
Research Article | DOI: https://doi.org/10.31579/2637-8892/303
1 Clinique Médico-Psychiatrique de Lomé (Togo)
2 Centre of Psychotraumatology and Mediation, Neuchâtel, affiliated @ SIPM: Swiss Institute for Postgraduate and Continuing Medical Education Neuchâtel, Switzerland
3 Centre Psychothérapique de l’Orne (France) 2 Centre Psychothérapique de l’Orne (France)
4 Clinic of Adolescents and Young Adultes Resilient (CAYAR), PSI: PSY-SCAN Institute, Neuchâtel, Switzerland
5 Centre Hospitalier Régional de Tsévié (Togo)
6 Université de Lomé (Togo)
7 Département de Psychiatrie, CHU de Lomé, Togo
8 Centre of Psychotraumatology and Mediation, Yaoundé, IPM-Cameroon, subsidiary of IPM-International, Switzerland.
*Corresponding Author: Lidawouwè Ahloma, Issack BIYONG. Clinique Médico-Psychiatrique de Lomé (Togo), Centre Psychothérapique de l’Orne (France) 2 Centre Psychothérapique de l’Orne (France), Centre of Psychotraumatology and Mediation, Neuchâtel, affiliated @ SIPM: Swiss Instit
Citation: Lidawouwè Ahloma, Issack Biyong, Sidonie L. Ngo Ndjebet, Similiwa Koulou Dassa, Bayaki Saka, (2024), The Impact of acne on the mental health of women and young adults, a case-control multicenter study of 300 patients in Lomé, Togo, West Africa, Psychology and Mental Health Care, 8(8): DOI:10.31579/2637-8892/303
Copyright: © 2024, Lidawouwè Ahloma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 September 2024 | Accepted: 07 October 2024 | Published: 15 October 2024
Keywords: acne; anxiety; mental health; sociodemographic; women, gender; young adults
Background: This study explores the relationship between acne and anxiety, both common health issues among young adults. Acne, a chronic inflammatory skin condition, can significantly impact an individual's self-esteem and quality of life. Anxiety, characterized by feelings of imminent danger and distress, often exacerbates this impact. While the association between acne and anxiety has been well-studied in developed countries, research in Africa, particularly in Togo, is limited.
Materials and Methods: A case-control study was conducted over eight months, from July 2017 to February 2018, in three public dermatology clinics in Lomé, Togo. The study included 300 acne patients, matched with 600 controls based on age (±5 years) and gender. Data were collected through structured interviews, clinical examinations, and validated questionnaires like the General Anxiety Disorder-7 (GAD-7) for anxiety assessment.
Results: Out of 4,126 dermatology patients, 300 (7.3%) consulted for acne, with young adults representing the majority. The study found a significant correlation between acne and anxiety, with a higher prevalence of anxiety among acne patients compared to the control group.
Conclusion: The findings highlight the psychological burden and mental health impact of acne in young adults in general and of women, emphasizing the need for a holistic approach to acne treatment that includes mental health support integrated in dermatologic treatment. Further research is recommended to explore this relationship in different African cultural contexts.
Acne and anxiety are two common health issues among young adults. Acne is a chronic inflammatory disease of the pilosebaceous follicle involving the sebaceous gland, follicular epithelium, Propionibacterium acnes, and innate immunity [1]. This condition can cause painful and unsightly skin lesions, as well as a deterioration in self-esteem and quality of life. On the other hand, anxiety is a feeling of imminent but undefined danger accompanied by discomfort, restlessness, distress, and even annihilation [2].
The pathophysiology of acne results from several factors, including excessive sebum production (hyperseborrhea), proliferation of epithelial cells in the follicular canal, a bacterium called Propionibacterium acnes, and an innate immune response of the skin. According to a study published in the "International Journal of Women's Dermatology" in 2018, testosterone may be involved in hyperseborrhea and the proliferation of epithelial cells in the follicular canal, which can lead to follicle obstruction and comedone formation. As for the epidemiology of acne, it is widespread worldwide. According to a study published in the "Dermatology" journal in 2002, acne affects approximately 80% of the global population. Moderate to severe acne represents about 20% of all acne cases. According to a study published in the "Journal of the American Academy of Dermatology" in 2004, prognostic factors for acne severity include hyperseborrhea, acne onset after the age of 17, acne extension on the back, stress in both sexes, and family prevalence of acne. Indeed, acne in adults (both men and women) is on the rise and affects approximately 40% of adults. However, according to a study conducted by the National Institute of Arthritis and Musculoskeletal and Skin Diseases in 2011, acne is the most common skin problem among adults, affecting about 54% of men and 40% of women aged 25 to 44. Other studies, such as those conducted by the Journal of the American Academy of Dermatology, have shown that adult acne is a growing problem, especially among women, with a prevalence estimated between 12% and 22%. Furthermore, acne is one of those conditions that can have a significant impact on the patient's quality of life, ranging from social withdrawal to depression and even suicide. Acne and anxiety are common issues among young adults, with acne being a chronic inflammatory disease involving the sebaceous gland, follicular epithelium, Propionibacterium acnes, and the skin's innate immunity. It can significantly affect self-esteem and quality of life due to painful, unsightly lesions. Anxiety, on the other hand, manifests as feelings of undefined danger, discomfort, and distress. Studies, such as those from the Journal of the American Academy of Dermatology, indicate that acne is associated with an increased risk of anxiety, social withdrawal, and even depression.
