
Research article | DOI: https://doi.org/10.31579/2639-4162/052
1Akdeniz University, Faculty of Medicine, Department of Family Medicine, Antalya /Turkey.
2Akdeniz University, Faculty of Medicine, Department of Sports Medicine, Antalya /Turkey.
*Corresponding Author: Melahat Akdeniz, Akdeniz University, Faculty of Medicine, Department of Family Medicine, Antalya / Turkey.
Citation: Elif Duman Acar, Melahat Akdeniz, Ethem Kavukcu, Esma Eseroglu, Hasan Hüseyin Avcı, (2021) The Health of Companions: Evaluatıon of Care Burden, Psychologıcal Dıstress and Psychıatrıc Dısorders of the Companıons of Patıents ın the Medıcal Ward of Akdenız Unıversıty Hospıtal. J. General medicine and Clinical Practice, 4(1); Doi:10.31579/2639-4162/052
Copyright: © 2021 Melahat Akdeniz, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 February 2021 | Accepted: 11 June 2021 | Published: 16 June 2021
Keywords: companion; caregiver; zarit caregiver burden scale; brief symptom ınventory; hospitalized patients
Objective: The aim of this study was to evaluate the care burden, psychological distress and psychiatric disorders of the companions of adult patients in the hospital.
Method: This study is a cross-sectional descriptive study. A study questionnaire that included a sociodemographic information form, the Zarit Caregiver Burden Scale (ZCBS) and the Brief Symptom Inventory (BSI) were administered to the companions. Simple descriptive and inferential statistics were performed. The Mann-Whitney U test was used if comparisons between two independent groups were normal. Correlation coefficients and statistical significance were calculated by using the Spearman test for at least one normal nondistributed relationship. A multiple linear regression analysis was performed for determining factors associated with BSI scores. The type 1 error level was used as 5% for statistical significance. All P values of less than 0.05 were considered significant.
Results: Three hundred companions were included in the study. Emotional commitment was the leading cause of companionship. The mean values of the companions’ ZCBS and BSI scores were 20.2 and 34.4, respectively. There was a moderately positive correlation (r=0.502) between the ZCBS and BSI scores, and it was statistically significant. ZCBS score were positively associated with BSI score.
Conclusion: Psychological distress increases as the care burden of companions increases. Companions need more assistance from health care institutions, family members and the community. The support of health workers and family members reduced the companions’ care burden and psychological distress. Physicians working in the hospital should take into account that companions may be hidden patients.
The illness of a family member affects other members of the family, changes family relationships and alters family life. If the disease is acute and curable, the effect on the family is minor and temporary. If serious, long-term chronic diseases and disability are present, problems arise in the care of the patient. To provide proper care for the sick family member at home or in the hospital environment, the roles within the family must be rearranged, and the routine lifestyle of the family changes. [1,2]
Family members play a major role in caring for a sick family member with a chronic illness. The physical, emotional and economic difficulties experienced by the family members who provide care to the sick person adversely affect their quality of life. These difficulties faced by caregivers are called care burden. [1,3]
Caregiver burden has been defined by George and Gwyther (1986) as ‘the physical, psychological or emotional, social, and financial problems that can be experienced by family members caring for impaired older adults”. [4] "Zarit et al. also defined caregiver burden: “The extent to which caregivers perceive that caregiving has had an adverse effect on their emotional, social, financial, physical, and spiritual functioning.” [5] Although Caregiver burden is an important health problem, there is no International Classification of Diseases, Ninth Revision (ICD-9) or ICD-10 code for caregiver burden.
