
Research Article | DOI: https://doi.org/10.31579/2690-4861/306
Department of Medicine and Geriatrics, Princess Margaret Hospital, Lai Chi Kok, Kowloon, Hong Kong, China.
*Corresponding Author: Chin Tong Kwok, Department of Medicine and Geriatrics, Princess Margaret Hospital, Lai Chi Kok, Kowloon, Hong Kong, China.
Citation: Chin T. Kwok, (2023), The Impact of Coronavirus Disease 2019 (COVID-19) on Lung Function, Exercise Capacity and Quality of Life in a Cohort of Survivors, International Journal of Clinical Case Reports and Reviews, 13(4); DOI: 10.31579/2690-4861/306
Copyright: © 2023, Chin Tong Kwok. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 April 2023 | Accepted: 17 April 2023 | Published: 25 April 2023
Keywords: COVID-19; lung function; 6-minute walk test; SF-36
Background: The lung function outcome among COVID-19 survivors in Hong Kong remained unknown.
Methods: Patients above the age of 18 years old with the principal diagnosis of COVID-19 who were discharged from a tertiary center in Hong Kong between the period of 1st February 2020 to 31st July 2020 were offered three lung function tests at approximately one, three and six months upon discharge for monitoring of their outcome. Six-minute walk test (6MWT) and health related quality of life assessment by Medical Outcomes Study 36-item Short Form General Health Survey (SF-36) were arranged on the same day of lung function test.
Results: Thirty patients had lung function test performed within 60 days after discharge. Nineteen and twelve patients had lung function test performed at 60-180 days and 180 days after discharge respectively. After corrected for underlying lung diseases, 32% patients have reduced hemoglobin adjusted DLCO and PImax, while 88% patients have reduced PEmax. For patients with serial lung function performed, adjusted DLCO and PImax improved with time. The exercise capacity of COVID-19 survivors was significantly lower than normal subjects in most age groups. COVID-19 survivors have lower quality of life in the context of physical functioning, social functioning and role limitation due to physical problems, compared with normal subjects.
Conclusion: COVID-19 leads to lung function abnormalities including reduced diffusing capacity of carbon monoxide, maximal inspiratory pressure and maximal expiratory pressure in more than 40% of patients, which improved with time. Exercise capacity and health status of COVID-19 survivors are lower than normal subjects.
COVID-19 is a novel viral infection that was characterized as a pandemic by the World Health Organization since March 2020. There were multiple waves of outbreak in Hong Kong. Among local survivors, the outcome remained unknown. This study aims to analyze the lung function, exercise capacity and quality of life of the first cohort of survivors.
Similar study was done in Hong Kong for Severe Acute Respiratory Syndrome which led to the outbreak in 2003. Significant impairment in diffusing capacity of lung for carbon monoxide (DLCO) was noted in SARS survivors at 6 months and 12 months after illness onset. Exercise capacity and health status of SARS survivors were remarkably lower than those of a normal population [1,2].
The first case of COVID-19 was reported in Hong Kong in late January 2020. Hospital Authority Infectious Disease Centre (HKIDC) received all local COVID-19 cases at the beginning of the outbreak. Due to the increasing number of cases, COVID-19 patients were later taken care in hospitals at different clusters. In the first 6 months of the outbreak from 1st February 2020 to 31st July 2020, adult patients discharged from the HKIDC were offered three lung function tests at approximately one, three and six months upon discharge for monitoring of their outcome. Six-minute walk test (6MWT) and health related quality of life assessment by Medical Outcomes Study 36-item Short Form General Health Survey (SF-36) were arranged on the same day of lung function test.
This study will provide information for counselling COVID-19 patients on the long-term consequences and insight on follow up plan for COVID-19 survivors.
COVID-19 leads to lung function abnormalities, reduced exercise capacity and impaired quality of life in survivors.
4.1 Subjects
This is a retrospective study involving COVID-19 patients who were discharged from Princess Margaret Hospital in Hong Kong in the first six months of the outbreak. Patients above the age of 18 years old with the principal diagnosis of COVID-19 who were discharged from the Princess Margaret Hospital HKIDC between the period of 1st February 2020 to 31st July 2020 and had follow-up lung function test at 1-2(early), 3-6(mid) and >6(late) months after discharge were included in the study. A list of patients will be generated from the clinical data analysis and reporting system (CDARS) using the searching criteria of COVID-19 and lung function test. Patient records will be reviewed retrospectively for data collection. Patients who refused lung function tests will be excluded.
