
Review ariticle | DOI: https://doi.org/10.31579/2690-1919/521
Department of Otorhinolaryngology, Head and Neck Surgery; Saarland University, Homburg, Germany.
*Corresponding Author: Silke Wemmert, Department of Otorhinolaryngology Kirrberger Strasse 100; 66421 Homburg, Germany.
Citation: Bernhard Schick, Lukas Pillong, and Silke Wemmert, (2025), The Embryological Basis of Juvenile Angiofibroma: A Unifying Hypothesis for Tumor Pathogenesis, J Clinical Research and Reports, 19(5); DOI:10.31579/2690-1919/521
Copyright: © 2025, Silke Wemmert. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 March 2025 | Accepted: 08 April 2025 | Published: 30 May 2025
Keywords: juvenile angiofibroma; embryology; first branchial arch; neural crest cell; LH/LHR; epithelial-mesenchymal transition
Juvenile angiofibroma (JA) is a rare tumor, primarily affecting adolescent males, with an unclear etiology. This study reviews clinical and molecular data to assess an embryological hypothesis explaining JA's key features: its origin near the sphenopalatine foramen, vascular supply from the maxillary artery, sex-specific incidence, and fibrovascular composition. Findings support the hypothesis that JA arises from remnants of the first branchial arch plexus and persisting neural crest cells, which accounts for its location, blood supply, and growth. The hormonal surge during puberty, acting via the luteinizing hormone receptor, likely triggers tumor development. Epithelial-mesenchymal transition (EMT) is involved in its fibrous component. This hypothesis integrates JA's clinical, histopathological, and rare variant characteristics, suggesting an embryologically derived pathology.
Juvenile angiofibroma (JA) is a rare yet fascinating fibrovascular tumor defined by four distinct features: [1] an origin near the sphenopalatine foramen, [2] a primary blood supply from the maxillary/sphenopalatine artery with potential additional feeders from the internal carotid artery, [3] an almost exclusive manifestation in male adolescents, and [4] a fibrovascular architecture characterized by irregular vascular spaces - often lined solely by endothelial cells - embedded within a fibrous stroma (Schick & Kahle, 2000). These unique characteristics have spurred numerous theories regarding the tumor’s nature since the 19th century (Schick & Urbschat, 2004). However, most of these hypotheses have focused on only one aspect of JA, thereby neglecting the full spectrum of its features and ultimately failing to achieve general acceptance.
Historically, many proposed theories have concentrated on either the vascular or fibrous components of JA. This piecemeal approach risks an incomplete understanding of the tumor’s etiology, as it overlooks the interplay between both tissue components. In parallel, extensive genetic and molecular investigations - such as the frequent detection of beta-catenin mutations in JA - have identified various alterations without providing decisive insights into tumor etiology (Abraham et al., 2001; Calanca et al., 2021; Schick et al., 2011).
Moreover, these genetic and molecular studies have not identified a definitive tumor cell of origin, a crucial step for establishing a convincing etiological model. The absence of a clear explanation for the tumor’s almost exclusive occurrence in adolescent males further underscores the limitations of previous approaches; hormone studies, for instance, have yielded conflicting results (Kumagami, 1993; Liu et al., 2015; Schick et al., 2014).
In response to these challenges, a strong impetus is to adopt a unifying theory of JA nature. Here, we present an embryological perspective that, for the first time, simultaneously accounts for all four characteristic features of JA. This model integrates the vascular and fibrous elements of the tumor and offers a comprehensive explanation for its pathogenesis, thus holding the promise of achieving general acceptance.
Start of Embryological Thoughts in JAs
Two key developments initiated the embryological perspective on juvenile angiofibroma:
First Branchial Arch Artery
The first branchial arch artery is transiently present during embryonic development (days 22 to 24). It provides the essential blood supply to the developing brain during this period, while the later needed arteries are not yet fully established (Bertulli & Robert, 2021; Schick & Urbschat, 2004). Notably, the first branchial arch artery forms a temporary connection between the tissues surrounding the future sphenopalatine foramen and the segment of the internal carotid artery from which internal carotid feeders in JA are sometimes observed. As development proceeds, this artery regresses via the formation of a vascular plexus, with remnants of this plexus subsequently being incorporated into the arteries around the sphenopalatine foramen (Schick & Urbschat, 2004). Figure 1 a-d illustrates the normal development of the first branchial arch artery, along with the potential remnants of its plexus.
