
Research Article | DOI: https://doi.org/10.31579/2578-8965/006
Department of Neuropsychiatry, Faculty of Medicine, Tanta University, Egypt.
*Corresponding Author: Mohamed MK, Department of Neuropsychiatry, Faculty of Medicine, Tanta University, Egypt.
Citation: Gad NM , Dawood AS , EL-Gharib MN , Mohamed MK. The Effects of Selective Serotonin Reuptake Inhibitor (sertraline) on Premenstrual Tension Syndrome. J.Obstetrics Gynecology and Reproductive Sciences, 2(1); doi. 10.31579/2578-8965/006
Copyright: © 2018 Mohamed MK. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 March 2018 | Accepted: 09 April 2018 | Published: 11 April 2018
Keywords: Electroencephalogram, premenstrual dysphoric disorder, premenstrual stress, premenstrual syndrome, selective serotonin reuptake inhibitors, sertraline
Background: Premenstrual dysphoric disorder (PMDD) is a severe form of premenstrual syndrome (PMS).
Aim: To examine the effect of selective serotonin reuptake inhibitor (sertraline) on electroencephalographic (EEG) patterns, and clinical manifestations in females with PMS.
Materials and Methods: This prospective observational study was conducted on 200 females. Patients will be subdivided into two groups: Group A (control): includes 80 normal females and Group B consists of 120 patients with PMS. Patients with PMS were given sertraline 50 mg/day orally, initiated 14 days before the expected onset of menses and discontinued the day menses began.
Results: We found that sertraline has no substantial effects on EEG findings, simply it relieved the clinical symptoms.
Conclusions: We recommend use of SSRIs in the treatment of PMS
Premenstrual syndrome (PMS) is determined as a combination of physical and mood disturbances that take place in the last half of a woman's menstrual cycle after ovulation which normally ends with the menstrual flow. Premenstrual dysphoric disorder (PMDD) is a serious kind of premenstrual syndrome. PMDD occurs in 3% to 8% of menstruating women [1].
Epidemiologic surveys have estimated that 75 percent of women of reproductive age, experience some symptoms attributed to the premenstrual phase of the menstrual cycle. Most adult females able to treat these symptoms through lifestyle changes and conservative therapies [2].
The American Psychiatric Association has established formal guidelines for the diagnosis of PMDD in their Diagnostic and Statistical Manual (DSM-IV). The DSM-IV diagnostic criteria of PMDD require prospective documentation of symptoms being present for at least two consecutive menstrual cycles. At least one affective and one somatic symptom must exist and symptoms are relieved within 4 days without recurrence until cycle day 13[3].
Some EEG study of adult females with PMS demonstrated that Frontal EEG asymmetry was recorded at rest and during affective picture viewing, once during lateral and once during follicular phases, in counterbalanced order [4]. El-Gharib and associated concluded that that resting luteal phase of EEG frontal asymmetry must be added to the research criteria for PMDD (DSM-IV-TR) [5].
Serotonin is a monoamine neurotransmitter. Biochemically derived from tryptophan, serotonin is primarily found in the gastrointestinal tract, blood platelets, and the cardinal nervous system. It is popularly thought to be a contributor to feelings of well-being and happiness [6].
Evidence implicates the serotonergic system, in particular in the pathogenesis of premenstrual dysphoric disorder, which is considered to be associated with symptoms such as irritability, depressed mood, and carbohydrate craving [7].
Selective serotonin reuptake inhibitors (SSRIs) are considered to increase the extracellular levels of the neurotransmitter serotonin by inhibiting its reuptake into the presynaptic cells and thus increasing the measure of serotonin available to attach to the postsynaptic receptor. SSRIs are most usually used as antidepressants and anxiety disorders [8]. Numerous studies with a double-blind, randomized, confirm that SSRIs improves the quality of life of women with PMDD [9].
The hypotheses of this work is to study the effect of Selective Serotonin Reuptake Inhibitors on electroencephalographic patterns, and clinical manifestations in females with premenstrual tension syndrome.
This prospective observational cohort study was conducted on 160 women from those serving the Department of Obstetrics and Gynecology, Tanta University Hospital. Recruitment of the chess sets out in November 2015 and was finished in July 2016.
