
Research Article | DOI: https://doi.org/10.31579/2692-9406/179
Department of Chemistry, College of Natural and Computational Sciences, Mekdela Amba University, P.O. Box 32, Tulu Awuliya, Ethiopia.
*Corresponding Author: Abyt Ibraimov, Department of Chemistry, College of Natural and Computational Sciences, Mekdela Amba University, P.O. Box 32, Tulu Awuliya, Ethiopia.
Citation: Abyt Ibraimov, (2024), The human body heat conductivity: its origin, evaluation, and significance, J. Biomedical Research and Clinical Reviews. 9(1); DOI:10.31579/2692-9406/179
Copyright: © 2024, Abyt Ibraimov, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 January 2024 | Accepted: 30 January 2024 | Published: 09 February 2024
Keywords: human body heat conductivity; cell thermoregulation; condensed chromatin; chromosomal heterochromatin regions; obesity; alcoholism; drug addiction
The biological role of “excess DNA” in eukaryotes, which consists of short repeating sequences of nucleotides and does not code for proteins and enzymes remains unclear. The part of this DNA in the interphase cell is complexed with proteins into highly compacted structures, referred to as condensed chromatin, and they appear on metaphase chromosomes in the form of heterochromatin regions. The purpose of this article is to provide rationalization for the hypothesis, that it is possible that in higher eukaryotes the biological role of non-coding DNA, which form a dense layer of condensed chromatin around the cell nucleus in the interphase cell, is their participation in maintaining intracellular temperature homeostasis. Although the issue of thermoregulation at the cellular level is not yet on the agenda of scientists, nevertheless, an attempt has been made to collect data indicating the possibility of the existence of such a phenomenon. Since direct in vivo measurements of temperature changes in different parts of the cell are not yet technically possible, indirect methods for studying the supposed phenomenon (cell thermoregulation) by studying the heat conductivity of the human body and the number of chromosomal heterochromatic regions in his genome are proposed. It is assumed that the phenotypic manifestation of the cell thermoregulation at the level of the human organism is the level of his body heat conductivity, which significance is to be assessed in normal and pathological conditions.
Heat conductivity (HC) is the transfer of energy from more heated parts of the body to less heated ones because of thermal motion and interaction of micro particles. HC leads to the equalization of body temperature. It is commonly known that HC due to the transfer of energy is one of the three transfer phenomena existing in Nature (heat conductivity, diffusion and internal friction or viscosity). All substances have HC: gases, liquids and solids. Unlike gases and liquids, convection is not possible in solids, therefore, the thermal transfer is carried out only by heat conductivity.
The study of the HC of nonliving bodies is a developed section of physics and technology, which is more than can be said about the bodies of living organisms. From the literature available to us, we were not able to find out why studies of thermoregulation in animals and humans are carried out without taking into account the level of HC of their bodies. For example, when talking about the HC, for example, of the skin, we usually mean the degree of blood supply through changes in the expansion of the lumen of the vessels, and not its initial physical HC, i.e., convection, not conduction. It may have been, this is due to the fact that, a) it is difficult to measure the HC of the body of living organisms in vivo due to the heterogeneity of physical density of their cells, tissues and organs; b) the constant circulation of blood, lymph and tissue sap throughout the body; c) temperature difference between the core (core temperature) and the outer skin of the body.
The origin of the idea of human body heat conductivity.
We began to pay attention to the possible role of body heat conductivity (BHC) in human life activity for a number of objective reasons. The vast majority of scientists in Kyrgyzstan are directly or indirectly engaged in the study, including biomedical problems, of indigenous and non-indigenous individuals in the high-altitude climate of the Pamirs and Tien Shan. The fact is that the main sources of material wealth of the country are extracted (mineral resources, including large reserves of precious and rare earth metals) and produced (distant cattle breeding) in conditions of high altitudes.
Interest in human physiology and pathology to the extreme climate of high altitudes suddenly became relevant in connection with the invasion of the USSR troops into Afghanistan, when the problem of human adaptation to high altitudes became a problem of paramount importance. In particular, there was an acute problem of selecting a military contingent capable of fighting in high altitude conditions without compromising their health. Looking ahead, we note that this task - scientifically based selection of individuals capable of successful adaptation to high altitudes above sea level - has not yet been solved.
Many facts and observations indirectly indicate the possibility of the existence of a variability in the human BHC in a population:
1. The thermoregulation is best developed in humans, then in primates and in predators;
2. Individuals in a population differ in their tolerance to high and low temperatures;
3. Comparative tests of the endurance of white-skinned people and black-skinned people to physical activity in conditions of hot weather and high humidity revealed the superiority of black-skinned people even over those white-skinned people who have long been accustomed to working in these conditions. It was shown that the rectal temperature in black-skinned people turned out to be significantly less elevated than in white-skinned people during standard physical exercises in hot weather conditions; black-skinned people sweated much less than white-skinned people, while collapse occurred ten times more often among white-skinned people than among black-skinned people [1].
4. The study of the comparative performance of the Eskimos in the Arctic, well-trained soldiers of the army and pilots of the US Air Force who did not undergo special training in Alaska, found that the Eskimos are 3.5 times more endurance than the pilots and 2.5 times the soldiers.1 On the other hand, during the Korean War, frostbite was much more common among black-skinned soldiers than among white-skinned ones [1].
5. A high risk of developing pulmonary edema in the high-altitudes is observed in adolescent boys (pre-adolescent period) and young men. Clinical observations are often limited to stating the accumulation of fluid in the lungs, but the exact genetic causes of the disease are not known, since the disease has a tendency to recur in the same individuals.
6. It is generally accepted that the level of cellular metabolism is strictly limited and it is set by the Nature. Humans consume and expend several hundred kilocalories more per day than higher primates expend, that is, our metabolism is adapted to more rapid burning. How, in such a case, does a human manage to get rid of excess heat produced by his increased cellular metabolism?
7. The uniqueness of human, in addition to all his known features, also lies in the fact that only he managed to populate the entire surface of the Earth, including such extreme environments as the Far North and high-altitude regions, while remaining a single, tropical species. Moreover, all this happened in a very short period of time (about 30,000 - 50,000 years), this event is unprecedented in the evolution of life [2].
But the crucial fact that induced us to study the variability of the human BHC in the population, in normal and pathological conditions, was the completion of the physical mapping of the human genome (The Human Genome Project), when it finally became clear that the gene part makes up less than 2% of the DNA in the human genome. The remaining 98% of the DNA in the human genome is the so-called non-coding DNA. About 15%-20% of this non-coding part of human DNA form the so-called constitutive heterochromatin, which can be detected and studied under an optical microscope.
