design statistical model, was conduct in King Saud Medical City on OPD clinic of allergy/ immunology. By direct contact with patient telephone number through our specialist, who having follow up with asthma and allergy clinic.
It included questions about the general clinical condition, medication delivery and adherence, triggering factors of pediatric asthma and family attitude during the COVID 19 pandemic. The survey questionnaire can be found in appendix.
Study population:
Pediatric patients (male from 0-12 years old and female up to 14) and their family.
Study period:
3 months from26/7/2020 to 25/10/2020 IRB approval 21/7/2020
Sample size:
All the patients who replayed to the OPD telephone call over the period of three months (103 Patients).
Data Collection and Analysis:
Data was collected through Questionnaires which guided by the Saudi Initiative for Asthma (SINA) 2020 And Asthma Control test, via direct telephone contact. The questionnaire is constructed with input from the allergist consultant and Epidemiologist. And the data will have analyzed through SPSS for windows software, Version 17.0 with confidence interval = 95% and P value= <0>
A total of 103 patients participates with their families during COVID 19 Pandemic. The Majority of them were Saudi nationality 97.1% (100) while male gender 61.2 % (63) the maximum age 14 years old and the minimum one year and ten months while the mean 7.75 with standard Deviation of 8.98 ± 3.94 years (table 1).
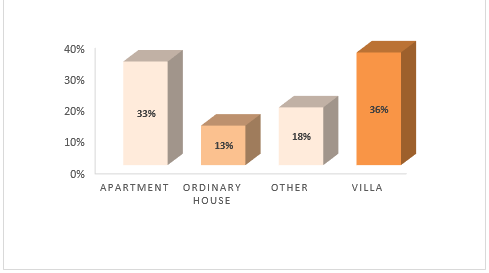
Most of the participants living in a villa 36.0% (37) (Table 1, Figure 1) The general information showed that more than half of the participants are non-smoker 58.3 % (60), most of the family members who have reported to have bronchial asthma are one member followed by two members 36.0% (37) 33.0% (34). In comparison, those who did not have bronchial asthma was reported 15.5% (16). (Table 1).
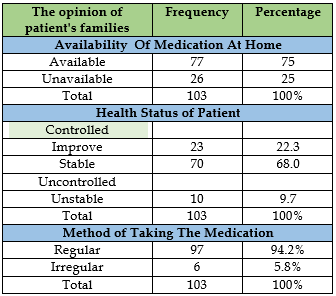
The majority of the participants, 78.8% (76), have enough medication available at home, and they are aware of how to use the treatment regularly way 94.2% (97). (Table 2, Figure 2).
Comparison of the responsibility for giving the medicine to the patient revealed that the mother was the most responsible person who is giving the medication to the patient before73.8% (76) and after 69.9% (72) Covid-19 Pandemic but she is less responsible after Pandemic (Table 3). On the other hand, the father was more responsible for giving the medicine to the patient after Pandemic 10.7 % (11) (Figure 3).
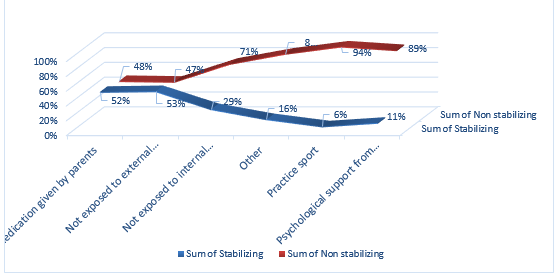
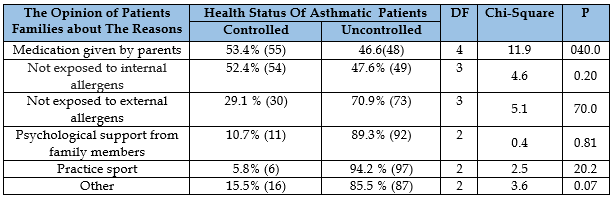
The most common opinion of patient families about the reasons for improving and stabilizing the disease during the pandemic was due to not being exposed to external allergens 53.4% (55), followed by medication given by parents 52.4% (54). (Figure 4).
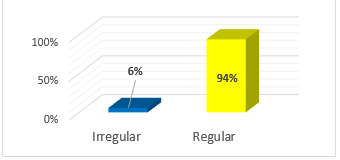
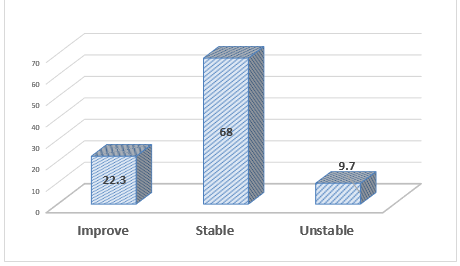
More than two third of the opinion of patient’s families, were improved 22.3 % (23) and stable 68.0% (70), during the covid-19 pandemic in general, while the majority of them taking medicine in regular way 94.2% (97). (Figure 5).
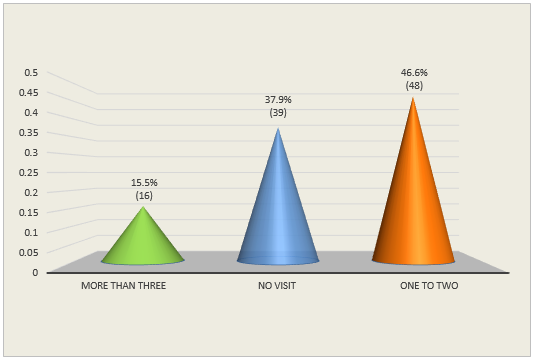
The Majority of the patients visited the Emergency one to two times, 46.6% (48). However, 37.9% (39) did not visit it in the last three months before Covid-19 Pandemic. (Figure 6).
