
Research Article | DOI: https://doi.org/10.31579/2641-0419/055Copyright
*Corresponding Author: Gary L Murray, The Heart and Vascular Institute, 7205 Wolf River Blvd, Germantown, TN, 38138, USA
Citation: Gary L. Murray, Colombo J (2020) The Feasibility of Blood Pressure Control with Autonomic- Assisted Hypertension Therapy Versus JNC 8 Therapy. J. Clinical Cardiology and Cardiovascular Interventions, 3(4); Doi:10.31579/2641-0419/055
Copyright: © 2020 Gary L. Murray. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 February 2020 | Accepted: 13 March 2020 | Published: 18 March 2020
Keywords: hypertension; parasympathetic nervous system; sympathetic nervous system; autonomic nervous system.
Background: Over one billion people have Hypertension (HTN); mortality and morbidity are increasing. The Parasympathetic and Sympathetic (P&S) nervous systems prominently affect the onset and progression of HTN, yet P&S measures are not used to assist in management. Our objective was to determine the feasibility of HTN control using P&S-guided to JNC 8 HTN therapy.
Methods: 46 uncontrolled HTN patients were randomized prospectively to P&S-assisted management, adjusting JNC 8 therapy using the ANX 3.0 Autonomic Monitor and adding (r) Alpha Lipoic Acid (Group 1) vs. JNC 8 (Group 2).
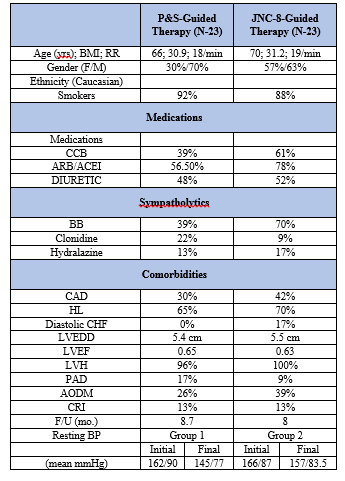
Results: The two Groups were similar in: 1) age (mean 66 vs. 70 y/o for Groups 1 and 2, respectively; 2) initial resting home Blood Pressure (BP, Group 1 mean=162/90 mmHg vs. Group 2 mean=166/87 mmHg, 3) initial resting office BP Group 1 mean=151/75 mmHg vs. Group 2 mean=155/73 mmHg, and 4) ethnicity. Upon follow-up (mean=8.35 mo.): 1) mean resting home BPs were 145/77 mmHg (Group 1, 74% of patients at JNC 8 goal) vs. 155/83.5 mmHg (Group 2, 30.4% at JNC 8 goal), and 2) mean resting office BPs were 138/71 mmHg (Group 1) vs. 146/65 mmHg (Group 2). At the study’s conclusion, Group 1 Sympathetic tone was lower than that for Group 2 both at rest and upon standing, and Group 1 Parasympathetic tone was higher than that for Group 2 both at rest and upon standing.
Conclusion: P&S-assisted HTN therapy is feasible, resulting in improved BP control, through healthier P&S tone on fewer prescription medications.
Hypertension (HTN) is the most common disorder seen in family practice, affecting over 25% of primary care patients. Less than 50% of hypertensives are controlled, and mortality as well as morbidity is increasing. While several causative mechanisms of HTN have been elucidated, much investigation remains [1,2].
A neuroadrenergic cause is prominent: Increased Sympathetic (S) tone and Cardiac Output (CO) with low systemic vascular resistance (Rs) occur in young hypertensives; eventually, the high CO and S-tone usually come down (3); Rs increases, uncoupling it from S-tone; and decreased Baroreceptor Reflex (BR), cardiopulmonary receptor sensitivity, and Parasympathetic (P) tone are present, likely resulting from end-organ damage [1,3-8]. If P<
Despite the involvement of Parasympathetic and Sympathetic function in HTN, routine pharmacologic management of HTN is not tailored for it, potentially contributing to reduced time in therapeutic range that is inversely associated with all-cause mortality, resistant HTN, the 24% HTN recidivism, as well as undesirable orthostasis and fatigue [12,13]. Additionally, the increased oxidative stress that can contribute to the development of HTN and ANS dysfunction is also not specifically addressed therapeutically.
