
Research Article | DOI: https://doi.org/10.31579/2641-5194/004
Laxmisamhitha Bontha, Deportment of Pharmaceutics, Lamar University, Beaumont, Texas
*Corresponding Author: Laxmisamhitha Bontha, Deportment of Pharmaceutics, Lamar University, Beaumont, Texas. E-mail: vijaypharmacy2000@gmail.com
Citation: Laxmisamhitha Bontha, Vijayakumar Bontha , The Frequency and Significance of Portopulmonary Venous Anastomosis (PPVA) and Transvenous Obliteration for Gastric Varices., J. Gastroenterology Pancreatology and Hepatobilary Disorders. 2(1). DOI: 10.31579/2641-5194/004
Copyright: © 2018 Laxmisamhitha Bontha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 August 2018 | Accepted: 20 August 2018 | Published: 26 August 2018
Keywords: frequency and significance; portopulmonary venous anastomosis; gastric varices
A Portopulmonary Venous Anastomosis (PPVA) is a direct vascular connection between the portal venous system and the pulmonary veins, close to the left atrium. We describe a patient with advanced cirrhosis and moderately severe Hepatopulmonary Syndrome (HPS) in whom (PPVA) was demonstrated by a high resolution computed tomographic scan. In order to reduce the symptoms of hypoxia in our patient, we sequentially performed Transjugular Intrahepatic Portosystemic Shunt (TIPS) followed by a catheter based obliteration of the PPVA. The case raised three questions which were addressed through an extensive literature review.
Among patients with advanced cirrhosis, what is the frequency of PPVA? Our literature review suggests that the frequency of finding a PPVA in patients with portal hypertension depends on the imaging technique used. Transhepatic or transvenous portal venography may demonstrate PPVA in about 20% of patients with cirrhosis and varices. Limited published experience with contrast enhanced (bubble) echocardiography suggests that PPVA may be present in about 30% of such patients. An increasing number of case reports of PPVA have been published in recent years. This observation indicates that routine use of High Resolution Computed Tomography (HRCT) and magnetic resonance imaging is able to identify PPVA in cirrhotic patients. The visualization of PPVA with HRCT depends on the timing of the contrast injection and the expertise of the viewer.
The present report describes three patients with portopulmonary venous anastomosis (PPVA) in whom balloon-occluded retrograde transvenous obliteration (B-RTO) of gastric varices was attempted. No patients had a gastrorenal shunt. In one patient, after an approach from the inferior phrenic vein (IPV), the PPVA was embolized with the use of microcoils.
Portopulmonary Venous Anastomosis Detected at Balloon-occluded Retrograde Transvenous Obliteration for Gastric Varices among cirrhotic patients with PPVA, what is the clinical significance of the PPVA? There are multiple causes of clinically significant hypoxia in patients with cirrhosis. A PPVA is a right to left shunt that, theoretically, could be associated with clinically significant systemic arterial hypoxemia or emboli. There is not definitive evidence in the published literature that PPVA alone causes clinically significant hypoxia in cirrhotic patients. PPVA is, however, a documented important risk factor for systemic emboli when needle or catheter techniques are used to treat or prevent bleeding from gastroesophageal varices.
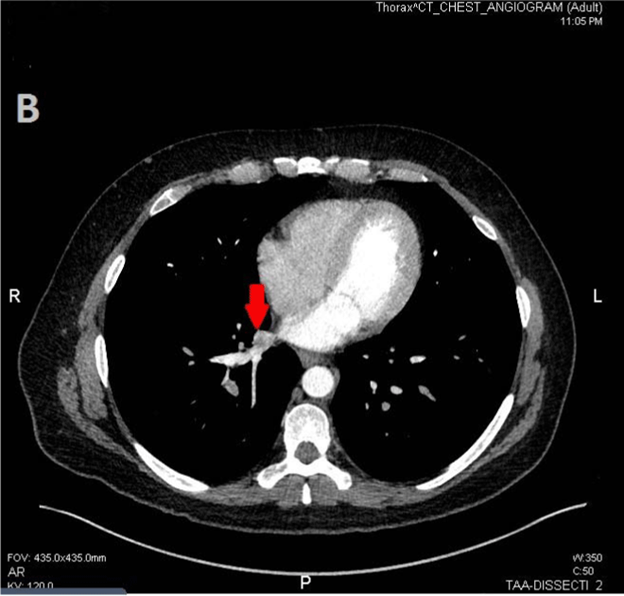
Portal hypertension is a common complication of cirrhosis. The increased pressure in the portal system leads to the development of portosystemic collateral vessels. Many pathways of collateral communication between the portal and systemic circulation have been described [1,2]. Some cirrhotic patients with portal hypertension develop collateral communication between the portal system and the pulmonary veins [3,4]. These collaterals have been called Portopulmonary Venous Anastomosis (PPVA). The term PPVA differentiates direct portal to pulmonary vein anastomosis from the intra-pulmonary shunts associated with the Hepatopulmonary Syndrome (HPS). This report describes a cirrhotic patient diagnosed with HPS. He was not a candidate for liver transplantation. In the setting of progressive symptoms of defective oxygenation, further studies were done to find an additional treatable cause of hypoxemia. Computed tomography revealed a PPVA connecting a large paraesophageal varices to the right inferior pulmonary vein. We hypothesized that the shunt may be contributing to the hypoxemia. We also hypothesized that the hypoxia might be improved if the portal pressure was reduced or if the PPVA was obliterated. There is limited data in the literature about the relation between PPVA and clinically significant hypoxia.