Anxiety, on the other hand, is a feeling of intense and persistent worry, often without apparent cause, which can interfere with daily activities and negatively affect quality of life [3]. Anxiety can also be associated with other psychological disorders such as depression and social phobia [4]. It can be very distressing and have a significant impact on the lifestyle of those who suffer from it. Indeed, individuals with acne may feel uncomfortable or even depressed, which can impact their mental health. This can also lead to significant anxiety [5].
Studies have shown that the risk of anxiety is higher in individuals with acne compared to the general population. A study conducted in 2002 revealed that 50% of patients with severe acne also suffered from anxiety [1]. Another study in 2009 demonstrated that acne patients were twice as likely to experience anxiety compared to the general population [2]. The impact of acne on mental health can be measured using various tools, such as the General Anxiety Disorder-7 (GAD-7), which is a questionnaire consisting of 7 items that screen for anxiety in patients. Other scales, such as the Hospital Anxiety and Depression Scale (HADS), measuring anxiety and depressive disorders, and the Liebowitz Social Anxiety Scale (LSAS), assessing social anxiety disorder, can also be utilized. The relationship between acne and anxiety is a extensively researched topic in developed countries [6]. However, limited work has been conducted on this subject in Africa. The complex and multifactorial relationship between acne and anxiety can be influenced by several factors, such as the negative impact of acne on physical appearance and quality of life [7]. Indeed,in the The Journal of Clinical and Aesthetic Dermatology the skin and the nervous system have a close relationship due to their common origin from the ectoderm and sensitivity to the same neurotransmitters during embryological development. The skin, being visible and playing a crucial role in the expression of emotions, is essential for self-esteem and socialization. However, acne, often affecting the face, can have a negative impact on the individual's psychological state due to its visibility and difficulty to conceal. A study has demonstrated that individuals with acne exhibit higher levels of anxiety than the general population [2]. In Africa, acne is often considered commonplace or normal, and dermatologists may underestimate the prevalence of psychiatric comorbidities. Individuals with acne may struggle with body image and interpersonal relationships, leading to anxiety. However, no study has been conducted to determine the association between acne and anxiety in the specific country mentioned. Studies have been conducted in various countries, including Africa, Europe, Asia, and America, to explore the correlation between acne and anxiety [8-13]. In Togo, one study examined the impact of artificial depigmentation on acne [14]. Another study investigated the clinical aspects and quality of life of acne patients in Lomé [1]. However, no study has yet examined the correlation between acne and anxiety in this particular country. In this context, this article aims to examine the relationship between acne and anxiety in Lomé, Togo, using a case-control study design.
• Determine the socio-demographic characteristics of acne patients: This objective aimed to understand the social and demographic factors that may influence the presence of acne in patients, such as gender, age, occupation, etc.
• Describe the clinical characteristics of acne patients: The objective was to understand the specific characteristics of acne, such as the location and severity of lesions, as well as the duration of the condition among patients.
• Determine the correlation between acne and anxiety: The ultimate goal of the study was to determine if there is a correlation between the presence of acne and levels of anxiety among patients. The objective was to understand if there is a relationship between physical appearance and the psychological state of patients.
We conducted a case-control study from July 2017 to February 2018, spanning a period of 8 months, in the three public dermatology services in the city of Lomé. Each case was matched with two controls based on age (± 5 years) and gender. We included, with their consent, all patients diagnosed with acne by a dermatologist. Patients who decided to withdraw from the study were not included. The sample was open to all patients, and recruitment was consecutive and exhaustive.
In International Journal of Epidemiology inclusion Criteria: Male or female patients of any age diagnosed with acne by a dermatologist in the three public dermatology services in Lomé and who gave their consent. Exclusion Criteria: Patients who refused to participate in the study.