The family member who is exposed to care burden may experience physical, psychological, emotional, and functional health problems. In family-oriented primary care, these people are defined as “hidden patients”. [2] In any family in which there is an individual with an acute and life-threatening or chronic and long-term illness or diseases, the caregiver is under considerable stress. If this caregiver is not getting enough support from other family members, mechanisms for coping stress may fail and the caregiver may develop obvious or hidden signs of illness. For this reason, it is important for physicians to evaluate the health status of caregivers as well as patients. [2]
Most of the studies on care burden and quality of life of family members have been conducted on the problems and needs of people who provide home care for people with chronic diseases or who have limitations in daily life activities. [6,8]
Culturally, in some countries, such as Turkey, where there is a high tendency not to leave hospitalized family members alone, there is usually a family member who stays with the hospitalized patients, supporting and taking care of them. In Turkey, these people who are known as “refakatçi” (the patient's companion) could be spouses, children, close relatives, friends or neighbors who provide important assistance to hospitalized persons. The companions assist the care of their relatives or friends in the fields of personal hygiene, nutrition, going to the toilet, bathing and taking oral medication. [9-13]
During care giving of the hospitalized patients, companions often find themselves isolated from society. They have very little time to maintain social contacts with people. As companions spend a considerable amount of time in the hospital, their own care needs also arise. Furthermore, even if voluntarily performed, being detached from private life, having to leave individual’s home and workplace, and dealing with the severity of the disease of the patient who receives care creates a care burden on the companions. The companions are vulnerable to physical and psychological conditions and, their quality of life is negatively affected. [9,11]
Currently, the number of studies examining hospital companions is very limited. Moreover, the health status of companions has not been investigated in these studies. Some of the existing studies on the caregivers of hospitalized relatives were conducted in Greece, where family members stay with patients for long periods of time and provide in-hospital informal care. [13-17] However, in these studies, care burden and health status of informal caregivers were not evaluated.
Bellou-Milona et al. [14] investigated health personnel's attitudes towards the participation of family members in patient care, health education, the need for information and emotional support of companions. Stavrianou et al. [13] investigated the role of informal caregivers during hospitalization of a family member, factors affecting their presence and patient's needs. Sapountzi Krepia et al. [16,17] in 2 separate studies investigated the kind and frequency of care provided to hospitalized cancer patients by relatives and the reasons for providing this care, as well as the type and frequency of care-giving activities provided by family members in the rehabilitation setting. Lavdaniti et al. [15] compared the perceptions of the nurses and the inhospital informal caregivers about the patient care.
A study conducted in Israel by Rothman et al. [18]investigated how nurses, patients and family members evaluated the participation of family members in the care of the patient. Islam et al. [19] examined whether companions were at risk for hospital-acquired resistant infections was investigated on companions in a tertiary hospital in Pakistan. In a study conducted by Sadigh et al. [20] in Uganda, companions’ demographic data, difficulties faced and the effects of these difficulties on patient care were investigated; however, their health status and care burden were not investigated. In Brazil, in a qualitative study conducted by Passos et al. [12] investigated the changes in the routine of the family companion during the hospitalization of a family member.
There are studies related to companions in Turkey. A study by Sarıtaş et al. [21] investigated the burden of care for the companions of patients who were hospitalized in the oncology service. Akpinar et al. [9]identified and described the concept of the patients' companions from the perspectives of the companions and evaluated the concept of the patient's companion in terms of biomedical ethics. Celik et al. [22] investigated the roles, expectations and problems of patient companions.
In the mentioned studies, however the health status of the companions was not evaluated, which may have significant effect on care burden. It is known that care burden on the caregiver affects his/her physical, mental and social health, and cultural characteristics will change the caregiver/companion’s perception of care burden. [7,9].
In Turkey, there is a companion present for the majority of hospitalized adult and pediatric patients. Awareness of the companion's care burden and the possible effects of this burden on his/her health can be a guide to protecting and improving their health. Hence in this study, we aimed to evaluate the care burden, psychological distress and psychiatric disorders of companions of adult patients who were hospitalized in the medical ward of XXX University Hospital.
The illness of a family member affects other members of the family, changes family relationships and alters family life. If the disease is acute and curable, the effect on the family is minor and temporary. If serious, long-term chronic diseases and disability are present, problems arise in the care of the patient. To provide proper care for the sick family member at home or in the hospital environment, the roles within the family must be rearranged, and the routine lifestyle of the family changes. [1,2]
Family members play a major role in caring for a sick family member with a chronic illness. The physical, emotional and economic difficulties experienced by the family members who provide care to the sick person adversely affect their quality of life. These difficulties faced by caregivers are called care burden. [1,3]
Caregiver burden has been defined by George and Gwyther (1986) as ‘the physical, psychological or emotional, social, and financial problems that can be experienced by family members caring for impaired older adults”. [4] "Zarit et al. also defined caregiver burden: “The extent to which caregivers perceive that caregiving has had an adverse effect on their emotional, social, financial, physical, and spiritual functioning.” [5] Although Caregiver burden is an important health problem, there is no International Classification of Diseases, Ninth Revision (ICD-9) or ICD-10 code for caregiver burden.