We, as have others, have found the potent, natural antioxidant (r) Alpha Lipoic Acid ([r]-ALA) can reduce sitting systolic and diastolic BP [14-16]. Therefore, our hypothesis is that pharmacologic HTN treatment, adjusted for P&S dysfunction when present treated with adjunctive (r)-ALA, could result in improved P&S function and HTN control using fewer prescription medications. The cost and side effects of treatment might be reduced. This is a prospective, controlled, hypothesis- generating, feasibility study.
In a suburban, mid-west cardiology clinic 46 consecutive patients (70% Female, average age 66 years, age range 33 to 88 years, 92% Caucasian, see (Table 1) were recruited for this feasibility study. At baseline, all patients were under standard care based on the Eighth Joint National Committee (JNC-8) guidelines. At baseline, all patients recruited: 1) Were treated but uncontrolled HTN (unmet JNC goals) patients with any abnormality in P-and/or S-tone regardless of all other vital characteristics, 2) Signed informed consent, and 3) Were randomly, prospectively assigned to P&S-assisted therapy (Group 1) or JNC 8- guided only therapy (Group 2).
All patients were on a 2 gm. sodium diet and asked to perform at least
2.5 hr. aerobic activity/wk. and to stop smoking. All patients with obstructive sleep apnea were appropriately treated. P&S-assisted therapy consisted of adjusting JNC 8 therapy as well as adding (r)- ALA per our usual treatment for dysautonomia in patients without HTN. The groups’ ages are similar: Group 1 averaged 66 y/o and Group 2 averaged 70 y/o (p<0.001). The groups’ follow-up times are similar: Group 1 averaged 8.7 months and Group 2 averaged 8.0 (p<0.001). Five days of home morning and evening BP monitoring were collected.
Each monitoring event recorded BP after 5 minutes of quiet sitting and the data were averaged upon entry. Three days of b.i.d BPs were averaged 2 months of adding (r)-ALA in Group 1, in order to allow it to take full effect and monthly thereafter, whereas BPs were repeated 2 weeks after entry in Group 2 and monthly afterwards. Physician measured BPs were never used in this unblinded trial and doses of antihypertensive medications, along with changes, were per JNC 8 guidelines in both groups; only the choice of medication, the use of alpha lipoic acid, and the frequency of medication change (less frequent in Group 1 since alpha lipoic acid requires at least 2 months for full effect, thereby excluding bias in favor of Group 1) differed Blood pressure goals were identical: patient recorded home BPs that would meet JNC goals. Office P&S testing measurements were taken with the ANX 3.0 autonomic monitor (TMCAMS, Inc., Atlanta, GA, USA, formerly ANSAR Medical Technologies, Inc., and Philadelphia, PA, USA). P&S activity were computed simultaneously and independently based upon concurrent, continuous time-frequency analyses of Respiratory Activity (RA) and Heart Rate Variability (HRV) [17-21]. P-activity (measured as the Respiratory Frequency area (RFa) is defined as the spectral power within a 0.12 Hz-wide window centered on the Fundamental Respiratory Frequency (FRF) in the HRV spectrum. FRF is identified as the peak spectral mode of the time- frequency analysis of RA.
Effectively, FRF is a measure of vagal outflow as it affects the heart (a measure of cardio-vagal activity). S-activity (measured as the Low Frequency area (LFa) is defined as the remaining spectral power, after computation of RFa, in the low- frequency window (0.04-0.15 Hz) of the HRV spectrum. High Sympathovagal Balance (SB=LFa/RFa) is defined as a resting ratio >2.5, established in our 483 patient study [9]. P&S activity was recorded from 5 mins of quiet sitting (normal ranges for both P&S at rest, including sitting, is defined as 0.5-10 beats/minute2 [bpm2]). The reported average SB is the average of the ratios of 4 second samples during sitting, not a ratio of the averages. Cardiac Autonomic Neuropathy (CAN) is defined as critically low, resting P-activity, RFa of <0.10 bpm2.
