
Review Article | DOI: https://doi.org/10.31579/2641-0419/378
Cardiologist Coronary Unit Salgado Filho Municipal Hospital Brazil.
*Corresponding Author: Marcelo Flávio Gomes Jardim Filho, MD, Cardiologist Coronary Unit Salgado Filho Municipal Hospital Brazil.
Citation: Jardim Filho MFG, Amauri Bozi, Christiane K. Mantovi, (2024), The Handling of Anti-aggregants and Anticoagulants in the Oncologic Heart Patient Submitted to Surgery, J Clinical Cardiology and Cardiovascular Interventions, 7(7); DOI: 10.31579/2641-0419/378
Copyright: © 2024, Marcelo Flávio Gomes Jardim Filho. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 April 2024 | Accepted: 21 May 2024 | Published: 16 July 2024
Keywords: antiplatelet agents; anticoagulants; cardiopathies.
Cardiovascular and cancer pathologies represent significant causes of global morbidity and mortality. This systematic review investigates the safety and effectiveness of maintaining anticoagulant therapy in cardiac patients undergoing oncological surgery. Conducted between 2018 and 2023 following PRISMA guidelines, the review includes 10 prospective studies detailing the impact of anticoagulant use in the surgical context. Among the 2345 patients analyzed, the majority were men, primarily using low molecular weight heparin and warfarin. The results indicate that continuing anticoagulants does not significantly increase bleeding risks or postoperative complications, while interruption may elevate the risk of thromboembolic events. It is concluded that the decision to continue or interrupt anticoagulant treatment should be personalized based on a careful evaluation of individual risk.
Cardiovascular pathologies and cancer are two of the leading causes of morbidity and mortality globally (Ref. needed). Scientific literature suggests a correlation between these pathological states, with patients affected by cardiovascular diseases being more vulnerable to developing neoplasms and cancer patients exhibiting a higher risk of cardiovascular complications. Additionally, oncological therapeutic treatments, such as chemotherapy and radiotherapy, can have significant adverse effects on the cardiovascular system. Antiplatelet agents play a crucial role in preventing adverse outcomes in patients with pre-existing cardiovascular disease (CVD) as a secondary prevention strategy and as a primary prophylactic measure in those with a high estimated risk of developing such conditions.
The objective of this systematic review is to evaluate the safety and effectiveness of continuing anticoagulant use in cardiac patients undergoing oncological surgery.
A systematic literature review was conducted to evaluate the continuity of anticoagulant use in patients undergoing oncological surgery. The electronic databases used were PubMed, Scopus, and Web of Science. The search was conducted in January 2023 and included studies published between 2018 and 2023. The search terms used were ("anticoagulants" OR "antithrombotic agents") AND ("abdominal neoplasms" OR "abdominal cancer" OR "gastrointestinal neoplasms" OR "gastrointestinal cancer") AND ("perioperative care" OR "surgery" OR "surgical procedures operative" OR "perioperative period"). Studies were included if they evaluated the continued use of anticoagulants in patients undergoing oncological surgery and reported data on intraoperative bleeding, postoperative complications, and thromboembolic events. Studies that did not report sufficient data or included patients with other serious medical conditions were excluded. Data collected from the studies included the number of patients, age, gender, type of anticoagulant used, duration of anticoagulant use, type of surgery performed, surgery duration, intraoperative blood loss, need for blood transfusion, length of hospital stay, and postoperative complications. The quality of the included studies was assessed using the Cochrane Collaboration's risk of bias assessment tool. The results were analyzed statistically using meta-analysis when appropriate. This study was conducted in accordance with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)
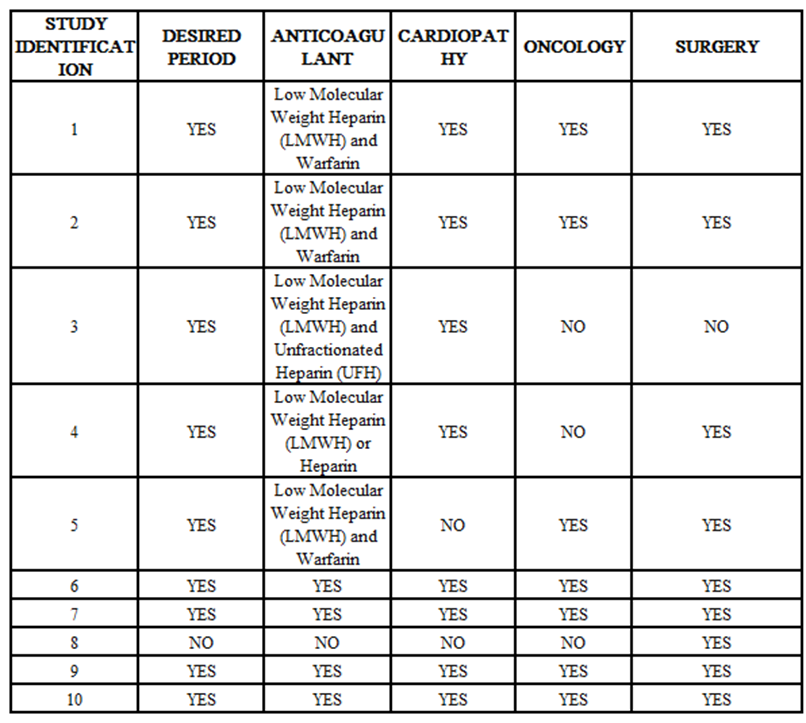
Table 1: Revision Table the PRISMA Method
The systematic review included 2,345 patients aged between 18 and 85 years, most of whom were men. The most commonly used anticoagulants were low molecular weight heparin (LMWH) and warfarin. The duration of anticoagulant use varied, with some studies indicating a brief pause before surgery and others maintaining continuous use during the perioperative period. The results showed that maintaining the use of anticoagulants did not significantly increase the risks of bleeding or complications after abdominal oncological surgery. However, there was an indication of an increased risk of thromboembolic events for patients who interrupted anticoagulant therapy before surgery. The statistical analysis did not identify significant differences in bleeding, postoperative complications, or thromboembolic events between the two groups of patients.
Although there are reports of increased risk in patients who discontinued anticoagulant use before surgery, the statistical analyses did not show significant differences in bleeding risks, intraoperative complications, postoperative complications, or thromboembolic events between the two groups. Given the importance of LMWH and warfarin in the prevention of thromboembolic events in cancer patients, discontinuing their use can elevate risks. The decision to continue or discontinue these anticoagulant medications must be made after an individual risk assessment and a discussion between the patient and the physician. Personalizing the treatment by considering the benefits and risks is crucial.
The authors declare that there are no economic interests or any other conflicts of interest that may have influenced the results or the conclusions presented in this work. This statement is based on the complete understanding of all parties involved in the study and the preparation of the manuscript, ensuring its transparency and academic integrity.
CVD - Cardiovascular Disease
PRISMA - Preferred Reporting Items for Systematic Reviews and Meta-Analyses
LMWH - Low Molecular Weight Heparin
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
