
Case Report | DOI: https://doi.org/10.31579/2690-4861/366
1 Associate Professor Department of Anesthesia & Perioperative Care, University of California, San Francisco, CA.
2 Adjunct Assistant Professor Department of Surgical Neurophysiology, University of California, San Francisco, CA.
3 Assistant Professor Department of Anesthesiology and Pain Medicine, University of California, Davis, Sacramento, CA.
4 Cardiac Anesthesiologist CASE Anesthesia Group, Sacramento, CA.
5 Professor Department of Anesthesia & Perioperative Care, University of California, San Francisco, CA.
*Corresponding Author: Andrew E. Schober, MD 521 Parnassus Avenue #4310 UCSF Department of Anesthesia and Perioperative Care San Francisco, California, USA.
Citation: Andrew E. Schober, John P. Clark, Amy Chen, Steven Hur, Jeremy A. Lieberman (2024), The Effects of High-Dose Ketamine on Motor Evoked Potential Monitoring in Patients with Myelopathy: A Case Series, International Journal of Clinical Case Reports and Reviews, 16(2); DOI:10.31579/2690-4861/366
Copyright: © 2024, Andrew E. Schober. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 December 2023 | Accepted: 15 January 2024 | Published: 26 January 2024
Keywords: ketamine; neuromonitoring; evoked potentials; meps; myelopathy; case series
Motor Evoked Potentials (MEPs) allow for real-time monitoring of the corticospinal tracts during spine surgery. MEPs can be difficult to obtain in patients with cervicothoracic myelopathy. We describe 5 myelopathic patients undergoing spine surgery with insufficient MEPs on a standard propofol-based anesthetic. Conversion to high-dose ketamine (20 mcg/kg/min) with other minimally suppressive agents resulted in signal enhancement in a majority (36 of 63) of muscle groups with adequate anesthesia and minimal adverse effects, although with considerable variability in the durability of this effect. High-dose ketamine appears to be a safe and viable option to attempt to augment poor baseline MEP signals.
ALIF: anterior lumbar interbody fusion
IONM: intraoperative neuromonitoring
IRB: institutional review board
MEP: motor evoked potential
POD: post-operative day
PSF: posterior spinal fusion
SSEP: somatosensory evoked potential
UCSF: University of California San Francisco
Intraoperative neuromonitoring (IONM) is utilized during spine surgery to monitor the functional integrity of the spinal cord and nerve roots. Motor evoked potentials (MEPs) allow for real-time assessment of corticospinal pathways at risk for injury [1]. Anesthetic agents are chosen to maintain conduction along these pathways and optimize MEPs in order to detect evolving neural injury. Hypnotic agents, like propofol, and volatile agents tend to depress evoked potentials, with MEPs being particularly sensitive to suppression compared to somatosensory evoked potentials (SSEPs) [2, 3]. Other anesthetics, including benzodiazepines, lidocaine, and opiates, appear to have negligible effects on evoked potential responses [4]. Ketamine is a short-acting intravenous anesthetic agent which is increasingly being utilized as an adjunct in complex spine surgery due to its opiate-sparing and anti-hyperalgesic effects [5-7]. However, the reported effects of ketamine on MEPs are inconsistent [8-11].
Cervicothoracic myelopathy is a disease of the spinal cord that impairs motor and sensory function, which is reflected in the MEP and SSEP responses [12]. While measuring MEPs is more difficult in these patients, monitoring the integrity of the corticospinal tracts remains critical to avoid further injury, since the incidence of adverse neurologic outcomes following surgery is proportional to disease severity [12, 13]. Several case reports in pediatric patients with pre-existing myelopathy describe improvement in IONM with a ketamine-based anesthetic [14-16]. Low-dose ketamine (1-5 mcg/kg/min) appears to augment, or at least not depress, MEP amplitudes[8, 9]. However, high-dose ketamine may reduce MEP amplitudes in some situations [10, 11]. To our knowledge, no one has described the efficacy of a high-dose (> 10 mcg/kg/min) ketamine-based anesthetic to augment IONM in adult spine surgery patients with myelopathy.