4.2 Study design
The early, mid and late lung function test parameters including spirometry (Forced Expiratory Volume in one second FEV1, Forced Vital Capacity FVC, FEV1/FVC ratio and peak expiratory flow PEF), lung volumes (Total Lung Capacity TLC), DLCO, maximal inspiratory pressure (PImax) and maximal expiratory pressure (PEmax) were recorded using CareFusion Vmax system. Normal lung function parameters are defined as 80
CDARS search yielded 323 patients discharged in the period of February 2020 to July 2020 for COVID-19. Among them, 47 patients had lung function test performed after discharge. There are 30 patients with first lung function test performed within 60 days after discharge. Among the 30 patients, 19 of them had second lung function test performed at 60-180 days after discharge. Among the 19 patients, 12 of them had third lung function test performed 180 days after discharge.

Among the 30 patients with first lung function test, the age ranged from 21 to 80 years old (mean 53 years old). There are 16 males and 14 females. There are 25 patients with good past health. The remaining 5 patients had scoliosis, bronchiectasis, chronic obstructive lung disease, history of tuberculosis and lung cancer respectively. The first lung function test was performed on day 21 to day 59 after discharge (mean day 37).
The first PFT results of all patients and patients with good past health were summarized in table 1 and table 2. All lung function parameters are abnormal, especially PEmax, hemoglobin adjusted DLCO, PImax and PEF. After corrected for underlying lung diseases, 32% patients have reduced hemoglobin adjusted DLCO and PImax, while 88% patients have reduced PEmax.
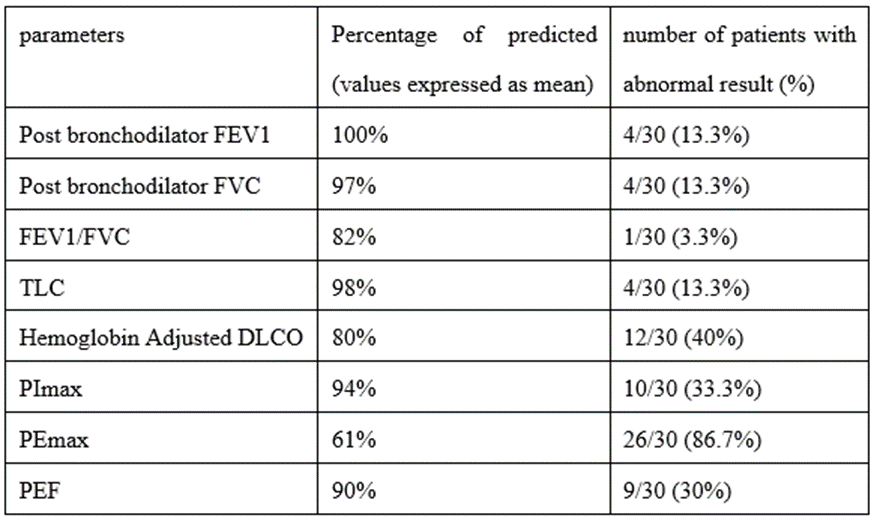
Table 1: First PFT result (number = 30)
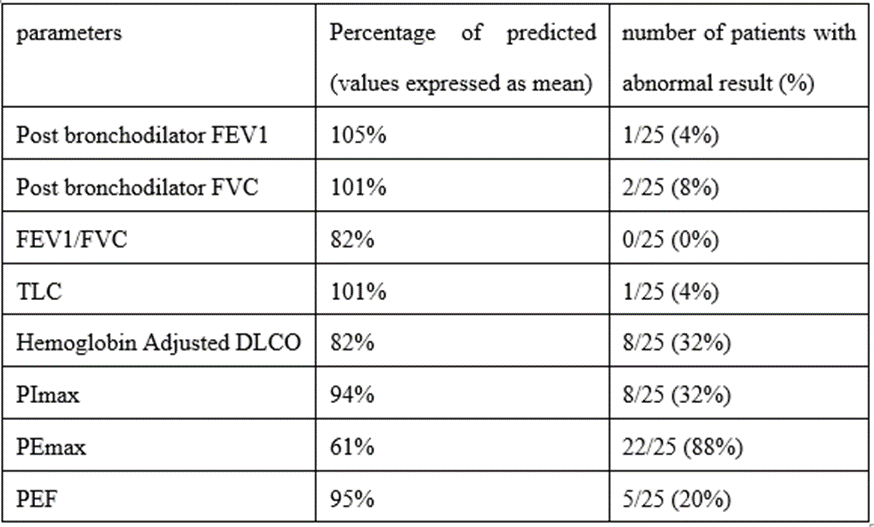
Table 2: First PFT result of patients with good past health (number = 25)
The six-minute walk test results of COVID-19 survivors within 60 days after discharge, compared with Hong Kong normative data, were shown in table 3. The exercise capacity of COVID-19 survivors was significantly lower than normal subjects in most age groups. Two patients had SpO2 < 88>
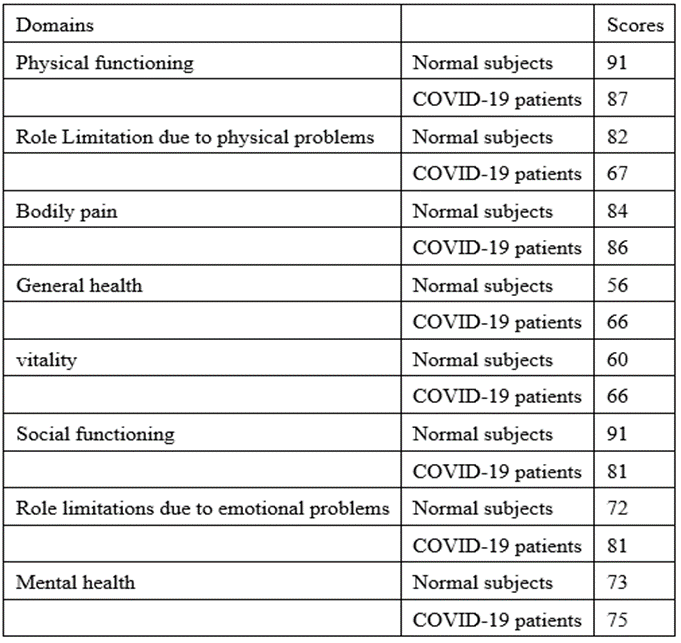
The SF-36 scale scores between Hong Kong normal subjects and COVID-19 survivors were summarized in table 4. COVID-19 survivors have lower quality of life in the context of physical functioning, social functioning and role limitation due to physical problems, compared with normal subjects. Table 4:
For patients with serial lung function performed, adjusted DLCO and PImax improved with time.
Among 9 patients with abnormal adjusted DLCO in the first lung function, 6 patients improved (figure 1).
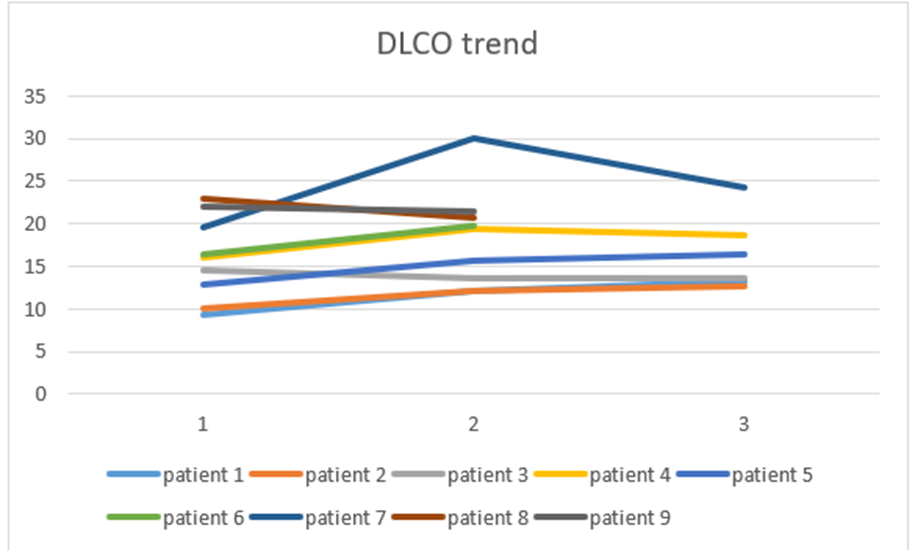
Figure 1: showing adjusted DLCO trend
Among 10 patients with abnormal PImax in the first lung function, 8 patients improved (figure 2).