The family member who is exposed to care burden may experience physical, psychological, emotional, and functional health problems. In family-oriented primary care, these people are defined as “hidden patients”. [2] In any family in which there is an individual with an acute and life-threatening or chronic and long-term illness or diseases, the caregiver is under considerable stress. If this caregiver is not getting enough support from other family members, mechanisms for coping stress may fail and the caregiver may develop obvious or hidden signs of illness. For this reason, it is important for physicians to evaluate the health status of caregivers as well as patients. [2]
Most of the studies on care burden and quality of life of family members have been conducted on the problems and needs of people who provide home care for people with chronic diseases or who have limitations in daily life activities. [6,8]
Culturally, in some countries, such as Turkey, where there is a high tendency not to leave hospitalized family members alone, there is usually a family member who stays with the hospitalized patients, supporting and taking care of them. In Turkey, these people who are known as “refakatçi” (the patient's companion) could be spouses, children, close relatives, friends or neighbors who provide important assistance to hospitalized persons. The companions assist the care of their relatives or friends in the fields of personal hygiene, nutrition, going to the toilet, bathing and taking oral medication. [9-13]
During care giving of the hospitalized patients, companions often find themselves isolated from society. They have very little time to maintain social contacts with people. As companions spend a considerable amount of time in the hospital, their own care needs also arise. Furthermore, even if voluntarily performed, being detached from private life, having to leave individual’s home and workplace, and dealing with the severity of the disease of the patient who receives care creates a care burden on the companions. The companions are vulnerable to physical and psychological conditions and, their quality of life is negatively affected. [9,11]
Currently, the number of studies examining hospital companions is very limited. Moreover, the health status of companions has not been investigated in these studies. Some of the existing studies on the caregivers of hospitalized relatives were conducted in Greece, where family members stay with patients for long periods of time and provide in-hospital informal care. [13-17] However, in these studies, care burden and health status of informal caregivers were not evaluated.
Bellou-Milona et al. [14] investigated health personnel's attitudes towards the participation of family members in patient care, health education, the need for information and emotional support of companions. Stavrianou et al. [13] investigated the role of informal caregivers during hospitalization of a family member, factors affecting their presence and patient's needs. Sapountzi Krepia et al. [16,17] in 2 separate studies investigated the kind and frequency of care provided to hospitalized cancer patients by relatives and the reasons for providing this care, as well as the type and frequency of care-giving activities provided by family members in the rehabilitation setting. Lavdaniti et al. [15] compared the perceptions of the nurses and the inhospital informal caregivers about the patient care.
A study conducted in Israel by Rothman et al. [18]investigated how nurses, patients and family members evaluated the participation of family members in the care of the patient. Islam et al. [19] examined whether companions were at risk for hospital-acquired resistant infections was investigated on companions in a tertiary hospital in Pakistan. In a study conducted by Sadigh et al. [20] in Uganda, companions’ demographic data, difficulties faced and the effects of these difficulties on patient care were investigated; however, their health status and care burden were not investigated. In Brazil, in a qualitative study conducted by Passos et al. [12] investigated the changes in the routine of the family companion during the hospitalization of a family member.
There are studies related to companions in Turkey. A study by Sarıtaş et al. [21] investigated the burden of care for the companions of patients who were hospitalized in the oncology service. Akpinar et al. [9]identified and described the concept of the patients' companions from the perspectives of the companions and evaluated the concept of the patient's companion in terms of biomedical ethics. Celik et al. [22] investigated the roles, expectations and problems of patient companions.
In the mentioned studies, however the health status of the companions was not evaluated, which may have significant effect on care burden. It is known that care burden on the caregiver affects his/her physical, mental and social health, and cultural characteristics will change the caregiver/companion’s perception of care burden. [7,9].