One of the important results of the study of human chromosomes is the detection of hereditary polymorphism at the chromosomal level. It turned out that this polymorphism is due to the high quantitative and qualitative variability of chromosomal constitutive heterochromatin regions (HRs). Numerous studies on various plant, animal and human species have shown the universality of the phenomenon of chromosomal HRs variability [3,7].
Two types of constitutive heterochromatin have been identified to date: С- and Q- heterochromatin. There are some significant differences between them [8]. Regarding our study, it is enough to note, that chromosomal C-heterochromatin regions (C-HRs) are present in the genome of all plants, animals and humans, while Q-heterochromatin regions (Q-HRs) are present in the genome of only three higher primates: humans, chimpanzees and gorillas [9.10].
The main features of the chromosomal C- and Q-HRs are: a) they are made up primarily of short, highly repetitive DNA sequences; b) HRs occupy quite specific regions of the chromosomes that are very important, namely: regions of centromeres and telomeres, as well as nucleolar organizer regions carrying ribosomal RNA genes; c) wide intraspecific variability (polymorphism) and evolutionary fixedness in the genome of higher eukaryotes. In this sense, the chromosomal HRs is a genetically inert material. It may have been that is why the issue of the role of chromosomal HRs performed by them in the process of life of a cell, organism, and population is still not clear.
Finally, our long-term studies of chromosomal HRs variability in human populations living in different climatogeographic conditions of Eurasia and Africa, as well as in some purely human forms of pathology (obesity, alcoholism, drug addiction, and high-altitude pulmonary edema) have shown that, apparently, chromosomal HRs are related to thermoregulation at the level of individual cells (cell thermoregulation), the phenotypic manifestation of which is the level of body heat conductivity in individuals [11,14].
Evaluation of the human body heat conductivity.
The HC of the human body, as one of the types of physical characteristics of the human body, has never been purposefully studied by anyone, although such a possibility cannot be denied from the point of view of physics. In fact, there is nothing new in the very idea that the human body must have some HC. However, it has not yet attracted the attention of either physicists or physiologists as an important physical characteristic of the human body. It would appear that this is due to the known physical heterogeneity (in the sense of density) of the human body. In addition, direct HC (conduction) is of relatively little importance in the redistribution of heat in the human body, because most tissues do not conduct heat well. Perhaps that is why we failed to find in the literature not only a special method, but also even any attempts to evaluate the body heat conductivity of living organisms in vivo.
We believe that cell thermoregulation underlies body heat conductivity (BHC) [11,12]. Since direct in vivo measurement of the temperature of different parts of cells is still not possible, then it was decided to somehow indirectly estimate the heat conductivity of the whole body. We turned to the experience of thermal physicists in search of a method for measuring of the human BHC. As is known in thermal physics, the measurement of HC of solids (e.g.: metal) is carried out by determining the coefficient of thermal conductivity by the calorimetric method. The thermal transfer takes place through a metal rod, the ends of which are placed in a calorimeter with water taken at temperatures Т1 and T2 (T1 > T2). It is necessary to experimentally determine the amount of heat transferred and the time to measure the coefficient of HC of a given metal rod.
It is obvious that the direct transfer of the HC measurement method used in thermal physics is not acceptable for the human body, both for technical and ethical reasons. To do this, we had to modify the generally accepted technique of physicists so that it was acceptable to humans. Since we first reported the possibility of the existence of thermoregulation at the level of individual cells [11,12], we have developed and tried different methods that allow us to estimate human BHC in one way or another [13,16]. Looking ahead, let us just say that it is too early to say that we can measure the human BHC with the same accuracy as thermal physicists do when measuring the thermal conductivity of nonliving bodies, such as metals. At best, we can only evaluate the human BHC as high, medium, or low, and apparently, it is still far from an accurate measurement in numbers.
To evaluate BHC we had to solve a number of technical and methodological problems. First, it was necessary to determine the creation of a temperature gradient between the human body and a heat source. As is known, to determine the heat conductivity of any body, it is necessary to create a temperature difference so that thermal energy is transferred from a hot object to a cold one. By trial and error, we have established that the optimal temperature difference between the human body and the heat source is 9 ⁰C. Then we had to solve the question of which part of the human body to choose in order to assess the level of his BHC. We solved this problem by assessing the temperatures of some parts of the human body. For this purpose, we measure the temperatures of the palm, forehead, armpit or oral cavity during the temperature load (for details see) [15,16].
In methodological terms, the difference between the two approaches (transfer of thermal energy from the heat source to the human body and vice versa) to the estimation of human BHC is as follows: the first method consists in the transfer of thermal energy from the heat source (e.g., water bath with controlled temperature) to the human body, and the estimation of BHC is carried out by the time of increase in the temperature of the surface of the right palm (‘temperature peak’). According to the second approach, the transfer of heat energy occurs in the direction from the human body to the water in the thermos (the temperature of which is 9 ⁰С lower than the temperature of the surface of the left palm of the given individual), and the estimation of BHC is carried out by the value of the decrease in the temperature of the water in the thermos.
In the process of testing the these approaches it also turned out that there is a statistically significant relationship between the level of human BHC and the magnitude of the temperature difference between distant parts of his body: left armpit and surface of the right palm; oral cavity and palm; or forehead and palm surface temperature. We believe that the smaller temperature difference between distant parts of the human body reflects the high heat-conducting capacity of this organism in the sense that: a) such an organism equalizes the temperature differences between different parts of the body more efficiently; b) removes (dissipates) excess heat energy outside of the body faster.
In the process of searching for the optimal temperature of “hot” water, as a source of thermal energy for measuring human BHC, we drew attention to the well-known phenomenon that people in a population differ in palm temperature. However, it turned out that the temperature of the palm itself can give very important information about the human BHC. For example, we were able to detect the existence of statistically significant differences between individuals by gender, age, and racial and ethnic origin precisely by studying only the distribution of palm temperature in the population. The temperature of the surface of the palm at rest also reflects the BHC level; individuals with a high palm temperature have a high BHC, and vice versa (see below). Summing up, it can be argued that all approaches allow assessing the level of human BHC and are interchangeable.
Thus, we have developed several methods for estimating human BHC different in complexity (in terms of technical execution), but giving fundamentally similar results. The simplest is the estimation of human BHC by the palm surface temperature, the most complex is the measurement of heat energy transfer from one part of the body to another in the process of controlled heat load [15]. While a non-contact thermometer (pyrometer) is sufficient to measure the palm surface temperature, more complex methods of human BHC assessment require special equipment, premises and trained personnel [16].
