
Research Article | DOI: https://doi.org/10.31579/2768-2757/077
1 Virginia Tech Carilion School of Medicine, Roanoke, VA
2 Department of Surgery, Section of Plastic and Reconstructive Surgery, Carilion Clinic, Roanoke, VA
*Corresponding Author: Nikitha Potturi, Virginia Tech Carilion School of Medicine, Roanoke, VA.
Citation: Matthew A. Applebaum, Nikitha Potturi, Stephanie Hamlin, Joo Won Choi, Kurtis E. Moyer, (2023), The Effects of Hemoglobin A1C on Complications in Implant-Based Breast Reconstruction, Journal of Clinical Surgery and Research, 4(3); DOI:10.31579/2768-2757/077
Copyright: 2023, Nikitha Potturi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 May 2023 | Accepted: 10 May 2023 | Published: 18 May 2023
Keywords: small cell carcinoma; esophageal carcinoma; small cell esophageal carcinoma
Background
Given the prevalence of diabetes and high complication rate of breast reconstruction, it is prudent to ascertain if there is an association between hemoglobin A1C levels and outcomes in patients undergoing implant-based breast reconstruction. This may help guide clinical decision making and also inform patients of their relative risk of complications.
Methods
A retrospective review of 203 patients that underwent implant-based breast reconstruction at a single institution was conducted. All patients required a documented pre-operative A1C. Patients were then categorized by A1C level into three groups: normal (<5.7%), prediabetic (5.7% to 6.4%), or diabetic (>6.5%). Patient demographics and postoperative complications were evaluated in relation to A1C values during both the initial tissue expander placement and subsequent exchange operations. Data was evaluated using a two-sample t-test for continuous variables, chi-squared for categorical variables and univariate logistic regression models were performed.
Results
203 patients were divided into normal (n=135), pre-diabetic (n=40), and diabetic (n=28) cohorts. Patients in the diabetic and pre-diabetic group were generally older (p=0.011), Caucasian (p=0.007), higher weight (p=0.002) with elevated BMI (p<0.001), and a higher percentage of hypertension (p<0.001). The prediabetic and diabetic groups had a higher percentage of overall complication rate (57.5% and 53.8% respectively), when compared to the normal cohort (31.3%) (p=0.003). The percentage of patients that sustained a loss of their tissue expanders was also increased in the prediabetic (10%) and diabetic groups (22.2%) (p= 0.029). The diabetic population was more likely to have a complication (OR=2.56, 95% CI [1.09,6.00]) and to have tissue expander loss (OR 4.5, 95% CI [1.42,14 .28]) after their tissue expander placement when compared to the normal population. There was no increased complications or tissue expander loss associated with A1C levels for the subsequent surgery for permanent implant placement.
Conclusion
Patients with elevated A1C are at an increased risk for overall complications and diabetic patients are at increased risk for tissue expander loss during the first stage of implant-based breast reconstruction. There were no associated risks for the implant exchange procedure. A preoperative hemoglobin A1C should be considered for patients seeking implant-based tissue expander breast reconstruction to discuss surgical risk.
Implant-based breast reconstruction, after mastectomy, is the most common type of reconstruction in the United States [1]. Despite its popularity, this treatment modality has been fraught with complications [2]. Given the high rates of complication, it is crucial for patients and providers to understand the relative risks of common pre-existing conditions to guide clinical decision making to mitigate the probability of these complications. Certain comorbidities such as obesity, hypertension, and tobacco use have been associated with increased risk of perioperative complications [3,4]. The American Diabetes Association (ADA) reports 37.7 million (11.3%) of Americans suffer from diabetes, and an estimated 38% of adults have prediabetes. This prevalence is expected to increase [5,6]. Poor glycemic control has been linked to increased rates of post-operative complications in various surgical specialties [7-10]. Whereas appropriate perioperative glycemic control, defined as hemoglobin A1C (A1C) <7%, is associated with decreased postoperative infections [11]. Additional studies demonstrate that elevated A1C is associated with poor wound healing after surgery and found that for every 1.0% increase in A1C, wound-area healing rate decreased by 0.028 cm² per day [12-15]. Given these associations, routine universal preoperative A1C testing has been initiated as a screening tool for patients undergoing elective joint replacement surgery [16-17]. The rationale is to identify patients with poorly controlled diabetes to intervene prior to surgery with optimization of their medical condition to limit higher surgical complication rates. This results in delaying the surgery for improvement of their glycemic index. Cancer patients, however, do not have the luxury of time for postponing surgery which would delay their care and potentially impact their outcomes. Certain surgeries demonstrated minimal impact of elevated A1C on outcomes with the recommendation to proceed with surgery as the surgical benefits outweighed the low risk of complications [18]. Given the increased prevalence of diabetes and high complication rate of breast implant reconstruction, it is prudent to ascertain the association between A1C and outcomes in patients undergoing implant-based breast reconstruction to guide clinical decision making and to inform patients of their relative risk of complications. We hypothesized that an elevated A1C would not affect complications in patients undergoing implant-based breast reconstruction.