We present a series of five patients with cervicothoracic myelopathy undergoing spine surgery where high-dose ketamine, in conjunction with other minimally suppressive anesthetics, was used to augment poor baseline MEPs. Waiver of written consent for this retrospective review was granted by the Institutional Review Board (IRB) at UCSF.
Five patients presented for spine surgery at the University of California San Francisco (UCSF) Medical Center due to cervicothoracic myelopathy. Pertinent medical history and surgical details for each patient are described in Table 1. In each case, initial MEP signals were determined to be unmonitorable on a standard propofol-based total intravenous anesthetic (TIVA) by the intraoperative neurophysiologist due to a lack of reproducible signals below the level of the lesion. An intraoperative wake-up test in the prone position was performed in Patients #1 and #3 to confirm intact gross motor function before proceeding.

Table 2 describes key characteristics of the intraoperative anesthetic and the effect of the high-dose ketamine (20 mcg/kg/min) anesthetic intervention on the MEPs for each patient. Conversion to a high-dose ketamine and opiate anesthetic allowed for substantial reduction in propofol in all cases. Since this reduction in propofol was not protocolized, the minimum propofol infusion rates varied (20-60 mcg/kg/min). In addition, the opiate adjunct varied at the discretion of the anesthesiologist. In all cases except one (Patient #4), ketamine infusions were initiated with a bolus. We further titrated the anesthetic to ensure the absence of burst suppression in the raw electroencephalogram (EEG) and based on clinical parameters to balance optimization of MEP signals with an adequate depth of anesthesia.
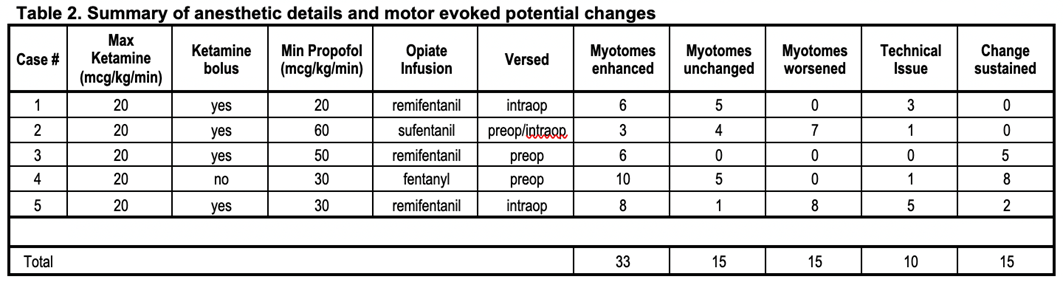
Given the severity of myelopathy, signals were generally of low amplitude and poor quality, making quantitative assessment of amplitude change challenging. Thus, MEP signals for each muscle group monitored were categorized as enhanced, unchanged, or worsened by qualitative comparison of the peak-to-peak amplitude before and after changing to a high-dose ketamine anesthetic. Of the 73 myotomes in which monitoring was attempted, technical issues (over-amplification and electrical interference) prevented accurate comparison in 10 myotomes.
After conversion to a high-dose ketamine anesthetic, all patients had some MEPs that were deemed monitorable below the level of the lesion by the neurophysiologist. Figure 1 displays an example of enhancement of MEPs from a single muscle group over time in Patient #3. The increase in peak-to-peak amplitude correlates with the initiation of ketamine and reduction of propofol. This augmentation degraded over time, which is typical of prolonged exposure to anesthesia.