High SB and CAN define a high risk of mortality, including: acute coronary syndromes, congestive heart failure or ventricular tachycardia/fibrillation alone or as a composite endpoint [9]. With challenge (e.g., head-up postural change or standing), a normal S- response (LFa) is defined as up to a 400% increase with respect to rest (e.g., sitting) and a normal P-response (RFa) is a decrease with respect to rest. Follow-up BPs and P&S measures were recorded 2 months after therapy adjustment in Group 1, whereas BPs were rechecked 2-4 weeks after adjustments in Group 2. Statistical analyses were performed in SPSS v22.0. Dichotomous data were analyzed using the chi-square test. A p-value of 0.05 or less was significant. Student t-tests as two-tailed with equal variance.
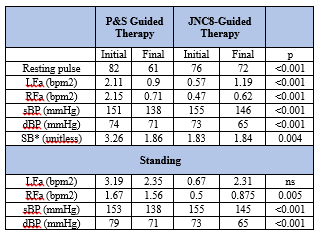
Although the two groups had similar initial BPs, home BP control was more normalized in the P&S-assisted patients. After a mean f/u of 8.35 mo., mean resting, home BPs were lower in Group 1 (145/77 mmHg, 74% 0f patients at JNC 8 goal, mean pulse 61 bpm) vs. Group 2 (155/83.5 mmHg, 30.4% of patients meeting JNC 8 goal, mean pulse 73 bpm; p<0.001 systolic, p= <0.001 diastolic, p<0.001 pulse). Similarly, Group 1 mean sitting office BPs were 138/71 mmHg vs. Group 2’s 146/65 mmHg; p<0.001 systolic, p<0.001 diastolic.
All Group 1 patients demonstrated at least 1 abnormal autonomic measure initially, managed exactly as in normotensives, and improved final office P&S measures (Table 2), including: lower resting (sitting) S-tone (LFa=0.90, p<0.001), higher final P-tone (RFa=0.71, p<0.001), and higher standing P-tone (RFa=1.56, p=0.005) as compared with final Group 2 values were present. All of these differences are consistent with improved HTN control. Prescribed sympatholytics influenced the results. Initially, 6 of 23 (23%) Group 1 patients had low sitting S-tone (LFa<0.5 bpm2) vs. 17 of 23 (74%) in Group 2, p<0.001. Group 2 had a higher percentage of patients prescribed sympatholytic.
As a result, with P&S-Assisted therapy, all but one (5 of 6 or 83%) of the Group 1 patients with low resting S-tone improved vs. 9 of 17 (53%) of similar Group 2 patients, p<0.001. These improvements also reduced the symptoms of fatigue and orthostatic hypotension in these low resting S-tone patients. P-tone directly and indirectly affects S-tone and thereby may affect BP. Low-resting P-tone may result in high resting S-tone, since P-and S-tone typically variate reciprocally. High S-tone increases BR activity, attempting to lower BP; low P-tone does the opposite. These opposing actions may increase difficulty in controlling BP in hypertensives. Initially, 7 of 23 (30%) Group 1 patients had low resting P-tone (<0.5 bpm2), vs. 15 of 23 (65%) Group 2 patients (p<0.001).
Group 1 final P-tone increased in 4 of 7 (57%) patients with low P-tone vs. Group 2 in which only 3 of 15 (20%) patients increased P-tone (p<0.001). CAN is extremely low P-tone (<0.01 bpm2). CAN is often associated with high SB. CAN with high SB is associated with increase MACE risk [9]. Initially, no Group 1 patient presented with CAN, vs. 7 of 23 (30%) Group 2 patients (p<0.001). At the end of the study, 3 of 23 (13%) Group 1 patients had CAN vs.5 of 23 (22%) with CAN in Group 2 (p=ns). A lower S-tone in Group 1 is associated with a smaller, increased MACE risk of CAN [9]. High SB was demonstrated by 8 of 23 (35%) of the Group 1 patients vs.4 of 23 (17%) patients in Group 2 (p<0.001). SB was corrected (normalized SB) in 5 of the 8 (62.5%) high SB patients of Group 1 vs. no (0%) high SB patients of Group 2 demonstrated normalized SB (p<0.001).