The following describes the methodology for evaluating human BHC using the heat load method in a laboratory setting. The studied individual sat on a chair with a back, the torso was straightened, the head was raised, the arms hung naturally at the sides, and the muscles were relaxed. Then the individual slowly immersed the left hand up to the wrist in a water bath filled with “hot” water. The studied individual should not be distracted, keep the hands only in the water and not press against the wall of the water bath during the measurement of BHC. Every minute, the temperature of the surface of the right palm of the studied individual was measured with a pyrometer to the nearest tenth of degrees Celsius (in °С). For the convenience of analyzing the numerical results of experiments for all measurements, when the thermometer level coincided with an odd division, its values were underestimated by one tenth degrees, so an even number was obtained. For example, if the pyrometer showed 31.5 ºС, it was recorded as 31.4 ºС. The experiment continues (heat load on the human body through the left hand) until the temperature increase on the surface of the right palm first reaches its maximum value ("temperature peak").
How did we interpret these data? We believe that the time of the onset of the temperature peak on the surface of the right palm reflects the rate of heat transfer in the human body (from the palm of the left hand across the body to the palm of the right hand). In other words, we believe that a human with high BHC is able to: a) conduct heat through his body faster than other individuals in the population; b) equalize the temperature difference in different parts of the body faster; and c) remove (dissipate) excess thermal energy outside of his body faster in order to maintain the required temperature level in the body. If the temperature peak on the surface of the right palm occurs within the first 5 minutes from the start of the thermal load, then such an individual is considered as a human with a high BHC, from 6-10 minutes, as an average one, from 11 minutes and above, as a low BHC (for details see) [16].
The samples of individuals from different gender and age and racial and ethnic groups living in the Kyrgyz Republic (the Kyrgyz and Russians) were studied. Among them are also selected individuals who were overweight, received treatment for the abuse of hard liquor or drugs. As a control group, phenotypically healthy individuals were selected, comparable in terms of racial and ethnic origin, gender and age with the studied samples. In addition, samples of students from Pakistan, India and China studying at universities in Bishkek were studied.
The influence of height, weight, pulse rate, blood pressure, body type (constitution), gender, age and racial and ethnic origin were studied as possible factors that can affect a human BHC. The aggregate data we have obtained over the last 20 years indicate that the levels of human BHC in the population are not significantly affected by weight, height, blood pressure, pulse rate and body types (these data are not presented here).
However, BHC is influenced by gender, age, racial and ethnic origin. The influence of these factors has been studied across ethnic groups and ages using all methods of assessing human BHC and they yielded comparable results. Thus, Tables 1 and 2 illustrate examples of the existence of statistically significant differences between genders obtained using only two different methods (analyzing the distribution of temperature of the palm and the temperature difference between the palm and armpit).

Table 1. The distribution of temperature (in °С) of the palm of the hands depending on the gender.
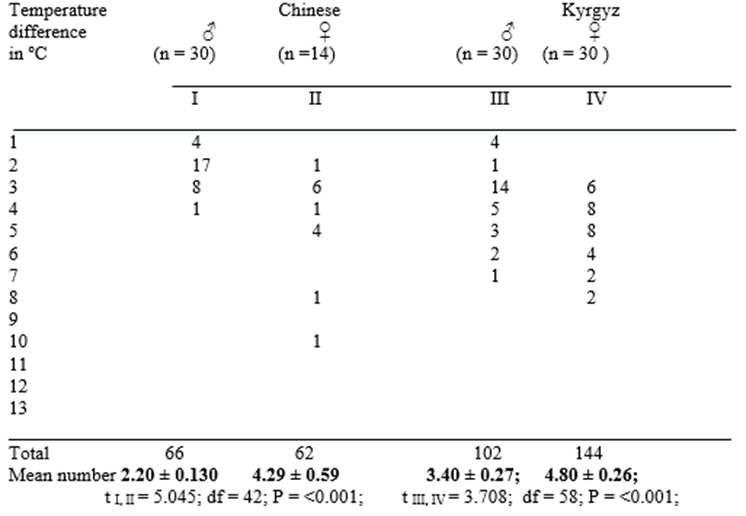
Table 2. The distribution of the temperature difference (in °C) between the palm and armpit depending on the gender of individuals.
As can be seen from these tables, both methods of BHC estimation give comparable results, although the second technique appears to be more sensitive. The same data were obtained using other methods (these data are not shown here). The effect of age on human BHC is demonstrated in Table 3, which uses, for example, analysis of the distribution of palm surface temperature alone.
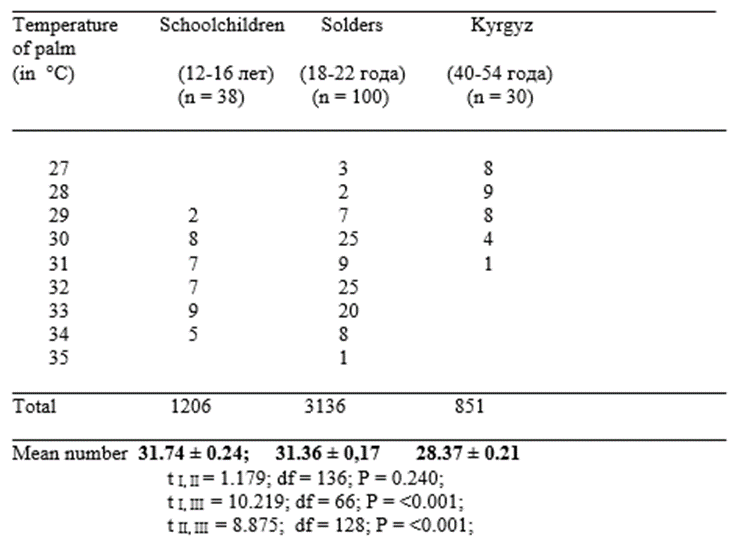
Table 3. The distribution of temperature (in °С) of the palm depending on the age (male Kyrgyz).
As can be seen from the above data, the temperature of the palm in individuals from younger age groups is on average higher than in adults. The influence of racial-ethnic characteristics on human BHC is demonstrated in Table 4 by analyzing the palm surface temperature distribution.
Table 4. The distribution of temperature (in °С) of the palm depending on the racial and ethnic origin (male students from China, India and Kyrgyzstan).
Taking into account the well-known circumstance that normally the temperature of the human armpit fluctuates within very narrow limits, and the temperature of the palms differ significantly, it seemed interesting to investigate the following; can the age, gender and racial and ethnic characteristics of individuals effect to the distribution of the temperature difference between the palm and armpit. Below it is presented an analysis of the distribution of the temperature difference between the palm and armpit in the samples that we have studied.
Table 5. The distribution of the temperature difference (in °C) between the palm and armpit depending on the age (male Kyrgyz).