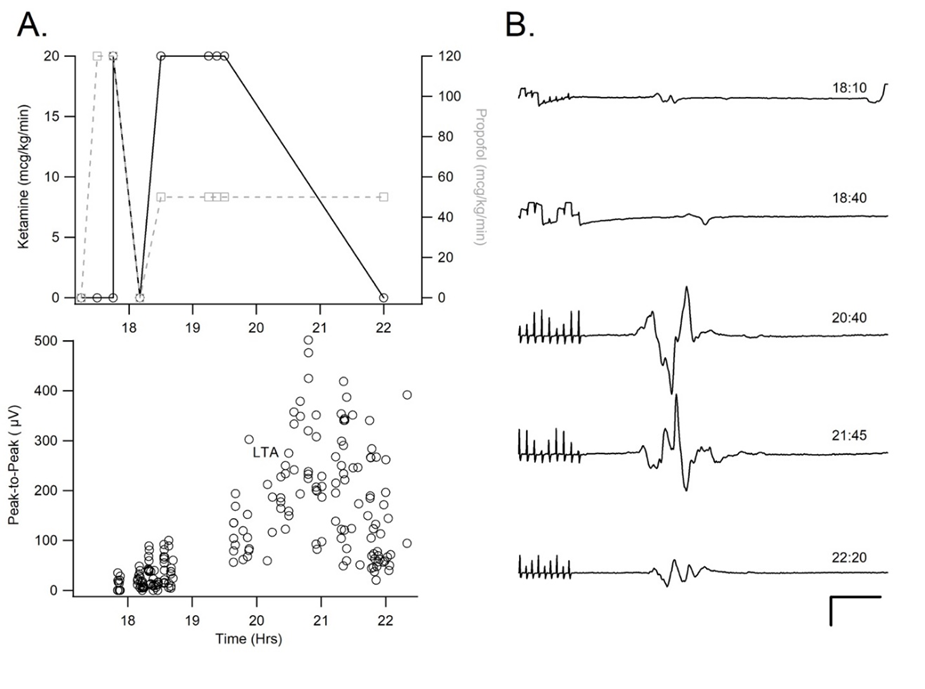
Figure 1: An example of anesthetic and motor evoked potential (MEP) data from the left tibialis anterior of patient #3. A. The dose of propofol and ketamine infusions (top) as well as peak-to-peak voltage measurements of the MEPs (below) are plotted over a 24-hour clock base (~17:00-23:00). B. Sample MEP tracings from the left tibialis anterior at various timepoints over the course of the surgical period (time bar: 100 mV, 20 ms). Both show enhancement during the change from standard total intravenous anesthetic (TIVA) to a high-dose ketamine anesthetic with reduction of propofol.
Despite the presence of some monitorable signal in each patient, the effects of this anesthetic change on individual MEP responses varied. In the 63 myotomes monitored over all 5 cases, 33 showed enhancement, 15 were unchanged, and 15 worsened after conversion to a high-ketamine anesthetic. In 3 patients (Patients #1, 3, and 4), MEPs showed enhancement in most recordings (22/32 muscles), while a minority were unchanged (10/32 muscles), and none worsened. In the remaining 2 patients (Patients #2 and #5), a minority of myotomes were enhanced (11/31 muscles), while the majority were either unchanged (5/31 muscles) or worsened (15/31 muscles). Of the 33 myotomes that enhanced, only 15 (45%) were sustained for the remainder of the monitoring period.
Adverse effects were minimal. 3 of 5 patients were extubated in the operating room. Two patients remained intubated for airway protection. Patient #1 initially failed a cuff leak test but was extubated uneventfully on post-operative day (POD) #2 once facial edema and the cuff leak improved. Patient #5 remained intubated for airway concerns, given the extent of the fusion to the occiput, but was extubated uneventfully on POD#1 once airway patency was confirmed by CT scan and fiberoptic laryngoscopy / bronchoscopy. Both patients had a monitorable neurologic exam post-operatively while intubated. One patient experienced mild, transient hallucinations. None of the patients reported intraoperative recall and none suffered from significant delirium.
Effective IONM in the anesthetized myelopathic patient can be challenging. Standard anesthetic techniques may be incompatible with obtaining adequate MEP responses. In the cases presented, high-dose ketamine, in conjunction with an opiate and a lower-dose propofol anesthetic, was used as an alternative to more typical anesthetic regimens for severely myelopathic patients when MEP amplitudes were otherwise unmonitorable. This case series shows that using high-dose ketamine as part of a balanced anesthetic is safe and well-tolerated but also may be effective in myelopathic patients undergoing spine surgery.