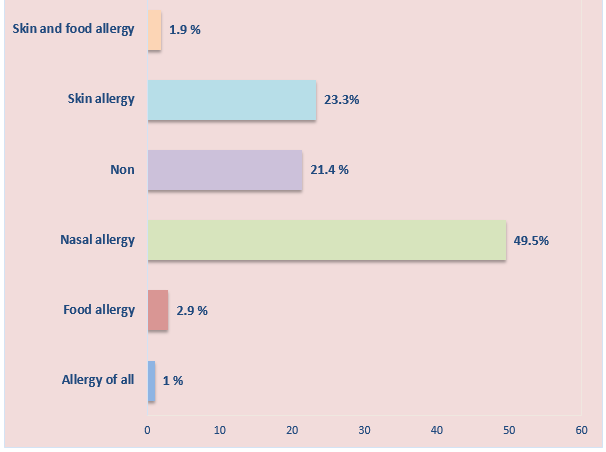
The most common type of allergies in our patients of bronchial asthma patients suffers from Nasal allergy 49.5 % (51) and Skin allergy 23.3 % (24). (Figure 7).
Table 3 shows significant statistical differences between the Age of patients with bronchial asthma (Chi-Square =38.3, DF = 3, P=0.003), with the Health Status of Asthmatic Patients during Covid-19 Pandemic. Weak and unreliable model, Alogistic regression model is required according to our bioststician when they do logistic regression way there was no much difference.
While there is relationship between the type of housing the patient lives in (Chi-Square =7.8, DF = 3, P=0.065), with the Health Status of Asthmatic Patients during Covid-19 Pandemic but is not statistically significant (Table 4).
There was a statistical relationship between the Medication given by parents (Chi-Square =11.9, DF = 4, P=0.004) with the controlled and stabilization of B.A during Covid-19 Pandemic (Table 5).




This questionnaire study provides important feedback about the impact of a lockdown on parents’ management of children’s asthma and disease outcomes. Eventually parental feedback was generally positive regarding asthma controlled and they related to not exposed to outdoor allergen and assistance of telemedicine for their interactions with health services to manage their children’s asthma.
Telemedicine thrives in all medical specialties during the COVID-19 epidemic all over the world. Standard tools where such as the Asthma Control Questionnaire were used, whereas objective measures, such as spirometry or peak expiratory flow rate, were less often feasible [13,14].
In spite there are challenges, there was no apparent deterioration in asthma in the large majority of patients. More than 90% stable and improved in our study and these the influence by increased adherence to treatment and regular used by both parent and more obvious father had more anticipation in his children management.
Furthermore, social distancing, sheltering at home, and reduced school days may reduce exposure to the main triggers of acute asthma events, most notably respiratory virus infections, outdoor allergens, physical exercise, and air pollution, contributing to sustained, or even improved, outcomes during this period [15,16].
Many recent reports have described evidence of significant mental strain, such as anxiety, fears and depression. These factors may affect asthma control both directly and indirectly [17.18].
Asthma management is a continuous cycle of assessment, treatment, and review by a trained person [19]. However, the coronavirus pandemic has disrupted this continuum of asthma care [20, 21]. Telemedicine can provide successful follow-up care for respiratory illnesses in children. [22].
The general information showed that more than half of our participants are nonsmoker 58.3 %, and majority of our patients were control. Protracted stay at home recommendations is associated with remarkable improved in patient with outdoor allergy.
In contrast of many studies show the influence of environmental factors that could worsen asthma control including prolonged exposure to indoor allergens, reduced physical activity, and exposure to second‐hand smoke.
As noted in the consensus statement of the Italian society of pediatric allergy on the management of pediatric allergic disease during COVID‐19, “an increased expression of ACE2, induced by smoking, means increased susceptibility to contract the COVID19 infection and potentially to develop a more severe form” [24].
However, living in substandard housing often leads to exposure to triggers and higher rates of allergen sensitization [25]. Features of substandard housing such as excessive moisture and dampness, inadequate or poorly maintained heating and ventilation systems, crowding, pest infestations, deteriorated carpeting, and structural defects are associated with exposure to indoor asthma triggers [26].
It is feasible to reduce indoor exposures and doing so improves clinical outcomes. Over the past 2 decades, knowledge of how to reduce exposure to indoor asthma triggers has increased dramatically [27].
About 49.5% of our patients suffer from allergic rhinitis. Many studies in Saudi Arabia reported older age groups, overweight and male present with severe and persistent forms of AR [28].
In adults, the prevalence of AR ranges from 10% to 30%, while in children it is approximately 40% [29].
We noted that majority of the patients visited the Emergency one to two times, 46.6%, and 37.9% did not visit in the last three months before Covid-19 Pandemic, and however we need further study to compare the ER visit through and after pandemic.
Telemedicine options were the best during the lockdown. Multiple studies reporting on the efficiency of telemedicine use as a tool for ongoing management of patients with chronic disease such as asthma [30],and diabetes mellitus [31].
The promising outcome from this pandemic that equivalence of patient health outcomes between in-person and remote care provision [32, 33].
Asthma control was better during lockdown and post curfew. Children with asthma need regular monitoring and adherence by parents to maintain good asthma management and control. Telemedicine can play an exciting role in the management of childhood asthma, however healthcare professionals should have adapted novel technology based management strategies to improve asthma care.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