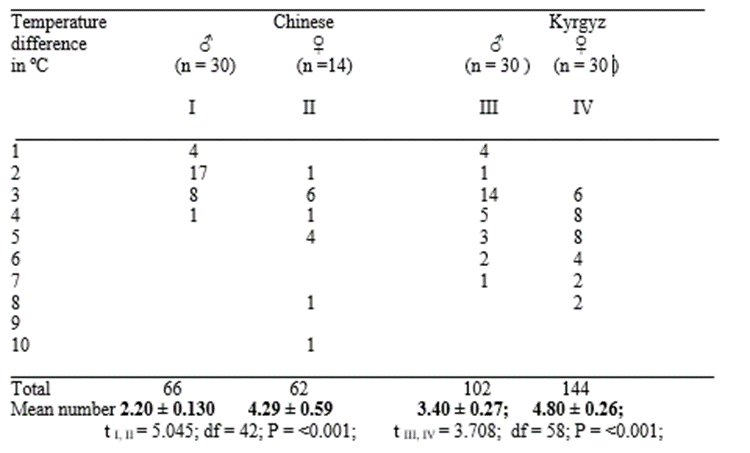
Table 6. The distribution of the temperature difference (in °C) between the palm and armpit depending on the gender of individuals.
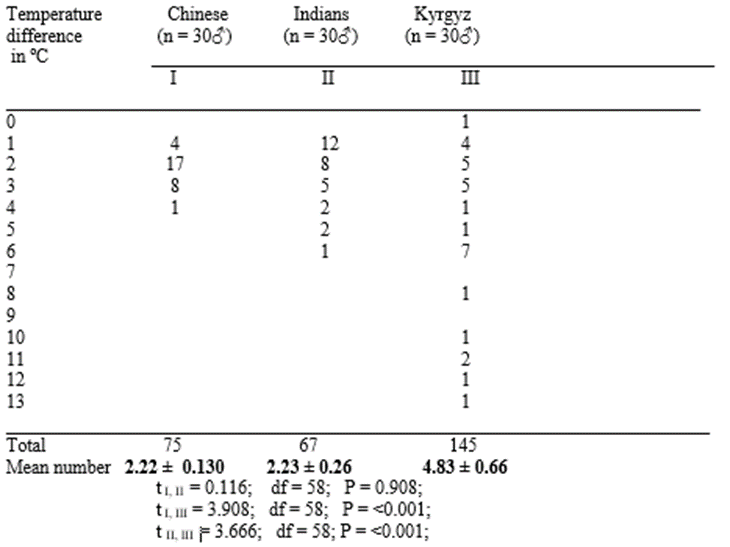
Table 7. The distribution of the temperature difference (in °C) between the palm and armpit depending on the racial and ethnic origin of individuals.
As can be seen from Table 5, the temperature difference between the palm and armpit in the elderly is significantly greater than in children. With regard to gender, it turned out that men had less temperature differences than women (Table 6) did. According to this characteristic of human BHC, the Kyrgyz differ from the Indians and Chinese in a significantly high temperature difference between the palm and armpit (Table 7). The question of why Chinese and Indians do not differ in BHC will be specifically returned to below.
Finally, the possibility of a close relationship between the temperature difference between the two distal parts of the body and the human BHC is evidenced by the data presented in Table 8. Here, for example, the distributions of BHC of individuals were compared depending on the temperature difference between the palm and armpit.
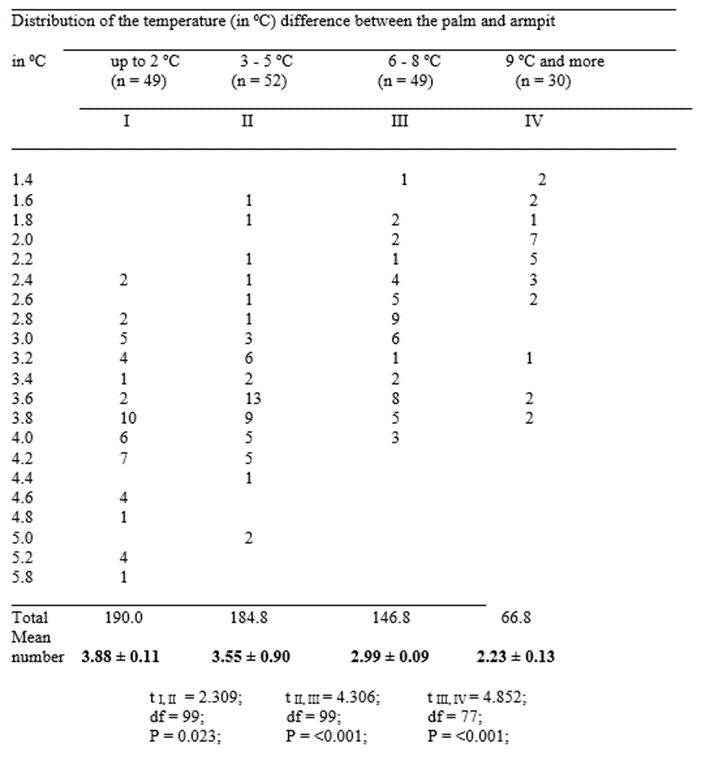
Table 8. The distribution of human BHC depending on the temperature difference (in ºC) between the palm and armpit.
As can be seen from this table, the smaller the temperature difference between the palm and armpit, the higher the human BHC, and vice versa. Thus, studies of human BHC variability in the population showed that:
a) individuals in a population differ from each other in the BHC;
b) such morphophysiological human characteristics as weight, height, physique and pulse rate do not significantly affect the body heat conductivity;
c) gender, age and racial and ethnic characteristics affect the human BHC.
One of the aims of this study was to find out whether people in the overweight sample differ in their BHC. For this purpose, individuals from
two ethnic groups (Kyrgyz and Russians) with alimentary obesity were studied. All methods of estimating BHC were used and all of them gave comparable results. It turned out that samples of overweight women, regardless of their racial and ethnic characteristics, did not differ significantly in any of the methods of human BHC assessment (these data are not presented here), which allowed us to combine them into one group for further analysis. However, individuals with alimentary obesity differed significantly from controls, Kyrgyz and Russian women of normal weight (Tables 9 and 10). They are characterized by low values and a narrow range of variability of BHC compared to controls.
________________________________________________
Control Temperature
of palm Obesity Kyrgyz Russians
(in ⁰С) (n = 100) (n = 30) (n = 30)
1 2 3
29 22 2
30 36 1 2
31 17 8 6
32 15 10 9
33 9 9 9
34 1 2 2
_________________________________________________
Total 3056 963 957
Mean
number 30.56 ± 0.129; 32.10 ± 0.182; 31.90 ± 0.237;
t 1,2 = 6.019; df = 128; P = <0>
t 2,3 = 0.671; df = 58; P = <0>
t 1,3 = 4.986; df = 128; P = <0>
Table 9. The distribution of the temperature (in °C) of the palm of the hands in women with alimentary obesity and in the control sample, taking into account their ethnic origin.