Initial management of gastric variceal bleeding involves diagnostic and therapeutic considerations. (5,6)Patients who are planning to undergo a BRTO procedure for bleeding gastric varices require preprocedural assessments that include endoscopy and clinical, laboratory, and imaging evaluation. Patients undergoing BRTO are cirrhotics that require a multidisciplinary team approach, as described earlier.2
Patients who are potential candidates for BRTO are either stable or unstable. BRTO has been reported to be effective in controlling active bleeding from gastric varices.(7,8) Obviously, stabilizing patients is a priority before full clinical and diagnostic assessment, although realistically both clinical assessment and stabilization occur simultaneously. Almost all patients with gastric varices with established gastrorenal shunts (traditional BRTO candidates) have cirrhosis that may be suspected by prior evaluation or through historical, physical examination, and laboratory findings. In patients with known or suspected portal hypertension, medical therapy is required, including antiportal hypertension medications and antibiotic prophylaxis.2
Not all patients undergoing BRTO for gastric varices are unstable; in fact, most are stabilized before the actual BRTO procedure. Basic life-sustaining and resuscitative measures routine to any form of gastrointestinal bleeding are initiated. However, physicians must be cognizant of avoiding overaggressive fluid resuscitation that can exacerbate portal hypertension because multiple reports have established that volume expansion increases portal vein pressure.(9,10,11) Variceal bleeding is predominantly portal pressure driven; thus it is apparent that minimizing portal pressure is an important goal in managing these patients. To avoid significant volume expansion and subsequent elevated portal venous pressures, systemic blood pressures lower than normal are therefore acceptable. Also to this end, a lower target hematocrit (21%) with packed red blood cell transfusions, along with optimization of platelet count and function, are commonly targeted goals.41,42 Renal function support may also be necessary for volume control and platelet function.
Endoscopic Management of Bleeding Gastric Varices
Once the patient is stabilized, upper gastrointestinal endoscopy is usually undertaken as a routine early measure to evaluate upper gastrointestinal bleeding. Upper gastrointestinal endoscopy is essential for diagnosing, triaging the management of, and/or treating upper gastrointestinal bleeding.(9,10)The identification of which varices, if any, are bleeding is essential. Esophageal varices can be controlled effectively by endoscopic-guided banding and sclerotherapy. Bleeding esophageal varices that cannot be controlled medically and endoscopically would warrant a TIPS procedure and not a BRTO.Bleeding from gastric varices that are small and exhibit slow flow by endoscopic Doppler ultrasound (EUS) can be sclerosed (or “glued”) endoscopically and may not necessarily require a BRTO procedure.(12,13,14) However, if there are large fundic and/or cardiac gastric varices exhibiting high flow, some endoscopists would defer to a BRTO procedure due to concerns about causing intravascular (usually systemic venous) nontarget embolization of the sclerosant. Obviously, if bleeding is from a combined gastric and esophageal varices, then the esophageal varices can be managed by endoscopy and large high-flow gastric varices could be managed by BRTO. In the presence of large high-flow gastric varices and prominent but not bleeding esophageal varices, preemptive esophageal variceal banding may be warranted because BRTO exacerbates portal hypertension and may aggravate esophageal varices
Between December 1994 and November 1997, balloon-occluded retrograde transvenous obliteration was performed on 20 patients with gastric varices in danger of rupture and with gastrorenal shunts; three patients also had hepatic encephalopathy. The sclerosant was injected into the gastric varices during balloon occlusion. The degree of progression of the gastric varices and of collateral veins was classified into five grades, with grade 1 being least progression and grade 5 most progression; collateral veins that had developed were treated with embolization. Follow-up consisted of fiberoptic endoscopy and computed tomography.
Technical success was achieved in all patients. Occlusion of collateral veins was essential for the occlusion of gastric varices with a grade greater than grade 2. The clinical symptoms of hepatic encephalopathy in the three patients improved remarkably. Follow-up endoscopy 3 months after the procedure revealed the disappearance of gastric varices in 15 patients and reduced variceal size in five. During the follow-up period, 19 patients had no recurrence of gastric varices; three patients had aggravation of the esophageal varices.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
