
case report | DOI: https://doi.org/10.31579/2690-4861/725
1Parc Taulí Hospital Universitari, Department of Medical Oncology. Institut d’Investigació I Innovació Parc Taulí (I3PT-CERCA). Universitat Autònoma de Barcelona, Sabadell, Spain.
2Clínica Universidad de Navarra, Department of Radiology, Pamplona, Spain.
3Clínica Universidad de Navarra, Department of Medical Oncology, Pamplona, Spain.
*Corresponding Author: Marina Sierra-Boada, Parc Taulí Hospital Universitari, Department of Medical Oncology. Institut d’Investigació I Innovació Parc Taulí (I3PT-CERCA). Universitat Autònoma de Barcelona, Sabadell, Spain and Salvador Martín-Algarra, Clínica Universidad de Nava
Citation: Marina S. Boada, Isabel V. Pérez, Salvador M. Algarra, (2025), The Evolving Liver of a Metastatic Mucosal Melanoma Patient with a Long-Term Response, International Journal of Clinical Case Reports and Reviews, 24(3); DOI:10.31579/2690-4861/725
Copyright: © 2025, Marina Sierra-Boada and Salvador Martín-Algarra This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 February 2025 | Accepted: 17 March 2025 | Published: 24 March 2025
Keywords: mucosal melanoma; immune checkpoint inhibitors; radiology; hepatic calcifications
A man in his 50s with a diagnosis of localized melanoma of the nasal mucosa with progression to liver and lung nodes. He received immune checkpoint inhibitor-based treatment, and after a sustained complete metabolic response, the CT scan showed some residual hepatic calcified lesions as a symbol of maintained response.
A man in his 50s with a diagnosis of localized melanoma of the nasal mucosa, treated by excision of the lesion and partial maxillary surgery, was referred to our service one month later due to hepatic progression detected on computed tomography (CT) (Figure. Panel A1-2) performed as a result of mild abdominal symptoms during adjuvant radiotherapy.
Treatment with ipilimumab-nivolumab within a phase I clinical trial (CA209038) was initiated by the end of 2014.
A CT scan performed after three cycles of treatment, revealed a clear increase in the size and number of liver lesions (Figure. Panel B1-2) and multiple new lung nodules. Liver function tests were normal. According to the protocol, the fourth cycle was administered as scheduled, and a new CT scan was planned six weeks later, during nivolumab monotherapy.
A month and a half later, CT scan showed a partial response (Figure. Panel C1-2). At the same time, the patient began to develop cutaneous vitiligo, which spread over a few months to the upper trunk and generalized to the whole body.
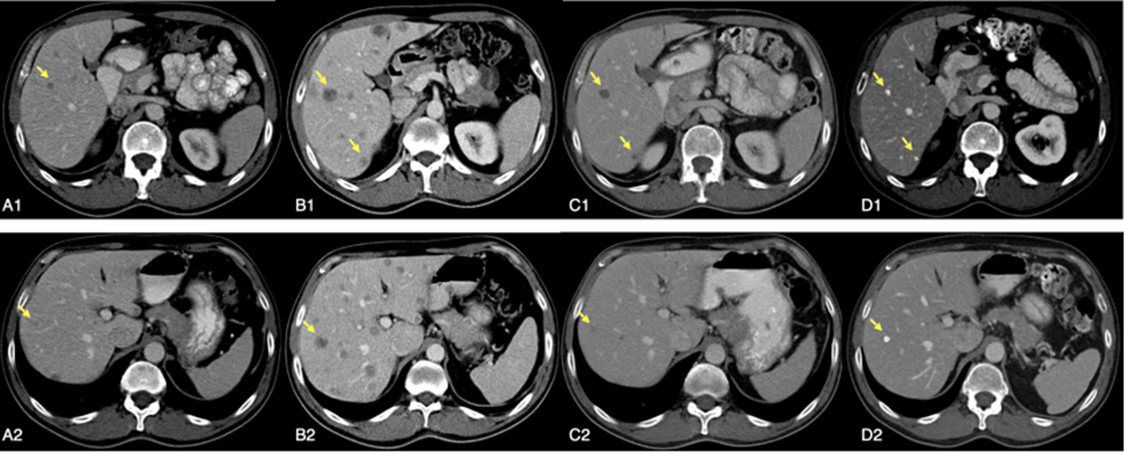
Figure 1: Sequence evolution of two CT scan slices of some hepatic metastases.
A1-2; basal imahe. B1-2; pseudoprogression afret three cycles of treatment. C1-2; partial response. D1-2; calcification of liver metastases 87 months after stopping treatment.
A PET/CT at the end of 2016, confirmed a complete metabolic response of all lesions. He continued treatment with good tolerability and radiological stability until completing 2 more years of treatment, about 4 years from the beginning, when nivolumab treatment was stopped. Subsequent CT studies during the follow-up were reported as “stable residual lesions of indeterminate significance”, undetectable by PET.
Early 2024, the patient maintains a fully active life in excellent state of health, and the CT scan report described and unchanged residual calcified hepatic punctiform nodules (Figure. Panel D1-2 and Video.) with no other evidence of residual melanoma, 87 months after stopping treatment.
The treatment landscape of metastatic melanoma has changed radically in recent years with the introduction of immune checkpoint inhibitors (ICI) and targeted therapies[1]. The most updated long-term follow-up data published so far with the combination of nivolumab and ipilimumab, show median overall survival of 72 months [2]. In spite of that, it is well-known that non-cutaneous forms of melanoma, including mucosal, usually have worse prognosis[3].
This case highlights not only the fact that aggressive mucosal melanomas may respond to ICI, particularly to the combination of ipilimumab and nivolumab, and achieve long term survival as their cutaneous counterpart, but also that the tumor response may be manifested also as residual calcified lesions, a well-known sign of long-term durable response in other tumors [4].
The differential diagnosis of hepatic calcifications has been, and remains, a diagnostic challenge for radiologists. The wide spectrum of diseases from neoplastic origin to other causes, including cystic, autoimmune, infectious (bacterial, viral, fungal or parasitic) lesions, makes it difficult to establish an accurate diagnosis. Besides that, to the best of our knowledge, there is no clear protocol to follow-up in this situation. Nor additional radiologic studies such as ultrasound, magnetic resonance or
PET/CT, neither interventional procedures, such as fine needle aspiration or biopsy, have been proposed so far as an adequate procedure to attain a definitive diagnosis.
A completed and detailed information to the patient, as well as a close follow-up using the best clinic-radiological criteria, was considered the most sound and appropriate way to reach a conclusion in this case, that currently seems to be no other than a sign of tumor remission.
The long follow-up in the absence of clinical or analytical data suggestive of other diagnosis, suggest that hepatic metastases calcification may also be a sign of maintained response after ICI based therapy. This cause, in our view, must also be included in the future reviews of the differential diagnosis of calcified hepatic lesions[5-6].
If that is the case, future consensus in this field may allow clinicians and radiologists not only to establish better follow-up strategies, but also to contribute to define better and most cost-effective ways to improve the management of the growing number of ICI treated cancer patients.
The progressive development of calcified lesions in liver metastases as a sign of response after ICI based therapy, should be included in the algorithms for evaluating the spectrum of disease with calcified hepatic lesions.
This situation could also be observed in other tumors treated by immunotherapy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