_________________________________________________
Obesity Control
Temperature ____________________________________
difference Kyrgyz Russian
(in °С) (n = 100) (n = 30) (n = 30)
1 2 3
_________________________________________________
2 2 2
3 12 9 9
4 13 12 10
5 18 6 5
6 39 1 2
7 18 2
___________________________________________________
Всего 538 115 122
Средне число 5.38 ± 0.126; 3.83 ± 0.173; 4.07 = 0.235;
t 1,2 = 6.202; df = 128; P = <0>
t 2,3 = 0.800; df = 58; P = <0>
t 1,3 = 4.980; df = 128; P = <0>
Table 10. The distribution of the temperature difference (in ºС) between the palm and armpit in women with alimentary obesity and in the control sample, taking into account their ethnic origin.
As can be seen from Tables 9-10, women with alimentary obesity significantly differ from the control according to all the BHC assessments.
The study of a sample of alcoholics and drug addicts of Kyrgyz and Russian ethnicity showed that regardless of their racial and ethnic characteristics, the BHC levels estimated by the methods used for a sample of individuals with alimentary obesity differ significantly from the control: alcoholics are characterized by extremely low, whereas drug addicts are characterized by very high BHC (these data are not presented here). We will specifically return to this issue below when we analyze the relationship between the level of BHC and the number of chromosomal HRs in the human genome.
Chromosomal heterochromatin regions, condensed chromatin, cell thermoregulation and body heat conductivity.
We believe that cell thermoregulation underlies the variability of human BHC. Without direct experimental evidence, we have nevertheless hypothesized that the layer of condensed chromatin (CC) around the cell nucleus of higher eukaryotes is associated with intracellular physical thermoregulation. The CC, being the most densely packed material, should have the highest thermal conductivity in the interphase cell, since it consists of chromosomal HRs, which represent the higher form of organization of noncoding DNA [11,13,15].
It is assumed that any scientific hypothesis can be objectively tested experimentally, using direct or indirect methods. Before discussing this part of the problem, it seems necessary to clarify some of the concepts that we used in the presentation and verification of our hypothesis. There are two such concepts: density and heat conductivity. No one seriously doubts that they may have some significance in wildlife, although these physical concepts are used extremely rarely in the biomedical literature. We use them not as metaphors, but as fundamental physical quantities, that is, in their original sense: a) density, a physical quantity defined for a homogeneous substance by its mass per unit volume; b) heat conductivity is the transfer of heat from one body or object to another when their surfaces touch. This process takes place without the transition of matter from one surface to another, i.e. thermal energy is transferred with the help of micro particles.
From our point of view, the thickness of the CC layer around the cell nucleus depends on the number of chromosomal C-HRs in the genome. However, as we believe, the packing density (compactization) of CC is possibly associated with the number of chromosomal Q-HRs. The fact is that human populations do not differ significantly from each other in the number of chromosomal C-HRs in the genome [17,18]. Wide quantitative variability at the population level was found only in the chromosomal Q-HRs. In addition, it has been established that quantitative patterns in the distribution of chromosomal Q-HRs in the population depending on gender, age, racial and ethnic origin and the characteristics of the place of permanent residence of humans [7,19-36]. It is noteworthy that these patterns turned out to be very similar to the pattern of wide variability of human BHC in the population.
If our hypothesis is correct, then the differences of people among themselves in BHC should be a consequence of the known wide quantitative variability of chromosomal Q-HRs in the genome of the human population. In other words, there should be a direct relationship between the number of chromosomal Q-HRs in the genome and the level of human BHC. The results confirming this assumption are given below.
Table 11 shows the relationship between the number of chromosomal Q-HRs in the human genome and the rate of reaction of the body to the controlled thermal load, which was determined by the time (in minutes) to the occurrence of peak temperature on the surface of the right palm.

Table 11. The numbers of chromosomal Q-HRs and time to occurrence of temperature peak on the surface of the right palm.
*These differences are statistically significant.
As can be seen in this Table, there is a statistically significant relationship between the number of chromosomal Q-HRs in the human genome and the reaction of the body to the controlled thermal load. In individuals whose genome contains more chromosomal Q-HRs than the population average, the peak temperature occurs in the first five minutes of the thermal load, and vice versa. The relationship between the quantity of chromosomal Q-HRs and the temperature difference between the surface of the right palm and the left armpit at rest is shown in Table 12.
Numer of Q-HRs | The temperature difference between the palm and the armpit. | ||
0.1 °C to 1.0 °C (n = 32) I | 1.0 °C to 2.0 °C (n = 71) II | 2.1 °C to 3.0 °C (n = 33) III | |
| 2 | 10 | 9 | |
| 3 | 12 | 11 | |
| 4 | 9 | 26 | 7 |
| 5 | 9 | 14 | 12 |
| 6 | 7 | 4 | 1 |
| 7 | 5 | 3 | 2 |
| 8 | 2 | 2 | 1 |
| Total Q-HRs | 174 | 291 | 117 |
| Mean number of Q-HRs | 5.44 ± 0.220 | 4.10 ± 0.168 | 3.54 ± 0.275 |
| Statistics | t I, II = 4.607; df = 101; P = <0> t II, III = 1.786; df = 102; P = 0.077; t I, III = 5.349; df = 63; P = <0> | ||
*These differences are statistically significan
Table 12. The numbers of chromosomal Q-HRs and the temperature difference between the surface of the right palm and the left armpit.
As can be seen in Table 12 the more chromosomal Q-HRs in the human genome, the smaller the temperature difference between the left armpit and the surface of the right palm, and vice versa. Table 13 demonstrates the relationship between the number of chromosomal Q-HRs in the human genome and palm surface temperature.
Number of Q-HRs | The temperature of the surface of the rightpalm. | ||
Below 35.0 °С (n = 36) I | 35.1 °С to 36.0 °С (n= 74) II | 36.1 °С and over (n = 26) III | |
| 2 | 5 | 14 | |
| 3 | 6 | 17 | |
| 4 | 16 | 23 | 3 |
| 5 | 7 | 7 | 11 |
| 6 | 2 | 5 | 5 |
| 7 | 6 | 4 | |
| 8 | 2 | 3 | |
| Total Q-HRs | 139 | 284 | 149 |
| Mean number of Q-HRs | 3.86 ±0.179 | 3.97 ±0.185 | 5.73 ±0.239 |
| Statistics | t I,II = 0.380; df= 108; P = 0.704; t II,III = 5.111; df = 98; P = <0> t I,III = 6.395; df= 60; P = <0> | ||
*These differences are statistically significant.
Table 13. The number of chromosomal Q-HRs and the temperature of the surfaceof the right palm.
As can be seen in Table 12 the more chromosomal Q-HRs in the human genome, the smaller the temperature difference between the left armpit and the surface of the right palm, and vice versa. Table 13 demonstrates the relationship between the number of chromosomal Q-HRs in the human genome and palm surface temperature.