In Turkey, there is a companion present for the majority of hospitalized adult and pediatric patients. Awareness of the companion's care burden and the possible effects of this burden on his/her health can be a guide to protecting and improving their health. Hence in this study, we aimed to evaluate the care burden, psychological distress and psychiatric disorders of companions of adult patients who were hospitalized in the medical ward of XXX University Hospital.
This study is a cross-sectional and descriptive study. The study sample comprised companions of inpatients admitted to the university hospital between January and April 2018. Companions who were over 18 years old and were involved in caring for the patient for at least 5 continuous days in the hospital were included in the study. In hospitals in Turkey, companions are not the same persons for hospitalizations of less than 5 days. In hospitalizations longer than 5 days, the same person stays with the patient as an companion. Therefore, we took 5 days as a starting point. This study is originated from one center and sample calculation and randomization were not performed based on the suggestions of the statisticians. Since the number of companions of inpatients could not be known clearly during the research, expert statisticians suggested that there should be at least 250 participants. We recruited 300 companions who agreed to participate in the study.
The inclusion criteria in the study were being older than 18 years of age, giving care to an adult patient in the hospital as a companion for more than 5 days and giving informed consent to participate in the study. The exclusion criteria were being younger than 18 years of age, giving care as a companion for less than 5 consecutive days, not giving informed consent to participate in the study and being a paid caregiver.
The XXX University Faculty of Medicine Clinical Research Ethics Committee dated 20 December 2017 and numbered 747 approved the scientific and ethical relevance of this study. Written informed consent was obtained from all companions who agreed to participate in the study. Then, the study questionnaire, which included sociodemographic data, the Zarit Caregiver Burden Scale and the Brief Symptom Inventory were administered by the researchers in face-to-face interviews. The sociodemographic information form is a 33-item form that includes items such as age, sex, educational level, income level, history of chronic illness, degree of intimacy, duration of companionship, problems encountered during hospital stay, and cause of companionship.
The Zarit Caregiver Burden Scale (ZCBS) is widely accepted as a reliable and valid scale for measuring caregivers’ burden and has been used extensively. It was developed in 1980 by Zarit, Reever and Bach-Peterson. [5] Turkish validity studies were conducted by Inci and Erdem in 2006. [23] The ZCBS, which may be filled out either by the caregiver or a researcher, consists of 22 statements on the effect of caregiving on the respondent’s/caregiver's life. Each of the statements is answered using a Likert-type scale, with scores ranging from 0 to 4 (never, rarely, sometimes, quite frequently, and nearly always). The composite score was then calculated, and the burden was graded as follows: little or no burden (≤20), mild burden (21–40), moderate to severe burden (41–60), and severe burden (>61-88). The ZCBS has good internal consistency reliability, with a Cronbach’s alpha coefficient of 0.92.
The Brief Symptom Inventory (BSI) is an instrument that evaluates psychological distress and psychiatric disorders in people. It was developed by Derogatis in 1975. [24]. The BSI is a 53-item self-report scale designed to evaluate psychopathological and psychological symptoms, measuring nine dimensions (namely, somatization, obsession–compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism). Respondents rank each feeling item (e.g., “your feelings being easily hurt”) on a 5-point scale ranging from 0 (not at all) to 4 (extremely). The rankings characterize the intensity of distress during the past seven days. The total score from the scale varies between 0 and 212.
The Turkish version used in this study was adapted to Turkish by Sahin and Durak. [25] In the Turkish version, 5 dimensions are defined.
Data Analysis - Statistical Methods
The data obtained were analyzed using IBM SPSS Packet version 24.0 (IBM Corporation, Armonk, NY, USA). While evaluating the data, the suitability of the parameters to a normal distribution was evaluated by visual (histogram and probability graphs) and analytical methods (Kolmogrov-Smirnov / Shapiro Wilk tests). Simple descriptive and inferential statistics were performed. Descriptive statistics were performed with results presented as frequencies, proportions, means and standard deviations. The Mann-Whitney U test was used if comparisons between two independent groups were normal. If the groups with more than two independent groups did not show a normal distribution, these parameters such as education level, monthly income, self-rated health, and mental illnesses of companions were compared using the Kruskal-Wallis test. Pairwise comparisons were made using the Mann-Whitney U test and evaluated using Bonferroni correction. Correlation coefficients and statistical significance were calculated by using the Spearman test for at least one normal nondistributed relationship. A multiple linear regression analysis was performed for determining factors associated with BSI scores. The type 1 error level was used as 5% for statistical significance. All P values of less than 0.05 were considered significant.