An institutional review board-approved retrospective review was performed on patients that underwent implant-based breast reconstruction at a single institution between March 2013 and October 2020. Patients were selected using Current Procedural Terminology codes for tissue expander placement (19357) and tissue expander removal or replacement with a permanent implant (11970, 19328) by the surgeons involved in the study. A total of 203 patients were included in the analysis. All patients required a documented pre-operative A1C within three months of the operation. AIC levels are obtained on all general anesthesia cases, including non-diabetic patients, according to our hospital’s institutional policy. Chart review identified demographic information including patient age, BMI, history of hypertension, tobacco use, sentinel lymph node biopsy or axillary lymph node dissection at the time of operation, neoadjuvant or adjuvant therapies, pre-operative A1C level, and postoperative complications. Post-operative complications were defined as surgical site infection, development of seroma or hematoma, dehiscence requiring local wound care, dehiscence requiring operative intervention, exposure of prosthesis, and loss of prosthesis. Postoperative complications were evaluated in relation to A1C values during both initial tissue expander placement and subsequent exchange operations. Patients were categorized into cohorts by A1C level in concordance with the ADA as either normal (<5>6.5%)5,19. Statistical significance was evaluated using a two-sample t-test for continuous variables and a chi-squared for categorical variables. Unweighted univariate logistic regression models were estimated to obtain an odds ratio for the development of complications after tissue expander placement and after permanent implant placement. The effect size was measured for prediabetic and diabetic patients compared to patients with a normal A1C at a significance level of 0.05.
203 patients were divided into normal (n=135), pre-diabetic (n=40), and diabetic (n=28) cohorts. Demographics demonstrated that patients in the diabetic and pre-diabetic group were generally older (p=0.011), Caucasian (p=0.007), higher weight (p=0.002), elevated BMI (p<0.001), and a higher percentage of hypertension (p<0.001) when compared to the normal population cohort (Table 1). The pre-diabetic population had a higher percentage of preoperative radiation (n=11, 28.2%) due to previous treatment with breast conservation therapy and a new primary malignancy or recurrence (p=0.011).
| Characteristic | Overall | Normal <5> | Pre-Diabetic 5.7-6.4% | Diabetic ≥6.5% | p-value* |
| (N = 203) | (N = 135) | (N = 40) | (N = 28) | ||
| Patient Age (Years) | 0.011 | ||||
| n | 203 | 135 | 40 | 28 | |
| Mean | 52.86 | 51.6 | 55.89 | 54.65 | |
| SD | 10.09 | 10.07 | 7.47 | 12.39 | |
| Race, n (%) | 0.007 | ||||
| White | 173 (85.2%) | 120 (88.9%) | 35 (87.5%) | 18 (64.3%) | |
| Non-White | 30 (14.8%) | 15 (11.1%) | 5 (12.5%) | 10 (35.7%) | |
| Weight (LBS) | 0.002 | ||||
| n | 199 | 133 | 38 | 28 | |
| Mean | 175.04 | 167.26 | 194 | 186.25 | |
| SD | 44.43 | 41.67 | 48.4 | 42.93 | |
| BMI | <.001 | ||||
| n | 201 | 134 | 39 | 28 | |
| Mean | 29.72 | 28.35 | 32.58 | 32.31 | |
| SD | 6.85 | 6.24 | 7.44 | 7.06 | |
| Hypertension, N (%) | <.001 | ||||
| Yes | 78 (38.8%) | 42 (31.3%) | 15 (38.5%) | 21 (75.0%) | |