Number of Q-HRs | The temperature of the surface of the rightpalm. | ||
Below 35.0 °С (n = 36) I | 35.1 °С to 36.0 °С (n= 74) II | 36.1 °С and over (n = 26) III | |
| 2 | 5 | 14 | |
| 3 | 6 | 17 | |
| 4 | 16 | 23 | 3 |
| 5 | 7 | 7 | 11 |
| 6 | 2 | 5 | 5 |
| 7 | 6 | 4 | |
| 8 | 2 | 3 | |
| Total Q-HRs | 139 | 284 | 149 |
| Mean number of Q-HRs | 3.86 ±0.179 | 3.97 ±0.185 | 5.73 ±0.239 |
| Statistics | t I,II = 0.380; df= 108; P = 0.704; t II,III = 5.111; df = 98; P = <0> t I,III = 6.395; df= 60; P = <0> | ||
*These differences are statistically significant.
Table 13. The number of chromosomal Q-HRs and the temperature of the surfaceof the right palm.
How do we interpret these data? We believe that the time to occurrence of peak temperature on the right palm reflects the rate of heat conductivity, while the value of temperature of the right palm’s surface at that moment seems to reflect the quantity of thermal energy in the individual’s body. If the peak temperature on the surface of the palm occurs in the first five minutes after the thermal load is applied, then such an individual is considered to have a high BHC, and vice versa. In other words, we believe that a person with a high BHC conducts heat through the body quicker and eliminates any excessive through the body shell quicker to better maintain inner body temperature at a constant level.
A statistically significant relationship between the number of chromosomal Q-HRs in the genome and the temperature difference between the left armpit and the right palm at rest may also characterize the heat conducting ability of the human body — the smaller the temperature difference, the higher the BHC, and vice versa. We believe that a smaller temperature difference between the armpit and the palm reflects the high heat conductivity of the body, so that such an organism equalizes the temperature difference between the different parts of the body more effectively, thereby successfully avoiding overheating in high temperature conditions. The temperature of the right palm at rest, presumably, also reflects the level of BHC: individuals with a high temperature at the palm may have higher BHC, and vice versa.
Taken together, our results show that, at the population level: a) BHC is higher on average in males than in females; b) individuals from different age groups differ in BHC, on average, its level in people steadily decreases with age; c) the indigenous inhabitants of the low mountains and low latitudes have a higher BHC on average than the inhabitants of the high altitudes and high latitudes. It is noteworthy that these results are consistent with the data obtained in the study of the quantitative content of chromosomal Q-HRs in the genome, namely: a) at the population level, the number of chromosomal Q-HRs in the male karyotype is usually greater than that of female; b) the number of chromosomal Q-HRs in different age groups is different, most of the Q-heterochromatin material is found in the genome of newborns, and the smallest amount is found in the elderly [13,22,41,42] and c) the largest number of Q-HRs is found in the genome of populations living permanently at low geographical latitudes, the smallest number is found in the indigenous inhabitants of the Far North and high altitudes, and the inhabitants of temperate climatic zones occupy an intermediate position in this regard [7,11,13].
In any case, our data support the assumption that: (1) apparently, the level of human BHC depends on the density of the peripheral CC layer in the interphase nucleus, in the compaction of which the amount of Q-HRs in its genome plays an important role; (2) the bodies of individuals in a population differ significantly from each other, among other things, in heat conductivity; (3) organ-based physiological thermoregulation is the same, in general, is realized under different physical conditions in all normal people due to the fact that individuals in the population differ in BHC [11,13,16].
Basically, we want to assert that, a) the smaller the temperature difference between different parts of the body, the higher the BHC for a given individual, and vice versa;
b) individuals with a high BHC equalize better and faster temperature differences between different parts of the body, and vice versa. If that is the case, then, for example, the well-known resistance of the indigenous inhabitants of the southern latitudes to high ambient temperatures would find a rational explanation. And namely, southerners, due to the high heat conductivity of their bodies, more effectively equalize temperature differences in different parts of the body and quickly remove (dissipate) excess heat into the environment. In this case, the natives of the Far North and highlands can better and longer retain metabolic heat in the body due to the low heat conductivity of their bodies, with all the ensuing consequences for their adaptation. In the same way, it would be possible to explain why men tolerate heat stress better than women, and the latter are more resistant to cold than men (for more details, see) [13].
We have studied Kyrgyz and Russian women of reproductive age to assess the possible role of the number of chromosomal Q-HRs in the genome in the predisposition of alimentary obesity. All studied individuals are residents of Bishkek, the capital of Kyrgyzstan. Our sample included women whose weight exceeded 20% or more of the norm, and, according to external clinical signs, was diagnosed as an alimentary form of obesity (see above). Phenotypically Kyrgyz and Russian healthy women of reproductive age with normal weight were taken as controls. Table 14 presents data on the distribution of numbers and the mean number of Q-HRs per individual in the surveyed samples.
| Number of Q-HRs | Obese females | Controls | ||
Kyrghyz (N = 56) | Russians (N = 44) | Kyrghyz (N = 100) | Russians (N = 100 | |
| I | II | III | IV | |
| 0 | 11 (19.6) | 5 (11.4) | 2 (2.0) | 4 (4.0) |
| 1 | 24 (42.9) | 18 (40.9) | 11 (11.0) | 7 (7.0) |
| 2 | 19 (33.9) | 19 (43.2) | 32 (32.0) | 24 (24.0) |
| 3 | 2 (3.6) | 2 (4.5) | 19 (19.0) | 33 (33.0) |
| 4 | 22 (22.0) | 31 (31.0) | ||
| 5 | 11 (11.0) | 1 (1.0) | ||
| 6 | 2 (2.0) | |||
| 7 | 1 (1.0) | |||
| Total number of Q-HRs |
68 |
62 |
294 |
283 |
| Statistics | χ21,2 = 1.69 χ21, 3 = 1.55 χ21,4 = 4.15 χ22,3 = 1.78 χ22,4 = 8.74 χ23,4 = 14.18 | |||
| df = 2 df = 2 df = 2 df = 2 df = 2 df =2 | ||||
| P > 0.50 P < 0> 0.95 | ||||
| Mean number of Q-HRs |
1.21 ± 0.11 |
1.41 ± 0.11 |
2.94 ± 0.14 |
2.83 ± 0.11 |
| t1,2 = 1.29 t1,3 = 9.72 t1,4 = 10.41 t2,3 = 8.59 t2,4 =9.13 t3,4 = 0.62 | ||||
| df = 99 df = 156 df = 144 df = 140 df = 123 df = 189 | ||||
| P > 0.20 P < 0> 0.50 | ||||
Table 14. The number of chromosomal Q-HRs per individual in groups of obese women and in control samples.