Principles of Epidemiology in Public Health Practice: Control Definitions in Clinical Studies,". Inclusion Criteria: Male or female subjects without acne lesions who gave their consent. Exclusion Criteria for Controls: Subjects without acne lesions who refused to participate in the study.
2. Data Collection:
Data collection was done using a pre-established form (Annex: please provide the names of the different forms and questionnaires used in this study without specifying "Annex"). The interview collected sociodemographic parameters (age, gender). Adolescents were considered as patients aged 12 to 17 years, young adults as those aged 18 to 25 years, and adults as those above 25 years old.
The recruitment of cases was done during dermatology consultations. The physical examination conducted by the dermatologist specified the types of lesions present, their location, and clinical forms. The clinical evaluation of acne was done using the ECLA grid.
The recruitment of controls was done among companions, medical personnel, as well as outside of hospital settings (universities, markets, streets, public and private services, etc.).
The total ECLA score, obtained by adding the scores of factors F1, F2, and F3, ranged from 0 to 36. An ECLA score of 12 or lower represented mild to moderate acne, while a score higher than 12 represented severe acne.
b. GAD-7 score
To assess anxiety, each item on the GAD-7 was rated from 0 to 3: 0=never; 1=several days; 2=more than half the time; and 3=nearly every day. The total score was obtained by adding the scores of each item, ranging from 0 to 21. A GAD-7 score of 10 or higher, with a sensitivity of 89% and specificity of 82%, indicated the presence of anxiety [17]. The results were interpreted as follows: a score below 10 indicated the absence of anxiety, while a score of 10 or higher confirmed the presence of anxiety.
4. Data analysis:
After data collection, the forms were entered into a database designed using Epidata software version 3.1. Statistical analysis was performed using R Studio software version 3.4.3. It included descriptive analysis of the population and comparative analysis. In the descriptive analysis, the characteristics collected for cases (enrollment center, age groups, observed acne lesions, clinical forms of acne) were presented as frequencies and percentages for qualitative variables, or as mean and standard deviation for quantitative variables. In the comparative analysis, the statistical tests used were the paired Student's t-test (for comparing two quantitative variables) and the McNemar test (for comparing two qualitative variables).
General Results:
A total of 900 subjects were recruited, including 300 cases (33 adolescents, 175 young adults, and 92 adults) with acne and 600 controls without acne. The controls were matched to the cases based on age (± 5 years) (two controls for each case) and gender. Young adults represented two-thirds in both groups (Figure 1).
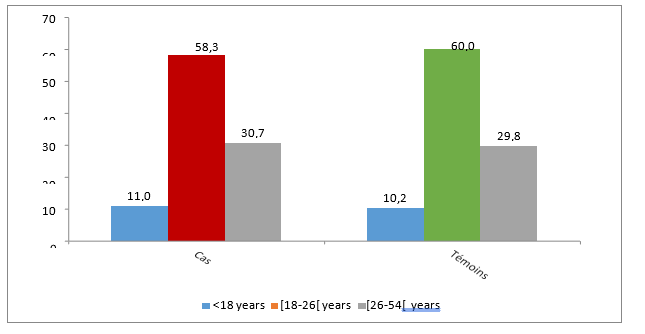
Figure 1: Distribution of cases and controls by age
During the study period, 300 out of 4,126 patients received in dermatology (7.3%, 95% CI [6.5-8.1%]) consulted for acne. Among the 300 acne patients, 167 were recorded at the Gbossimé Dermatology Center (Figure 2).
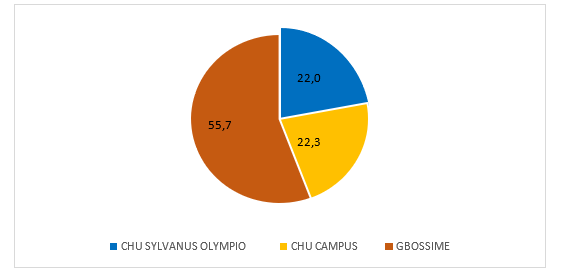
Figure 2: Source distribution of patients
Out of the 300 patients, 214 were female, resulting in a sex ratio (M/F) of 0.4. The mean age of the cases was 23.7±5.7 years (range: 12 to 52 years). The mean age of the controls was 23.6±6.2 years (range: 12 to 54 years), with no significant difference between the two groups (p=0.9362).