The two hundred patients included in this open area, subdivided into two groups: Group A (control): includes 80 normal females and Group B (patient): includes 120 patients with premenstrual tension syndrome.
All patients were included in the study was less than 35 years old, have a BMI between 20 and 30, having regular cycles, not using drugs (particularly ovulatory induction drugs, hormonal contraception, serotonin reuptake inhibitors and other drugs affecting CNS) during the last six months, do not cause neurological or psychiatric problems, if they owned a previous operation of the brain or spinal cord.
All patients submitted to the study were counseled thoroughly about the procedure including nature, value, and fates of the investigation and the aim of the study. After this, a written consent will be obtained and signed by the patient. We did not receive any funds, from any individual or organization. If the patient refused to complete the study, she was contracted away and replaced by another one from who are satisfying the inclusion criteria of the study. We did not classify the patients according to their religious belief or culture or race or any other inside information.
At one time women were admitted into the study, they were asked about their current phase of the cycle, by calculating backward from the starting day of the next expected period. PMDD was diagnosed by the daily symptom report [10].
Patients with PMS were given sertraline 50 mg/day orally, initiated 14 days before the expected onset of menses and discontinued the day menses began.
The Following methods were attempted for each patient:
Firstly, we prepared and clean the scalp of the patient from oil and any debris or draft, then 21 sliver-chloride electrodes were applied to the head surface and they were adherent to the scalp by using an adhesive conductive paste (10-20 paste). These electrodes were put on to the scalp according to 10-20 system. Hyperventilation and photic stimulation were applied as provocation methods during EEG recording. These signals from the surface electrodes will pass through an amplifier that converts them from parallel to digital ones which can be displayed and stored in a computer [11].
EEG was performed twice for each patient, firstly, on the 7th day of the cycle (follicular phase) and secondly on day 21 of the cycle (luteal phase).
Statistical analysis of data was performed by the IBM SPSS statistics program version 20. The value of P < 0>
The results of this study are pictured in 6 tables and 5 figures.
| Number | Range | Mean | ±SD | ||
| Age | Control group | 80 | 20-35 | 27.525 | 4.7447 |
| PMS group | 120 | 21-34 | 27.325 | 4.6233 | |
| BMI | Control group | 80 | 22-28 | 25.075 | 2.0049 |
| PMS group | 120 | 21-27 | 25.025 | 2.0231 | |
Table (1): Age and body mass index of the studied patients.
Table (1) shows the historic period and body mass index of the analyzed cases. The control and patient group were well seen.
Table (2) depicted the reproductive characteristics of the study group. There was a significant relation between the folk history of PMDD and the occurrence of the disease.
| Variables | With PMS/ MDD (120) | Without PMS/ PMDD(80) | t. test or X2 | P. val ue |
| Present age (in years) | 27.3 ± 4.985 | 27.75 ± 4.61 | 0.6349 | 0.2241 |
| Age at menarche (in years) | 13.05 ± 1.395 | 13.3 ± 1.455 | 0.4751 | 0.8519 |
| Number of bleeding days | 5.9 ± 1.165 | 5.7 ± 1.129 | 1.3248 | 0.1141 |
| Lengthof cycle (in days) | 26.65 ± 2.455 | 25.85 ± 2.641 | 1.9651 | 0.2239 |
| Number of years withPremen strual Symptoms | 3.3 ± 0.801 | 3.25 ± 0.786 | 0.8589 | 0.9511 |
Dysmenorrhea: Yes No | 10 18 | 56 24 |
2.0411 |
0.1519 |
TheIntensity of dysmenorrhea Mild Moderate Severe |
78 30 12 |
40 28 12 |
0.621 |
0.7321 |
Family history: Yes No | 108 12 | 48 32 |
5.149 |
0.024 |
Table (2): Reproductive characteristics of study subjects

Figure (1): The frequency of symptoms among subjects with premenstrual tension syndrome.
| Number of patients | No of Abnormal EEG | % | |
| PMS | 102 | 60 | 58.82 |
| PMMD | 18 | 6 | 33.33 |
Table (3): The Premenstrual symptoms in PMS / PMDD groups.