The hypothesis of this study is that psychological distress and psychiatric disorders of companions also increase as the care burden of companions of adult patients increases.
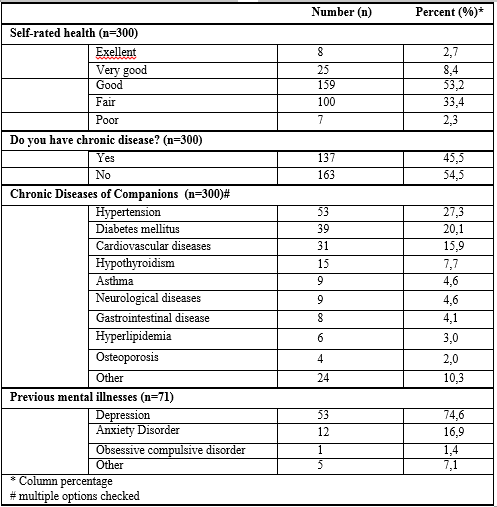
Three hundred companions participated in the study, comprising 99 (33%) males and 201 (67%) females, with ages ranging from 18 to 84 years (mean = 50 years). Half of the participants live in the city center, 37.7% were primary school graduates, 37.7% were at a low income level. Table 1 depicts the sociodemographic profile of the companions.

In the study, 35.7% of companions considered their health to be fair or poor, only 2.7% considered their health to be excellent. About half of the companions (45.5%) had at least one chronic disease; and the most frequently reported chronic disease was hypertension (27.3%). Twenty-four percent of the companions reported having had a previous mental illness. The most common mental illness was depression (17.6%). Table 2 shows the health characteristics reported by the companions themselves.
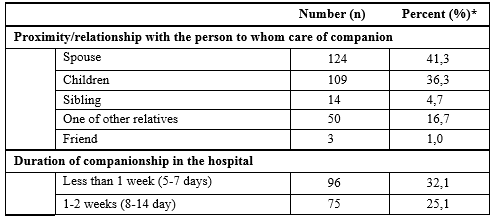
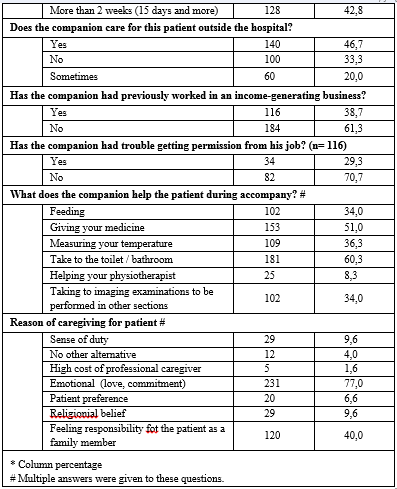
Forty-one percent of the companions were spouses of the patients, and 42.8% had been caring for their patients in the hospital for more than 2 weeks. In the study, 61.3% of the participants were not working professionally, and 30% had trouble getting permission from their job. Seventy-seven percent of the respondents reported that they were caring for the patient because of their emotional commitment. Approximately one-third of the companions did not receive support from the family, and 35.9% reported that they had problems meeting their basic needs during the hospital stay. Table 3 shows some characteristics of the companions.
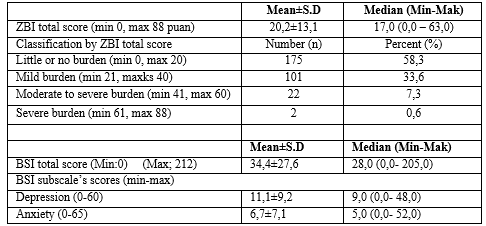
The companions’ care burden was calculated using the ZCBS. The companions’ mean ZCBS scores were 20,2±13.1. More than half of the companions (55%) had a little care burden, about 8% had a moderate to severe care burden. Psychological distress and psychiatric disorders in the companions were calculated using BSI. The mean BSI score of the participants was 34,4. Table 4 shows the distribution of ZBI scores and BSI scores of the participants.