The most commonly observed acne lesions were papules (97.3%), followed by seborrhea (92.3%), and comedones (90.7%) (Table 1).
| Acne lesion | Number | % |
| Wheals | 292 | 97,3 |
| Hyper seborrhoea | 277 | 92,3 |
| Comedones | 272 | 90,7 |
| Hyper-pigmented macules | 249 | 83,0 |
| Pustules | 217 | 72,3 |
| Excoriation | 177 | 59,0 |
| Scabby points | 120 | 40,0 |
| Punctuform depressions | 104 | 34,7 |
| Nodules | 95 | 31,7 |
| Cysts | 83 | 27,7 |
| Atrophic scars | 33 | 11,0 |
| Hypertrophic scars | 23 | 7,7 |
Table 1: Types of observed acne lesions
Papulopustular acne was the most common clinical form (200/300; 66.7%), followed by retentional acne (Table 2).
| Acné | Number | % |
| Papulo pustular | 200 | 66.7 |
| Retentional | 58 | 19.3 |
| Nodular | 35 | 11.7 |
| Pigmentary | 7 | 2.7 |
| Total | 300 | 100 |
Table 2 : Clinical forms of acne
The face w affected in 100% of cases, either alone or in combination with other locations (Table 3).
| Acne lesion | Nomber | % |
| Face | 300 | 100,0 |
| Back | 190 | 63,3 |
| Back, above scapula | 123 | 41,0 |
| Back, below scapula | 67 | 22,3 |
| Neck | 140 | 46,6 |
| Neck, upper cervical area | 88 | 29,3 |
| Neck, lower cervical area | 52 | 17,3 |
| Chest | 136 | 45,3 |
| Arms | 60 | 20,0 |
Table 3: Locations of observed acne lesions
This questionnaire allowed us to identify 72 cases of anxiety among our 300 acne patients, representing a prevalence of 24.0% (95% CI 19.4-29.3). We identified 37 cases of anxiety among the 600 control subjects, representing a prevalence of 6.2% (95% CI 4.44-8.48). The GAD-7 scores among the cases ranged from 0 to 21, with a mean score of 6.5±4.9. The mean GAD-7 score among the controls was 2.9±3.8 (range 0-21) with a significant difference between the two groups (p < 0>Anxiety Cas (n=300) Controls (n=600) p-value Yes 72 (24,0) 37 (6,2) <0> No 228 (76,0) 563 (93,8)
Table 4: Comparison of Anxiety between Cases and Controls
The GAD-7 scores ranged from 0 to 21 among adolescents. We identified 5 cases of anxiety among our 33 adolescent acne patients (15.2%) and 2 cases of anxiety among the 62 adolescent control subjects (3.2%). The mean GAD-7 score among the cases was 5.7±4.4 (range 0-18) compared to 2.6±3.8 (range 0-21) among the controls, with a statistically significant difference in the GAD-7 score between the two groups (P value = 0.0472).
The GAD-7 scores ranged from 0 to 21 among young adults. We identified 49 cases of anxiety among our 175 young adult acne patients (28.0%) and 20 cases of anxiety among the 358 young adult control subjects (5.6%). The mean GAD-7 score among the cases was 6.9±5.1 (range 0-21) compared to 3.0±3.7 (range 0-21) among the controls, with a statistically significant difference in the GAD-7 score between the two groups (P value < 0>
The GAD-7 scores ranged from 0 to 19 among adults. We identified 18 cases of anxiety among our 92 adult acne patients (19.6%) and 15 cases of anxiety among the 180 adult control subjects (8.3%). The mean GAD-7 score among the cases was 6.1±4.7 (range 0-18) compared to 2.8±3.9 (range 0-19) among the controls, with a statistically significant difference in the GAD-7 score between the two groups (P value < 0>
| Anxiety | (n=300) | Controls (n=600) | p-value |
| Teenagers | |||
| Yes | 5 (15,2) | 2 (3,2) | 0,0472 |
| No | 28 (84,8) | 60 (96,8) | |
| Young adults | |||
| Yes | 49 (28,0) | 20 (5,6) | <0,0001 |
| No | 126 (72,0) | 338 (94,4) | |
| Adults | |||
| Yes | 18 (19,6) | 15 (8,3) | <0> |
| No | 74 (80,4) | 165 (91,7) | |
Table 5 : Comparison of Anxiety and Age Groups
In our series, regardless of gender, anxiety was more commonly found among cases (19.8% in males and 25.7% in females) compared to controls (1.6% in males and 7.5% in females), with a statistically significant difference (p value < 0>Anxious (n=300) Controls (n=600) p-value Male Yes 17 (19,8) 3 (1,6) <0> No 69 (80,2) 186 (98,4) Feminine Yes 55 (25,7) 30 (7,5) <0> No 159 (74,3) 371 (92,5)
Table 6 : Comparison of Anxiety and Gender
Among adolescents, regardless of gender, there was no statistically significant difference in anxiety between the inclusion status (cases and controls) (p value > 0.05).