Figure (2): Premenstrual symptoms in PMS / PMDD patients, according to severity.
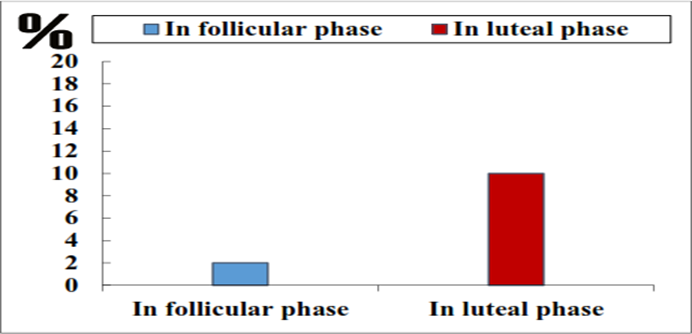
Figure (3): EEG patterns, ratio in premenstrual tension syndrome in patient during follicular and luteal phases
The main premenstrual symptoms were displayed in table 3 and figures 2 & 3, anxiety was the commonest symptoms.
| Mild | Moderate | Severe | X2 | P.value | ||||
| N | % | N | % | N | % | N | % | |
| Depressed, sad, “down”or “blue”feeling of worthless or guilty | 96 | 80 | 18 | 15 | 6 | 5 | 4.2529 | 0.0151 |
| Anxious, tense, “keyedup” or on edge | 108 | 90 | 6 | 5 | 6 | 5 | 2.6319 | 0.0511 |
| Mood swings/sensitiveto rejection | 84 | 70 | 24 | 20 | 12 | 10 | 7.5261 | 0.0489 |
| Anger, or irritable | 84 | 70 | 12 | 10 | 24 | 20 | 2.6321 | 0.0949 |
| Less interest in usualactivities | 102 | 85 | 36 | 5 | 12 | 10 | 5.4119 | 0.0091 |
| Lack of concentration | 72 | 60 | 24 | 20 | 24 | 20 | 3.1471 | 0.0279 |
| Lethargic, tired, fatiguedor of energy | 60 | 50 | 48 | 40 | 12 | 10 | 152 | 0.147 |
| Increased appetite orfoodcravings | 72 | 60 | 42 | 35 | 6 | 5 | 1.2011 | 0.3319 |
| Insomnia/hypersomnia | 54 | 45 | 54 | 45 | 12 | 10 | 0.3019 | 0.1141 |
| Overwhelmed, unable tocope | 78 | 65 | 18 | 15 | 24 | 20 | 2.8851 | 0.0159 |
Breast tenderness, breastswelling, bloatedsensation, weight gain,headache, joint or muscle pain, or otherphysical symptoms | 8 | 40 | 60 | 50 | 12 | 10 | 4.5229 | 0.0271 |
Reduction of productivity or inefficiency at work,school, homeor in dailyroutine | 14 | 70 | 12 | 10 | 24 | 20 | 5.6389 | 0.021 |
| Less participation inhobbies or socialactivities | 11 | 55 | 36 | 30 | 18 | 15 | 2.031 | 0.0119 |
| Interference in relationships with others | 17 | 85 | 6 | 5 | 12 | 10 | 2.3359 | 0.0741 |
Table (4): Comparison between EEG finding in PMS and PMDD cases
| PMS | PMDD | |
| Background activity | 0 | 0 |
| Sharp and slowwave activity | 12 | 0 |
| Spike and slow waveactivity | 0 | 0 |
| Slow wave activity | 0 | 0 |
| Frontal discharge asymmetry | 48 | 6 |
Table (5): Abnormal EEG finding in study group.

Figure (4): The abnormal EEG finding in study group.
Approximately 58% of patients with PMS has normal EEG findings compared with approximately 33% of cases with PMMD (tables 4-5, figure 4).
| Number | Get better | |
| Abnormal EEG | 60 | 36 |
Table (6): The Effects of Selective Serotonin Reuptake Inhibitors on EEG Findings in Females with Premenstrual Tension Syndrome.