As can be seen from this table, obese women, regardless of their ethnic origin, are characterized by a significantly low mean number and a narrow range of variability in the distribution of numbers of Q-HRs in samples, compared with controls We also studied samples of alcoholics and drug addicts of Kyrgyz and Russian ethnicity to assess the possible role of the number of chromosomal Q-HRs in the genome in the development of these purely human forms of pathologies. Phenotypically Kyrgyz and Russian healthy индивидов were taken as controls. Table 15 presents data on the distribution of numbers and the mean number of Q-HRs per individual in the surveyed samples.
Number of Q-HRs | Alcoholics | Drug addicts | Controls | ||
Kyrghyz (n = 48) | Russians (n = 57) | Mixed (n = 100)
| Kyrghyz (n = 202) | Russians (n = 556) | |
| I | II | III | IV | V | |
| 0 | 7 (14.5) | 10 (17.5) | 18 (8.9) | 46 (8.3) | |
| 1 | 23 (47.9) | 17 (29.8) | 37 (18.3) | 119 (21.4) | |
| 2 | 12 (25.0) | 22 (38.5) | 12 (12.0) | 72 (35.6) | 194 (34.9) |
| 3 | 6 (12.5) | 6 (10.5) | 13 (13.0) | 35 (17.3) | 122 (21.9) |
| 4 | 2 (3.5) | 36 (36.0) | 29 (14.4) | 57 (10.2) | |
| 5 | 30 (30.0) | 9 (4.5) | 16 (2.9) | ||
| 6 | 9 (9.0) | 2 (1.0) | 2 (0.4) | ||
| Total number of Q-HRs | 65 | 87 | 411 | 459 | 1193 |
| c2I, II = 2.40 | c2I, III = 78.39 | c2I, IV = 21.50 | c2I, Y = 21,78 | c2II, III = 57.21 | |
| df = 1 | df = 1 | df = 1 | df = 1 | df = 1 | |
| P > 0.50 | P < 0> | P < 0> | P < 0> | P < 0> | |
| c2II, IV = 8.34 | c2II, V = 7.52 | c2III, IY = 33.29 | c2III, Y = 39.65 | c2IY,Y = 0.43 | |
| df = 1 | df = 1 | df = 1 | df = 1 | df = 1 | |
| P < 0> | P < 0> | P < 0> | P < 0> | P > 0.05 | |
| Mean number of Q-HRs | 1.35 ± 0.128 | 1.53 ± 0.135 | 4.11 ± 0.113 | 2.27 ± 0.094 | 2.15 ± 0.51 |
| tI, II = 0,96 | t I, III = 16.17 | t I, IV = 5.79 | t I,V = 5.81 | t II, III = 14.66 | |
| df = 103 | df = 118 | df = 106 | df =64 | df = 112 | |
| P > 0.300 | P < 0> | P < 0> | P < 0> | P < 0> | |
| t II, IV = 4.50 | t II, V = 3.76 | t III, IV = 12.52 | t III, V = 15.81 | t IV, V = 1.12 | |
| df = 118 | df = 611 | df = 232 | df = 143 | df = 328 | |
| P <0> | P < 0> | P < 0> | P < 0> | P > 0.200 | |
Table 15. The number of Q-HRs per individual in alcoholics, drug addicts and controls.
First of all, we note that the relevant statistical analysis showed the following׃ patients suffering from alcoholism and representing two different ethnic groups did not differ significantly in all the studied quantitative characteristics of the variability of chromosomal Q-HRs, which made it possible to combine them into one group. According to the table, alcoholics have the lowest average number of Q-HRs per individual in populations and the narrowest range of variability in the number of chromosomal Q-HRs among all the samples studied by us. While persons suffering from drug abuse had the highest value, nevertheless, it should be noted that the range of variability in the number of chromosomal Q-HRs is as narrow as in alcoholics, however, individuals with large numbers of Q-HRs in the genome prevailed.
As noted above, the sample of drug addicts we studied could not be divided by their ethnic origin, due to their small number for adequate statistical analysis, and therefore we limited ourselves only to indicating their quantities. One way or another, according to our data, the content of chromosomal Q-HRs in the genome of drug addicts, compared with the control, and in particular, with patients suffering from alcohol abuse, was significantly higher.
The following results from our data are noteworthy: 1) patients with alcoholism have the lowest quantity of Q-HRs in the genome, and they do not differ from each other in all quantitative characteristics of the variability of chromosomal Q-HRs, despite their ethnic origin; 2) drug addicts have significantly more Q-HRs in the genome, compared with the control and, in particular, with persons suffering from the abuse of hard liquor [37,38].
It can now be considered established that individuals in a population differ from each other in terms of BHC. The level of human BHC can be determined by different methods that differ in complexity and execution time, but give comparable results. The fastest method of estimating human BHC is the surface temperature of the palm. Human BHC can also be estimated by the temperature difference between different parts of the body (e.g., armpit and palm) or by the timing of the temperature peak on the palm under controlled temperature loading (calorimetry). The most complex and in-depth is the assessment of human BHC by the number of chromosomal Q-HRs in the karyotype. Unfortunately, none of the above methods allow to estimate the level of BHC in absolute figures, as heat physicists have in relation to metals. The maximum that can be counted on is to estimate the level of heat conductivity of a given individual as high, medium or low.
Now, based on the above data, we will briefly consider the situation with alimentary obesity. We found that individuals suffering from alimentary obesity have a significantly lower BHC compared to the control sample. This circumstance, we believe, confirms the previously stated assumption about a possible relationship between the BHC level and the number of chromosomal Q-HRs in the human genome [16].
The main question remains open – why are some individuals thin and others fat even in a relatively homogeneous environment? It is believed that the answer to this question will be obtained by identifying the genes responsible for obesity in humans, and the leptin hormone is considered a key element of this system. We share only partially such “molecular genetic optimism”. The fact is that there are a number of circumstances that directly or indirectly indicate the limitations of exclusively molecular research approaches, including the search for a hypothetical structural gene (or genes) in the development of alimentary obesity in humans.
For example: 1) the results of numerous epidemiological studies conducted in many countries and regions have clearly shown that women are obese twice as often as men; 2) obesity, as a global medical and social problem, has arisen only in recent decades, and it seems very doubtful for us that there are violations of the functioning of the neuroendocrine and central nervous systems in maintaining energy homeostasis in a modern human, only due to improved living conditions and nutrition, despite the fact that the corresponding homeostatic systems have been operating in Nature for a long time. Moreover, our body is better equipped to deal with weight loss than with excess weight, since throughout history, a human has lived in conditions of food shortage; 3) in the evolution of the Homo sapiens species, there has never been such a period of “prosperity” as in the current economically developed countries, so that serious micro evolutionary changes occurred in its genome that could cause the emergence of a specific structural obesity gene, and therefore the increase in the frequency of alimentary obesity is difficult to explain solely by the appearance of new genes in the gene pool of modern human. In connection with the above data, we believe that there may be other hereditary factors besides structural genes that predispose to the occurrence of alimentary obesity in humans.