There was a moderate positive correlation (r = 0.502) between the ZCBS and BSI scores of the participants, and it was statistically significant (p <0>0.05). The ZCBS score was found to be significantly higher in companions with a previous history of mental illness than in those without (p <0>0.05).
The relationship of patient receiving care from a companion, the duration of the companionship, the state of caregiving outside the hospital, having trouble meeting their basic needs in the hospital, the status of working a job, and the status of the problem of getting permission from work had a statistically significant effect on the care burden (p <0>Table 5.
care burden of companions who did not receive support from other family members was significantly higher than those receiving support (25.7 vs 17.7) (p <0>
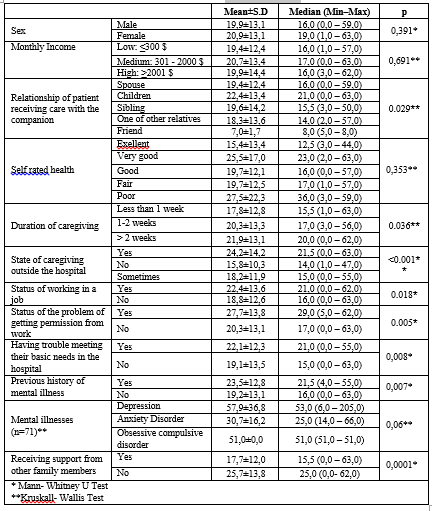
There was a statistically significant difference between the BSI scores according to sex, general health perception (self-rated health), state of caregiving outside the hospital, experiencing difficulties in meeting their basic needs in the hospital and previous history of mental illnesses of the companions (p <0>
There was not a statistically significant difference between the BSI scores according to education levels, income levels, duration of companionship, and having any diagnosed chronic disease of the companions (p >0.05). Table 6 shows the distribution of the BSI scores according to some descriptive characteristics of the companion

There was no statistically significant difference between the BSI scores and the degree of the relationship between the companion and the patient or the length of hospital care (p>0.05). Certain tasks, such as giving the patient their medication, measuring the patient’s body temperature, and helping the patient go to the bathroom and to the toilet, created more care burden for the companions and led to higher BSI scores. Lack of support from the environment and the family members of the companions significantly increased the score of the hostility subgroup (p <0>
When evaluating the reason for being a companion, the highest BSI score was from “I give care because of the high cost of professional care” (58.4%). This was followed by absence of choice (47.5%) and feeling of duty (37.7%). However, contrary to the ZCBS scores, there was no statistically significant relationship between reason for being a companion and the BSI scores (p >0.05).
As expected, companions who have problems in meeting basic needs during the hospital stay have higher BSI scores than those who do not have problems, and this difference was statistically significant (p <0>
Family members play a major role in caring for sick family members who have a chronic illness. Family members who are caring for the sick person face the care burden and may experience physical and mental health problems as a result of their care responsibilities. In Turkey, a family member remains in the hospital as a companion to the hospitalized patient and takes responsibility for the care of the patient.
As stated in the method section, a sample calculation could not be made in this study because of difficulties in predicting the total number of companions. We recruited 300 companions who agreed to participate in the study. Two-thirds of the companions were women.
In almost every country in the world, women are the main caregivers for the sick, the elderly, the disabled and the young. Caring for the sick person in the family is accepted as the responsibility of women. Historically, women are responsible for the care of the home, children, and the care in case of illness of a family member. Women accept their caregiver role as a cultural obligation.26 Patient care at home and in the hospital is considered as the natural task of women. [9] Today, although women increasingly participate in business life, the majority of family caregivers are female members of the family. [1,11] The U.S. Family Caregiver Alliance reports that upwards of 75% of all caregivers are female. [27] In a study by Chandran et al. [28] in India, 70% of family members who care for hospitalized patients are women. In a qualitative study by Passos et al. [12] in Brazil, 81% of family caregivers who care for hospitalized patients are women.