High SB is a measure of (relatively) high resting S-tone. Combining the resting S-tone results and CAN (very low P-tone) results, these findings support the hypothesis that lower S-tone lowers the risk of CAN [9]. At the end of the study, Group 1 patients had more patients with lower S-tone and patients with lower CAN risk. Upon standing, 8 of 23 (35%) of Group 1 patients initially had Sympathetic Withdrawal (SW, consistent with BR and cardiopulmonary receptor dysfunction) vs. 12 of 23 (52%) of Group 2 patients (p=0.01). SW was corrected in 5 of the 8 (62.5%) Group 1 SW patient vs. 4 of the 12 (33.3%) Group 2 SW patients (p<0.003).
Corrected SW indicates improved BR function. Inappropriately increased P-tone (P excess, PE) upon standing (the normal change is to decrease) initially occurred in 9 of 23 (39%) of Group 1 vs. 5 of 23 (21%) of Group 2 patients (p=0.004). PE was corrected in 6 of 9 (67%) of Group 1 PE patients and in 1 (20%) of the patients in Group 2 PE patients (p<0.001). However, PE developed in 3 (21%) of the other Group 1 patients and in 2 (11%) of the other Group 2 patients. Therefore, final PE was equally present (26%) in both Groups. Probably PE indicates a compensatory mechanism (vasodilatation) to increase blood volume thus attempting to maintain HTN.
While increased standing P-tone lowers BP, a pronounced increase can result in orthostasis, as can extreme SW. SB improved dramatically in Group 1 patients from 3.26 to 1.86 (p=0.004, Table 2), despite fewer patients using beta blockers, contrasted with essentially no change of SB in Group 2. This is consistent with the difference in HTN control. Despite nearly equal mean lower final S-and P-tone in Group 1, SB fell substantially, because SB is reported as the average of ratios, rather than the ratio of averages.
Since the final SB in both Groups was virtually equal, SB cannot be inferred solely by the BPs which was significantly different. With adjunctive P&S-guided therapy, home BP control was more normalized in Group 1 than without in Group 2: 134/77 mmHg vs. 155/83.5 mmHg, respectively (p<0.001 for systolic BP and p<0.001 for diastolic BP). The two patient groups were prescribed a mean of 2.3 vs. 3.0 prescription anti-hypertensives, respectively. More Group 2 patients were prescribed Calcium Channel Blockers (CCB) and at a higher daily mean dose (7.1 mg vs. 12.1 mg of Amlodipine for Groups 1 and 2 respectively). Both groups were prescribed Beta Blockers (BB) at similar mean doses, except for Carvedilol (40 mg for Group 1 vs. 32.5 mg for Group 2).
Both groups were prescribed Angiotensin Receptor Blockers (ARB) or Angiotensin Converting Enzyme Inhibitors (ACEI) at similar mean doses, except for Losartan (100 mg for Group 1 vs. 50 mg for Group 2) and Lisinopril (40 mg for Group 1 vs. 22 mg for Group 2). More Group 1 patients took Clonidine at a lower mean dose (0.24 mg vs. 0.6 mg) and Hydralazine was used similarly in both Groups (Table 1). Changes in medications were as follows: 5 of 23 (22%) of Group 1 vs. 7 of 23 (30%) of Group 2 patients were prescribed higher doses of medication; 14 of 23 (61%) of Group 1 vs. 100% of Group 2 had a new drug introduced; 3 of 23 (13%) of Group 1 vs. 2 of 23 (9%) of Group 2 were prescribed lower doses of medications and 17% of Group 1 vs. 9% of Group 2 had a change of medication drug class. Group 1 took a mean dose of 761 mg (r)-ALA.
This study demonstrates improved HTN BP control on fewer prescriptions using adjunctive (r)-ALA in Group 1 (74% of patients at JNC 8 goal vs. 30.4% of Group 2 patients, p<0.001). We and others have shown (r)-ALA can reduce resting BP and in this study concomitantly may assist lowering standing BP [16,22]. Superficially, the medication administration profiles do not explain the improvement in BP control, as more Group 2 patients took beta blockers, CCBs, and ARB/ACEIs. It may be that (r)-ALA’s favorable P&S effects significantly contributed to better HTN control via S-and P-dependent as well as its ANS-independent endothelial effects. Two Group 1 patients normalized BP solely by taking (r)-ALA.