With respect to obesity, we believe the following: in patients with alimentary obesity, respectively, with a low content of Q-HRs in the genome, under favorable living conditions (temperature comfort) and material standard of living, part of the calories in a low heat-conducting body accumulates in the form of body fat due to poor removal (dissipation) of excess metabolic heat from the body.
We would answer the notorious question: “Why are some individuals thin and others very fat?” - instead of existing points of view that believe that obesity is the result of a lack of internal discipline in food ingestion, or the presence in the genome of structural genes responsible for obesity in humans, that obesity is not just a personal failure or the result of a malfunction of any structural genes (here we mean only alimentary obesity). We believe that, apparently, there is a very wide diversity in the human population in the functioning of energy and temperature homeostasis, and this diversity is associated with the BHC level of the individual. In individuals with low BHC, even when consuming the same amount of food as people with normal weight, under comfortable living conditions, more fat will be deposited due to a smaller number of chromosomal Q-HRs, which, as we believe, are involved in human thermoregulation as part of CC in the cell nucleus [11,12,15].
Alcoholism and drug addiction are exclusively human pathologies. The pathogenesis of these diseases has not been fully elucidated despite the obvious etiology. Our data presented above show that the number of chromosomal Q-HRs in the genome seems to have something to do with the pathogenesis of alcoholism and drug addiction. As we have already shown, in the genome of individuals who abuse strong alcoholic beverages, the number of chromosomal Q-HRs is extremely small, while at the same time, people with drug addiction, on the contrary, have a lot of Q-HRs (see above).
The possible role of BHC in the development of alcoholism and drug addiction appears to us as follows; the frequency of consuming strong alcoholic beverages tends to increase with increasing latitude (from low to high) and altitude. At the same time, the number of Q-HRs in the genome in a population tends to decrease as the geographical latitude increases and the height of the place of permanent residence above sea level increases [7,11,13,39].
Let’s consider the simplest example. Often life and the harsh climate in the Far North or the high-altitudes predispose, in a certain sense, to the intake of strong alcoholic beverages just to obtain a feeling of thermal comfort. But at the same time, as we believe, the same dose of alcohol for people with different BHC can lead to different consequences. So, a feeling of thermal comfort in individuals with low BHC occurs after in taking a relatively large amount of alcohol in one feast due to delayed “warming up” and equalization of the temperature difference in different parts of the body, which eventually leads to more severe intoxication with a hangover syndrome than in individuals with normal or high BHC. In other words, the lower the BHC of an individual, the more strong alcohol is required due to the slow warming of the whole body necessary for the onset of a feeling of thermal comfort in the whole body.
Addiction to drugs in drug addicts, that is, individuals with high BHC (due to the high content of Q-HRs in the genome) also occurs due to the desire to get a sense of thermal comfort., but this “pleasure” specifically comes from the “narcotic cooling” of the body, with the resulting emotional or other sufferings. We believe that the psycho-emotional effects of alcohol and drugs on the body are determined by the depth of violation of temperature homeostasis at the cellular level, but manifested in diametrically opposite directions, that is, ethanol causes alcohol intoxication, raising body temperature (the oxidation of 1 g of ethanol produces 7 kcal), and drugs, on the contrary, lower it, causing a state of narcotic stupor.
The natural human desire in a hot climate to enjoy the “deep coolness” or thermal comfort in the North or the highlands would be a completely justified desire if they were not satisfied with narcotic stupor or alcohol intoxication. However, the notorious propensity of southerners to take drugs, and northerners or highlanders to strong alcoholic beverages, could be partly explained by the different content of Q-HRs in their genome [23,26,27,31-33] and, accordingly, associate them with the human BHC [13,37,38].
As we know, people differ from each other in skin color, eye shape, hair texture, height, body build (constitution) and many other external anatomical features. All of them are the result of long evolution (adaptation) of a human being to the environment of permanent residence. Most of these constitutional traits do not significantly affect a person's daily life, except for some cultural biases related to skin color, eye shape or hair texture. Human BHC, although not visible, is as constitutional traits as the above-mentioned anatomical features because it does not change during individual development (ontogeny). However, there is still one essential difference between these human constitutional features: it is desirable for a person to know and understand the level of his/her BHC when it concerns health, choice of profession and sport.
The reason is simple: a) in norm people do not differ significantly in the mechanisms of organ-based (hypothalamus) physiological thermoregulation; b) the differences of people lie in the fact that thermoregulation at the level of the organism is carried out in the body with different heat conductivity. In this sense, we have encountered a problem alien for classical courses of normal physiology.
Speaking about human health and choice of profession, we mean, first, the resistance of a given body to cold or heat. The role of BHC is particularly important when choosing a sport: it is hardly advisable for an individual with a low BHC to engage in a sport that requires efficient removal of excess metabolic heat outside the body (marathon running, professional soccer or boxing). On the other hand, it is dangerous for a person with a high BHC to engage in water and winter sports or mountaineering because of the risk of rapid body cooling [43]. The important role of BHC in predisposing a person to the development of obesity, alcoholism and drug abuse has already been discussed in detail above (for details see) [14,37,38,40].
Finally, the answer to the question why only humans differ from each other by BHC is known. The point is that among the three species of higher primates (Homo sapiens, Pan troglodytes and Gorilla gorilla), which have Q-HRs in their genome in addition to chromosomal C-HRs, only human populations are differ by a wide quantitative variability of Q-heterochromatin materials: from complete absence to ten Q-HRs in an individual. In chimpanzee and gorilla populations, individuals practically do not differ in the number of chromosomal Q-HRs. The reason for this circumstance lies in the peculiarity of the distribution of Q-HRs on the chromosomes of man and the two great apes. In the human karyotype, chromosomal Q-HRs are distributed on seven pairs of Q-polymorphic autosomes (3, 4, 13-15, 21 and 22) with different frequencies, which allows the birth of children with different amounts of Q-heterochromatin. In chimpanzees and gorillas chromosomal Q-HRs are present on five and seven pairs of autosomes (respectively) and they are evenly distributed, which does not allow the birth of offspring with different amounts of Q-heterochromatin materials in the genome. Therefore, only humans can differ in BHC, which allowed them to eventually master all climatogeographic regions of the Earth [13,44,45].
Acknowledgments. I apologize to those authors, whose works were not cited, or were cited only through reviews, owing to space limitations.
Conflicts of interest: none.
Funding has not been received for the study.
Statement of Consent/Ethical approval: Not required.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