| Anxious | (n=33) | Controls (n=62) | P-value |
| Male | |||
| Yes | 2 (12.5) | 0(0.0) | 0.1159 |
| No | 14(87.5) | 30(100,0) | |
| Feminine | |||
| Yes | 3(17.7) | 2 (6.3) | 0.3257 |
| No | 14(82.3) | 30 (93.7) | |
Table 7 : Comparison of Anxiety and Gender in Adolescents
Among young adults, regardless of gender, anxiety was more commonly found among cases (26.8% in males and 28.6% in females) compared to controls (1.6% in males and 6.5% in females), with a statistically significant difference (p value < 0>Anxious Cas (n=175) Témoins (n=354) Valeur de p Masculin Oui 15 (26,8) 2 (1,6) <0> Non 41 (73,2) 122 (98,4) Féminin Oui 34 (28,6) 15 (6,5) <0> Non 85 (71,4) 215 (93,5)
Table 8: Comparison of Anxiety and Gender in Young Adults
Among adults, anxiety was more commonly found among female adult cases (23.1%) compared to controls (9.4%) with a statistically significant difference (p value = 0.0056).
| Anxious | Cas (n=92) | Controls (n=174) | p-value |
| Male | |||
| Yes | 0 (0,0) | 1 (2,9) | 0,9999 |
| No | 14 (100,0) | 34 (97,1) | |
| Féminine | |||
| Yes | 18 (23,1) | 13 (9,4) | 0,0056 |
| No | 60 (76,9) | 126 (90,6) | |
Table 9: Comparison of Anxiety and Gender in Adults
The mean ECLA global severity score was 12.3±5.0 (range: 2 to 28). Acne was classified as mild to moderate in 162 patients (54.0%) and severe in 138 patients (46.0%). The mean ECLA score was 11.7±5.1 (range: 3 to 28) among anxious patients and 12.5±5.0 (range: 2 to 28) among non-anxious patients, with no statistically significant difference (p value = 0.2183) (Table X). Only 25 out of the 72 anxious patients (34.7%) had severe acne. The severity of acne was not correlated with anxiety scores (GAD-7: r = -0.02; p = 0.6724).
The Association between Acne and Anxiety:
Our study revealed that 24.0% of acne cases (72 out of 300 patients) had symptoms of anxiety, compared to only 6.2% of controls (37 out of 600), indicating a significant association between acne and anxiety. These results are consistent with a meta-analysis of 42 previous studies that found a modest but significant positive correlation between acne and anxiety, with a correlation coefficient of r = 0.25 [1].
Influence of Gender and Age on Anxiety in Acne Patients:
In our study, we found that anxiety was more prevalent in women with acne (25.7%) compared to men (19.8%). This trend is also observed in the general population, with a study from Harvard Medical School estimating that women are nearly twice as likely as men to suffer from anxiety disorders [5].
Regarding age, our study revealed that anxiety was most common among young adults with acne (28.0%), compared to adolescents (15.2%) and older adults (19.6%). This trend is also consistent with existing literature. For example, a study from the World Health Organization (WHO) found that the prevalence of anxiety disorders is generally higher in individuals aged 15 to 34 years [6].
Severe acne and anxiety:
In our sample, only 34.7% of anxious patients had severe acne. This finding challenges the common hypothesis that the severity of acne is directly proportional to the level of anxiety. Previous research has suggested a positive correlation between acne severity and anxiety [7], but other studies have noted that even mild to moderate acne can have significant psychological effects, emphasizing the importance of individual perceptions of acne [8].
In conclusion, our study, in line with numerous internationally conducted research, has highlighted a significant link between acne and an increased prevalence of anxiety, particularly among women and young adults. It is essential for healthcare professionals to be aware of this association in order to intervene early and appropriately, as these conditions can have a devastating impact on the mental health and quality of life of affected individuals.
As suggested by numerous studies, such as those by Dreno et al. (2018) and Tan et al. (2018), an integrated approach to the treatment of acne and anxiety could significantly improve the quality of life and self-esteem of patients. Furthermore, the role of mental health interventions, particularly cognitive-behavioral therapy, is increasingly recognized as an essential component of the overall management of patients with acne.
It is now more important than ever to advance our understanding of the relationship between acne and anxiety in order to propose integrated and effective treatment strategies. This way, every patient with acne can benefit from a tailored care plan that considers both the physical and psychological aspects of this complex condition.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