In the present study, companions’ care burden was evaluated with the ZCBS. The mean ZBI score was 20,2 / 88. This score corresponds to little burden. Studies on the care burden are more concerned with the care burden of home caregivers. There are few studies on the care burden of the companions of hospitalized patients. In Turkey, Saritas et al. [21] conducted a study with the caregivers of patients at the oncology service. The mean ZCBS score of the caregivers was found to be 25. This higher score may be due to the high burden of care for oncology patients. Chandran et al. [28] conducted a study in India, and the average ZCBS score of the caregivers for the patients in a private room was 45,4; the ZCBS score of the caregivers for the patients in a general room was 35,4. The difference between the results of this study and our results might be due to cultural beliefs and habits between the two communities and the
conditions of the hospitals. In the Turkish culture, the act of providing care to a close relative is considered to be an honor, and is performed voluntarily, whereas in Indian society, caring for hospitalized relatives is considered a cultural and religious duty. [11] In this study, the care burden did not increase in companions whose motivations are emotional ties (love, feeling close) with the patient and religious beliefs (p <0>
In a meta-analysis of 125 studies by Rodriguez-Gonzales and Rodríguez-Míguez [29] was showed that caregivers of individuals with a physical disability have an estimated mean ZCBS score of 27. The lower score in this study might be due to the shorter duration of care in the hospital and the potential for recovery in the patients who receive care.
In this study, ZCBS scores did not show statistically significant differences according to the sex, education levels, income levels, general health perception of the companions (p >0.05). However, as the length of the caregiving time increased, the care burden also increased (p <0>
In addition, working in an income-generating work and having problems in obtaining work permits to become a companion increased the care burden. In a study by Saritas et al. [21] the statistically significant relationship was not found between sex and educational status with care burden. These findings are in accordance with our conclusions.
Companions are usually relatives of patients, and they play a significant role in supporting their patients emotionally. In this study, most of the companions were spouses or adult children of the patient. The companions’ relationship with the patient receiving care affects the care burden. In this study, the highest care burden (22,4/88) was found in the adult children of the patients. This is followed by spouses and siblings (19,4/88 in both). This might be due to separation of young persons from social life or business life, which creates more stress.
More than half of the companions considered their health to be good, and 45.5% had at least one chronic disease. This is likely to be due to the average age of the companions which was 50 years old. In Turkey, the prevalence of multimorbidity in the population aged 40 and over is 27.8%, and increases with age. [30]
Companions who stay with their patients in the hospital live in uncomfortable conditions. As this period is prolonged, they experience physical and mental problems. It was previously documented that the companions have unsatisfactory physical conditions such as lack of resting and sleeping places in Turkey. [9,22] As stated in the results section of our study, the difficulty in meeting the basic needs of companions such as bathing, eating, resting and sleeping during the hospital stay increased the care burden.
In the study, BSI was used to evaluate the psychological distress of the companions. Female companions had higher BSI scores than male companions (p <0>
According to the research, there is a strong link between psychological health and physical health. [32] As expected, there was an inverse linear
relationship between the companion’s self-rated health status with their BSI scores. While the BSI score of those who evaluated their health as excellent was the lowest, those with poor health were found to have the highest BSI scores. BSI scores of the companions with a previous history of mental illness were also statistically significantly higher. However, there is no statistical difference between the BSI scores when comparing companions with chronic illnesses and those without chronic illnesses. These results show us that the healthiness perception of the companions is related to mental health rather than physical health. The absence of a significant relationship between the ZCBS score with the companion’s health self-assessment and chronic illness reinforces this assumption.
There was no statistically significant difference between the BSI scores regarding the degree of closeness between the companion and the family member receiving care and the duration of companionship at hospital (p >0.05). However, the BSI scores of the companions who provided care to the same person outside the hospital were significantly higher (p <0>
These results show that the length of the caregiving duration and the poor health perception negatively affect the mental health of the companion,
regardless of the care burden. Although the care burden of the companions was not significantly affected by current health perceptions or existing chronic diseases, the increased level of psychological symptoms may stem from the fact that the companion gives priority to the health and care of the patient rather than to his/her own health. In addition stress or sadness during the care process may also increase psychological symptoms. Further studies are needed to determine the main factors.