Based upon P&S measures, 17% of Group 1 patients had a change of drug class vs. 9% in Group 2. This likely was also beneficial. High SB corrected in 71% of Group 1 patients vs. none in Group 2, contributing to lowering HTN [22]. Amlodipine increases SB, while beta blockers and clonidine decrease SB; beta-blockers and ARB/ACEIs improve BRS; and non-dihydropyridine CCBs decrease BRS [22-27]. (r)-ALA is a powerful natural antioxidant that improves P&S function including BRS, nitric oxide levels, and endothelial dysfunction [15,16,22,28]. Sympathetic Withdrawal upon standing results in compensatory mechanisms to preserve perfusion of vital organs that include increasing S-tone, both supine and sitting.
This exacerbates HTN, thereby causing its control to be more difficult. Sympatholytics, therefore, can worsen SW (only clonidine has a minimal adverse effect as it increases BRS [24,25,29]. Group 1 patients significantly improved SW. This is consistent with improved BRS, probably by (r)-ALA and higher doses of Lisnopril and Losartan. P- excess (PE) upon standing is indicative of ANS dysfunction, and 9 of 23 (39%) of Group 1 vs. 5 of 23 (22%) of Group 2 patients initially displayed PE. PE may also trigger compensatory measures, including secondary S-excesses that increase BP.
The central alpha action of Carvedilol, Low Dose Serotonin Reuptake Inhibitors (SSRI), as well as Tricyclics (TC) may help to reduce PE. One Group 1 patient normalized PE and HTN with addition of (r)-ALA alone. Resting P&S measures were utilized in choosing medications as follows. If P&S balance (as measured by SB) was normal, then any anti-hypertensive was prescribed.
If SB was high due to a relative, resting S-excess), then sympatholytics were chosen or adjusted. If SB was high due to low P, then sympatholytics were avoided and an ARB/ACEI and/or Diltiazem were chosen or adjusted. High dose (r)-ALA may increase resting P-activity and thereby lower SB. Upon standing, if SW was absent, then any antihypertensive was prescribed. If SW was demonstrated, then sympatholytics were avoided (excepting Clonidine) as was Diltiazem and Amlodipine, Hydralazine and/or high dose (r)-ALA prescribed. Diuretics were utilized only for dependent edema, since intravascular volume needed to be maintained. Low dose ARB/ACEI also might be prescribed. If PE presented, again intravascular volume should be preserved, so diuretics were avoided. Since an increase in S-activity is a compensatory mechanism to combat orthostasis, sympatholytics were avoided (except low dose carvedilol whose central alpha action reduces P-tone and possibly clonidine). Amlodipine is a good choice only if S- tone isn’t high, since it increases S-activity.
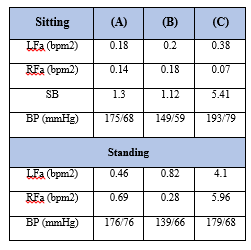
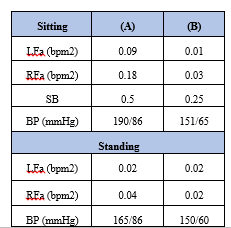
Adjunctive low dose TC or SSRI would have useful to reduce P- activity, but we confined our therapy to traditional anti-hypertensives. The uncoupling of P&S function to Rs in HTN results in variable P&S profiles. Anti-hypertensives have variable P&S effects. Consequently, knowledge of S-and P-tone is essential for choosing the best anti- hypertensive drugs and (r)-ALA enhances their effectiveness, given (r)- ALA’s ANS antioxidant effect which reduces ANS dysfunction secondary to the increased oxidative stress associated with HTN, chronic diseases and the aging process (Tables 3, 4 and 5 are illustrative).
P&S-assisted treatment of HTN, with adjunctive (r)-ALA for
dysautonomia is feasible and results in more normalized BP control within one year. Our hope is that reduced long-term medication costs, mortality, and morbidity will follow if BP control is sustained. A randomized, prospective clinical outcome study should be dome.
These results are short-term, single center, in 46 patients. Our accent was specifically lowering SB. Reducing standing PE with low dose TCs or SSRIs could have improved BP control further.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