Previous findings have further illuminated the presence of exclusively endothelial-lined vascular spaces in fetal tissues adjacent to the sphenopalatine foramen in both sexes (Harrison, 1987). These spaces are hypothesized to represent regression remnants of the first branchial arch artery plexus, which may, in rare instances, persist and provide the anatomical basis for later JA development. In this context, it would be interesting to investigate whether extranasopharyngeal angiofibroma reflects embryonal remnants of other branchial arches, or also represents spreaded remnants of the first branchial arch.
Verification of Embryological Tissue
Based on the embryological hypothesis, specific markers indicative of an embryological origin should be detectable in JA tissues. Molecular analyses have primarily focused on the pathological JA vessels. Notably, laminin alpha2 expression was identified in these vessels (Starlinger et al., 2007), a marker typically expressed in embryonic vessels associated with the brain. This finding strongly supports the embryological origin hypothesis for JA. Additionally, an embryological collagen I texture has been observed in the fibrous component of JA (Gramann et al., 2009), further reinforcing this notion.
Moreover, the detection of TSHZ1 in JA vessels (Schick et al., 2011) has provided additional support for the involvement of the first branchial arch artery in JA pathogenesis. TSHZ1 is known to play a role in the formation of the first and second branchial arch arteries in mice (Coré et al., 2007), thereby renewing interest in its potential role in JA.
Cell of Tumor Origin
For many years, attempts to define the tumor cell of origin in JA have been unsuccessful. The embryological hypothesis offers a new perspective, guided by two key considerations: a) the persistence of neural crest cells in pathologies of embryological origin, and b) the critical role of neural crest cells in vascular development (Ponzoni et al., 2022; Schussler et al., 2021).
A particularly compelling observation is the consistent detection of CD271-positive cells in all examined JA samples, localized near the irregular vascular structures. These CD271-positive cells were interpreted as persisting neural crest cells, further supporting the concept that JA originates from embryological remnants (Schick et al., 2022).
Tumor Initiation
The almost exclusive manifestation of JA in adolescent males has long suggested a hormonal influence in its initiation. Initial studies, however, did not find altered hormone levels in affected individuals (Kumagami, 1993). Consequently, research shifted to investigating hormone receptors -primarily androgen, estrogen, and progesterone receptors (Liu et al., 2015; Schick et al., 2014). Yet, these studies yielded contradictory results, leaving the explanation for the tumor’s sex specificity unresolved.
The subsequent detection of luteinizing hormone receptor (LHR) mRNA in JA (Schick et al., 2014) expanded the perspective. Although LHR expression is typically limited to a few tissues, its presence in JA was striking. A closer examination revealed that the pubertal surge in luteinizing hormone (LH) - which marks the onset of puberty - could serve as a potent stimulus for tumor growth in male adolescents. Further investigations visualizing both LHR mRNA and protein in JA tissue sections consistently demonstrated LHR expression in proximity to the pathological vessels (Wemmert et al., 2024), supporting the hypothesis that the pubertal LH surge plays a critical role in JA initiation (Figure 1e).
Fibrovascular Tissue Architecture
The distinctive fibrovascular architecture of JA demands an explanation that integrates both its vascular and fibrous components. Within the context of an embryological vascular origin, the process of epithelial-to-mesenchymal transition (EMT) - a key embryological mechanism - emerges as a compelling candidate (Ang et al., 2023; Calanca et al., 2021; Serrano-Gomez et al., 2016). EMT provides a plausible mechanism by which the vascular component transitions into the fibrous tissue observed in JA (Figure 1g). This hypothesis is further supported by the expression of EMT-associated markers in JAs such as MMP3, PDGFRβ, NG2, and vimentin (Boewe et al., 2022; Schick et al., 2022), as well as transcription factors like Snail and Twist (own unpublished data).