Conversion to a high-dose ketamine anesthetic enhanced MEPs in a subset of myotomes that otherwise could not be monitored (33 of 63 myotomes). The most likely explanation is that the use of ketamine enabled a reduction in anesthetic agents that suppress MEPs, such as propofol [2]. While propofol may be less suppressive than volatile agents [3, 17], in patients with significant spinal cord compromise, consistently amnestic doses of propofol may be incompatible with obtaining reliable MEPs[12]. The use of alternative agents, in this case ketamine, may allow for adequate anesthesia so that propofol can be reduced or eliminated[18]. This is supported indirectly by the observation that the patient (#2) with the highest minimum propofol infusion rate compared to the other patients (60 mcg/kg/min vs. 20-50 mcg/kg/min) had the least improvement in MEPs. Alternatively, ketamine may augment MEPs by increasing cortical excitability through NMDA receptor antagonism and disinhibition of excitatory cortical neurons. This may allow for sufficient corticospinal tract signaling through the myelopathic spinal cord segment to produce MEPs, manifesting as decreased MEP thresholds [19].
While a subset of MEPs were deemed sufficient to proceed with surgery after initiation of high-dose ketamine (20 mcg/kg/min), the effect on individual myotomes was inconsistent. Different myotomes in the same patient showed considerable variability in the response to ketamine and the durability of this effect over time. Since high-dose ketamine was initiated as part of a complex, balanced anesthetic to rescue extremely poor baseline MEPs, the type and dose of the opiate infusion and other non-opiate analgesic medications were not controlled. In addition, the myotomes monitored and titration of evoked potential stimuli were not standardized, making it difficult to compare signal amplitude between patients and even over time within the same patient. Future controlled studies assessing the effects of ketamine on MEPs should aim to reduce the variability reported here and in other studies [10,11,20] by protocolizing anesthetic titration as well as standardizing evoked potential stimuli and waveform analysis.
Higher doses of ketamine are often avoided due to the perceived risk of psychomimetic effects, including hallucinations, dysphoria, and emergence delirium [21, 22]. In this series, there were minimal adverse effects attributable to the anesthetic aside from mild visual hallucinations experienced by Patient #5, which were transient and not distressing. This is consistent with work showing a lower incidence of adverse psychomimetic effects associated with ketamine when used in conjunction with low-dose propofol, as was done in this study [23]. While reliable amnesia may be a concern when propofol is substantially reduced, no patient experienced recall, despite performing a wake-up test in 2 patients. There did not appear to be a substantial increase in anesthetic duration or need for post-operative intubation. Both patients who remained intubated were able to participate in a neurologic exam in the immediate post-operative period. Thus, the balanced anesthetic combination described was generally well tolerated.
Based on our experience, high-dose ketamine should be considered in patients with cervicothoracic myelopathy undergoing complex spine surgery where there is high concern for injury to the corticospinal tracts and when MEPs are insufficient using traditional propofol-based regimens. Due to the increased potential for delirium and negative psychomimetic side effects, it would be premature to recommend this technique in the general spine surgery population without further prospective, controlled studies. Instead, it is the opinion of the authors that the potential negative effects must be weighed against the risk of neurologic injury undertaken by proceeding in the absence of adequate monitoring of MEPs. In the end, if there is some concern regarding the adequacy of IONM signals, a wake-up test should be considered. This is generally well tolerated, even in the prone position, and often without post-operative recall. Further study is needed to see if this anesthetic regimen is useful for other case types or patient populations, as the effect of high-dose ketamine may be different in patients without myelopathy.
In a small subset of patients with cervicothoracic myelopathy undergoing complex spine surgery, MEPs are unmonitorable using a standard propofol-based anesthetic. In this limited series, use of a high-dose ketamine-based anesthetic allowed monitoring of MEPs and enhanced MEP amplitude from a majority of muscle groups measured. Prospective, controlled studies are needed to further clarify the effects of high-dose ketamine on evoked potentials.
There are no additional supplementary materials included with this case series aside from the Table 1, Table 2, and Figure 1.
The authors declare no conflicts of interest
The authors declare no competing interests.
All authors had access to the data and a role in writing this manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