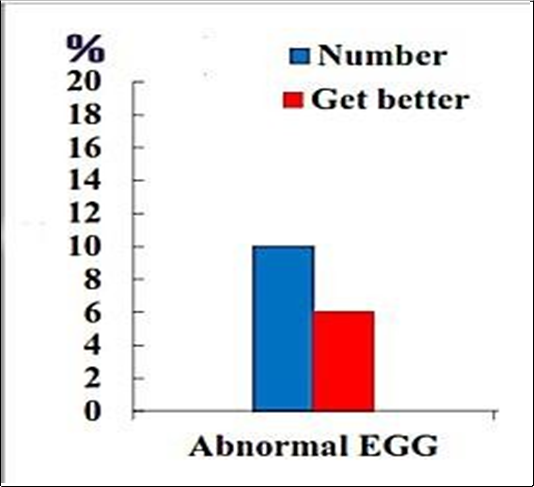
Figure (5): The Effects of Selective Serotonin Reuptake Inhibitors on EEG Findings in Females with Premenstrual Tension Syndrome.
EEG findings were set at 60% with sertraline therapy (table 6 and figure 5). Figure (1) displays EEG patterns, ratio in premenstrual tension syndrome in patients during the follicular and luteal phases.
The contemporaneous study showed a substantial difference in frontal alpha asymmetry between PMS and non-PMS women and a difference between right and left hemisphere alpha activities in the luteal phase. In increase, negative affect and somatic depression were related to frontal alpha asymmetry. In that location were more severe premenstrual distress and depressive symptoms during the luteal phase than during the follicular phase, as well as more severe premenstrual distress and depressive symptoms in PMS than in non-PMS (Tables 1-3 & Figures 1-3).
In judgment with previous studies, (4) the present work examined the participants' EEG not only below the resting baseline, but also during the depressive induction and relaxation conditions. Agreeing to the Davidson's theory, frontal alpha asymmetry reveals relatively higher left than right frontal alpha activity during depressive moods in major depressive disorders.
Furthermore, Baehr et al. & Accortt et al., [12] also confirmed higher left than right frontal alpha activity under the resting baseline in a diagnostic PMDD group. The finding of this study and those of the previous studies concur that frontal alpha asymmetry significantly differed between PMDD and non-PMDD.
All the participants of the present survey are of childbearing age and experienced regular menstrual cycles. We propose that the difference found in frontal alpha asymmetry may be made by one of the pathophysiological mechanisms underlying PMS. This concurs with the findings of Davidson [13] who indicated that frontal alpha asymmetry was related to metabolic activity in the amygdala (part of the limbic system), which was connected to emotion regulation.
In the existing study, we found no substantial correlation between EEG findings and the clinical manifestation of PMS (Tables 4-6 & Figures 4-5).
Numerous treatment modalities have been proven to be efficacious in the treatments of PMS, and counseling, including psychotherapy, medications as SSRIs (selective serotonin reuptake inhibitors). SSRIs are the most effective medication available at the present for treating PMDD, hormonal therapies, including oral contraceptive pills, danazol, GnRh analogue, progesterone, progestagens and surgical removal of the ovaries [14].
Selective serotonin reuptake inhibitors (SSRIs) are currently considered the most effective pharmacologic class for the treatment of symptoms related to severe premenstrual syndrome (PMS) and it’s most intense form, premenstrual dysphoric disorder [15]. Despite the conduct of systematic reviews supporting SSRI efficacy, sources of heterogeneity between studies have not been elucidated in prior meta-analyses [16].
The SSRIs, including sertraline, represent an important advance in the pharmacotherapy of mood and other disorders. They are chemically unrelated to tricyclic, heterocyclic, and other first-generation antidepressants. SSRIs are the treatment of choice for many indications, including premenstrual dysphoric disorder, because of their efficacy, good side-effect profile, tolerability, and safety in overdose, as well as patient compliance [17].
In the current study, we gave sertraline drugs for treating cases with PMDD in a dose of 50 mg once daily starting from the 14th days till menstruation occurred, for 3 cycles. We found amelioration of symptoms in 60% of cases. These results come to an agreement with the results of several authors [18-20].
Opportunely, we did confront with any side effects to sertraline administration. This differs from the results of other authors [21, 22].
To finish, we conclude that sertraline is an effective medicament for PMDD.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