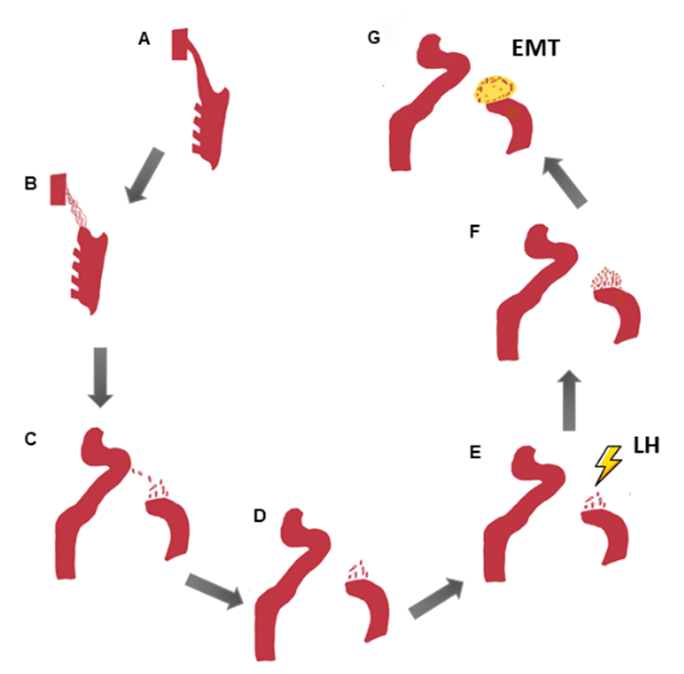
Figure 1: Embryological explanation for the characteristic vascular and fibrous features of JA. The first branchial arch artery ensures in embryology between day 22 and 24 blood supply for the developing brain in a still not completely developed internal carotid artery (a). The only temporarily present first branchial arch artery recedes via plexus formation in further development (b). The plexus remnants are found along the first branchial arch artery (c). Finally, they are only observed close to the area of the later sphenopalatine foramen (d) and incorporated partially into the arising vessels in this region. LHR-expressing remnants of the first branchial arch artery plexus are sensitive to an LH increase during puberty (e), resulting in vascular growth at this time (f) and tumor occurrence. Fibrous tissue arises (yellow) from the vascular component of the tumor by epithelial-mesenchymal transition (EMT)(g).
Tumor Localization
The endonasal approach is highly effective for resecting JA because it provides direct access to the sphenopalatine foramen and the altered vascular structures in this region. Complete tumor removal should include potential plexus remnants near the sphenoid foramen, the pterygoid plate, and the basissphenoid, thereby reducing the risk of recurrence (Howard et al., 2001).
Vascular Supply
In regard to JA embryological origin, it is essential to perform comprehensive angiographic evaluations of both the external and internal carotid arteries. Such assessments help to delineate the entire tumor blood supply and are critical in avoiding cerebral complications during embolization procedures. Moreover, the embryological perspective may also account for scarce, atypical JA locations (Windfuhr & Vent, 2018) where persistent vascular structures, akin to first branchial arch artery remnants, might be the origin.
Sex Specificity
The proposed involvement of LH in JA initiation not only explains the tumor’s prevalence in adolescent males but also provides insight into its occasional occurrence in early childhood (Newman et al., 2023). Known minor LH peak during early childhood could stimulate sensitive vascular remnants leading to JA formation (Bridges et al., 1994, Wu et al., 1990). Additionally, clinical observations indicate that anti-androgen therapy results in some tumor shrinkage in post-pubertal patients but not during puberty at the time of elevated LH levels (Sitenga et al., 2022), supporting the idea that LH is the dominant hormonal driver during puberty.
Fibrovascular Tissue
Histological analyses of JA reveal a transition from densely vascularized areas beneath a pseudo-capsule to regions dominated by fibrous tissue - a pattern consistent with EMT. This observation substantiates the clinical recommendation to avoid biopsies (due to the risk of abundant bleeding) and instead perform resection along the pseudo-capsule. In some cases, tumor involution may occur if the vascular remnants cease proliferating (Tosun et al., 2008), which aligns with the proposed EMT-based mechanisms.
Embryological JA Nature
The embryological hypothesis for JA is robustly supported by multiple lines of evidence that collectively address its unique features. The transformation of vascular tissue into fibrous tissue via EMT accounts for the tumor’s dual histological components. Furthermore, the identification of LHR in JA provides a plausible explanation for the near-exclusive manifestation in adolescent males, correlating with the pubertal LH surge (Schick et al., 2014; Wemmert et al., 2024). Finally, the detection of persisting neural crest cells and TSHZ1 in JA tissues (Schick et al., 2022; Schick et al., 2011) strongly supports the notion that the tumor arises from remnants of the first branchial arch plexus, thereby explaining its site of origin and characteristic blood supply. Functional analyses and single-cell RNA-seq will help to further elucidate the cell of origin and to follow the transitions.
Integrating developmental biology, molecular markers and clinicopathological features, our hypothesis differs from previous fragmented theories addressing vascular malformations or hormonal triggers in isolation, providing a comprehensive and unifying explanation for JA pathogenesis.
The authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