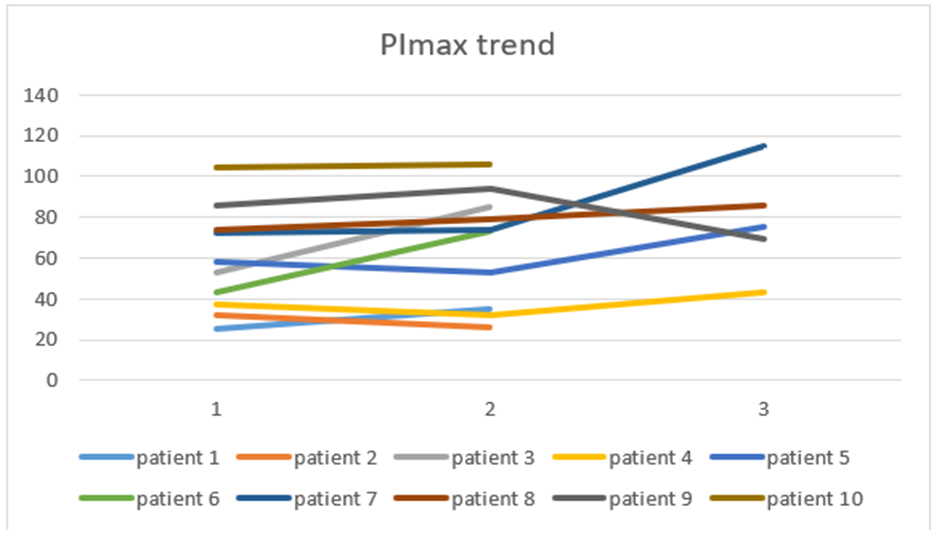
Figure 2: showing PImax trend
Among 21 patients with abnormal PEmax in the first lung function, 8 patients improved (figure 3).

Figure 3: showing PEmax trend
Our study demonstrated that 40% of the COVID-19 survivors in Hong Kong had abnormal lung function in terms of reduced diffusing capacity of carbon monoxide within 60 days after discharge, which improved with time. COVID-19 survivors also have reduced six-minute walk distance and impaired quality of life in terms of physical functioning, social functioning and role limitation due to physical problems.
For COVID-19, lung function outcome was reported in different countries. In China, impaired diffusing-capacity, lower respiratory muscle strength, and lung imaging abnormalities were detected in more than half of the COVID-19 patients in early convalescence phase [5]. In Swiss, lung function was normal for patients with mild to moderate disease, but patients with severe disease had a DLCO 20.9% lower [6]. In Austria, 22% of COVID-19 survivors had reduced DLCO 100 days after the diagnosis [7]. In Italy, restrictive lung defect was identified 6 weeks after the infection [8]. In the United Kingdom, interstitial lung disease was diagnosed in 4.8% of survivors, predominantly organizing pneumonia [9]. A systematic review involving 380 patients identified a prevalence of 0.39 for reduced DLCO after the infection [10].
Up to 86.7%of our cohort demonstrated abnormal maximal respiratory pressure. The possible reasons include technical problems such as mouth leakage, muscle weakness due to prolonged bed rest during hospital stay, steroid related myopathy if steroid was used for immune-modulation during admission [11] and COVID-19 associated myositis [12].
The limitations of this study include small sample size, high exclusion rate and single center study. First, at the beginning of the COVID-19 outbreak in Hong Kong, many patients were travelers and they left Hong Kong after discharge. Second, strict infection control regulations were observed during the outbreak, so lung function test was less available. Third, many patients refused follow up lung function tests because they were asymptomatic after recovery. The change in lung function parameters over time thus cannot be traced.
However, our study result is consistent with overseas studies on COVID-19 outcome [5,7] and studies on SARS outcome [1,2]. Follow up of discharged COVID-19 patients was warranted, given the impaired
DLCO. The British Thoracic society provided guidance for respiratory follow up of COVID-19 survivors [13]. For patients with severe pneumonia, a clinical review at 4-6 weeks after discharge was suggested and full lung function test at 12 weeks should be considered. For patients with mild pneumonia, a follow up CXR at 12 weeks after discharge is recommended.
COVID-19 leads to lung function abnormalities including reduced diffusing capacity of carbon monoxide, maximal inspiratory pressure and maximal expiratory pressure in more than 40% of patients. Exercise capacity and health status of COVID-19 survivors are lower than normal subjects.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