In this study, half of the companions stated that they also provide care to their patients outside the hospital. These people have higher ZBI scores and BSI scores than companions just providing care in the hospital. These companions may also be considered home caregivers and may have the same health risks as home caregivers. For this reason, we think that studies on long-term caregivers of chronically ill and disabled people may support our results.
Many studies have shown that caregiving affects the physical, mental, emotional and functional health of the caregiver. [1,33,34]. It is possible that this effect will be greater in people who have had mental illness before. In this study, in accordance with the expectations, both the ZCBS and BSI scores of the companions who had previous mental illness were significantly higher. Nearly three-quarters of their companions who had a history of mental illness reported that they suffered from depression. These companions had higher ZCBS and BSI scores.
The ZCBS and BSI scores of the companions who did not receive support and assistance from the other family members were significantly higher than those receiving support (p <0>
other family members to support caregiver to enhance the healing of the patients in both hospital and home. Health professionals need to monitor the health status of caregivers more carefully.
Care burden has a substantial effect on caregivers’ health. There are many studies showing that informal home caregivers have a high health risk for burden, stress, depression, irritability, aggression and these health problems leads variety of health complications during caregiving. [38,39] In a study conducted by Schulz and Beach [40], individuals who care for their spouses at an older age were compared in a 4-year cohort study. It was found that the mortality risk of individuals who care for their spouse and feel the burden of care is 63% higher than those who do not need to care for their spouse.
In our study, 46.7% of the companions stated that they gave care to their patients outside the hospital. These people have higher ZBI scores and BSI scores than companions just providing care in the hospital. These companions may also be considered home caregivers and may have the same health risks as home caregivers. Healthcare professionals need to monitor the health status of these people more carefully.
It is accepted that educating caregivers or companions about the illness and care process may reduce the anxiety and care burden of caregivers or companions, and may therefore have positive results in family relations. [1,8,41]
In our study, the companions reported that they were pleased that the physicians provided sufficient explanations about the condition and care of their patients. Getting enough information from the physicians in the hospital and consulting them when making healthcare decisions reduce the concerns about the treatment and prognosis of their patients. For this reason, it is important for healthcare professionals to approach hospitalized patients and their companions in a more empathetic manner, and to take medical decisions in a shared decision-making approach. This attitude will increase the satisfaction of physicians by improving patient outcomes. [42]
The companions of the hospitalized patients had a mean ZCBS score of 20,2 and a mean BSI score of 34,4. As the care burden of companions increased, the levels of psychological distress also increased. The support of health workers and family members reduced the companions’ care burden and psychological distress. Companions also need more assistance from health care institutions to cope with care burden. Physicians working in the hospital should take into account that companions may be hidden patients and should encourage other family members to provide support to the companions to protect their health.
Companions can increase the efficacy of healthcare services by facilitating the communication between patients and healthcare providers. By providing physical and emotional support to the patient, the companion contribute to the recovery of the patient, and shorten the length of stay in the hospital. [2]
In the last decades, participation of family members in hospital care is encouraged. In order for family members to make the best of their contribution to health care, their health should be protected, their care burden should be reduced and support should be provided. It requires that hospital administrators and ministry of health officials to work together and arrange appropriate and sufficient physical conditions (e.g. spaces for resting and sleeping) for companions within the hospital.
The limitation of the study and suggestions for future studies
This study is the first to investigate the health status and care burden of companions. There are some limitations to our study. First, as a cross-sectional study from single center, the findings of this study might be difficult to generalize and no cause-effect relationship could be established because the sample was not clinically and demographically representative of the general population. Second, this study is based on the subjective assessments of companions. To the best of our knowledge, this is the first study investigating the health status of companions. The companionship in not unique to Turkey as explained above. Multi-center studies with larger samples are needed on companions. Further studies are needed to increase the generalizability of this study’s findings.
Declarations
Ethics approval and consent to participate
The scientific and ethical relevance of this study was approved by the XXX University Faculty of Medicine Clinical Research Ethics Committee dated 20 December 2017 and numbered 747. All researchers have signed the declaration of Helsinki. Written consent was obtained from all participants. Written informed consent was obtained from all companions who agreed to participate in the study.
Consent for publication. Not Applicable
Competing interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. The research is financed by the authors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