| No | 123 (61.2%) | 92 (68.7%) | 24 (61.5%) | 7 (25.0%) | |
| Smoking at Operation, N (%) | 0.216 | ||||
| Yes | 21 (10.4%) | 11 (8.2%) | 7 (17.9%) | 3 (10.7%) | |
| No | 180 (89.6%) | 123 (91.8%) | 32 (82.1%) | 25 (89.3%) | |
| Smoking History, N (%) | 0.627 | ||||
| Yes | 77 (38.3%) | 50 (37.3%) | 14 (35.9%) | 13 (46.4%) | |
| No | 124 (61.7%) | 84 (62.7%) | 25 (64.1%) | 15 (53.6%) | |
| SLNB, n (%) | 0.779 | ||||
| Yes | 138 (68.7%) | 92 (68.7%) | 29 (74.4%) | 17 (60.7%) | |
| No | 57 (28.4%) | 38 (28.4%) | 9 (23.1%) | 10 (35.7%) | |
| Alnd, N (%) | 0.953 | ||||
| Yes | 56 (27.9%) | 37 (27.6%) | 10 (25.6%) | 9 (32.1%) | |
| No | 139 (69.2%) | 93 (69.4%) | 28 (71.8%) | 18 (64.3%) | |
| Radiation Therapy Prior To Reconstruction, n (%) | 0.011 | ||||
| Yes | 27 (13.4%) | 13 (9.7%) | 11 (28.2%) | 3 (10.7%) | |
| No | 174 (86.6%) | 121 (90.3%) | 28 (71.8%) | 25 (89.3%) | |
| Radiation Therapy After Operation, N (%) | 0.852 | ||||
| Yes | 34 (17.0%) | 24 (18.0%) | 6 (15.4%) | 4 (14.3%) | |
| No | 166 (83.0%) | 109 (82.0%) | 33 (84.6%) | 24 (85.7%) | |
| Neoadjuvant Chemotherapy, N (%) | 0.293 | ||||
| Yes | 65 (32.3%) | 48 (35.8%) | 9 (23.1%) | 8 (28.6%) | |
| No | 136 (67.7%) | 86 (64.2%) | 30 (76.9%) | 20 (71.4%) | |
| Adjuvant Chemotherapy, N (%) | 0.62 | ||||
| Yes | 44 (22.0%) | 27 (20.3%) | 9 (23.1%) | 8 (28.6%) | |
| No | 156 (78.0%) | 106 (79.7%) | 30 (76.9%) | 20 (71.4%) | |
| SD: Standard Deviation; *p-values are based on one-way ANOVAs for continuous variables and chi-square tests for categorical variables. | |||||
Table 1: Demographics by A1C Category.
Postoperative complications after tissue expander placement were assessed in each group. The prediabetic group and diabetic group had a higher percentage of overall complication rate (57.5% and 53.8% respectively), when compared to the normal population (31.3%) (p=0.003). The percentage of patients that sustained a loss of their tissue expanders was also increased in the prediabetic (10%) and diabetic groups (22.2%) with statistical significance (p= 0.029). Dehiscence, hematoma, surgical site infection, seroma requiring in office percutaneous drainage and tissue expander exposure were all higher in the diabetic population, but this was not statistically significant (Table 2).
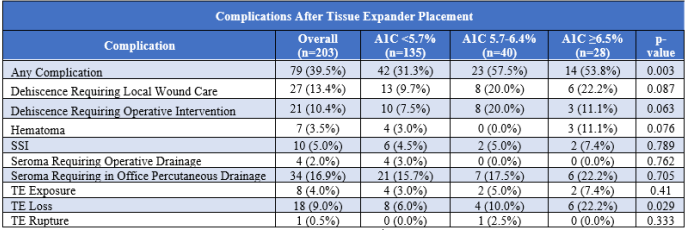
Table 2: Complications by A1C Category After Tissue Expander Placement.
Unweighted univariate linear regression models were then performed to assess the odds ratio for complications after tissue expander placement. The pre-diabetic and diabetic populations were more likely to have a complication after their tissue expander placement (OR=2.96, 95% [1.43,6.12], OR=2.56, 95% CI [1.09,6.00]) when compared to the normal population. The diabetic group was also more likely to sustain a tissue expander loss during the initial surgery when compared to the normal population (OR=4.50, 95% CI [1.42,14.28]) (Table 3).
Table 3: Linear Regression Model After Tissue Expander Placement.
In contrast to tissue expander placement, tissue expander exchange for permanent implant did not show statistical significance throughout the data points. The overall complication rate, dehiscence requiring local wound care, surgical site infection, seroma requiring operative drainage, and implant loss were similar between the diabetic group and the normal group (Table 4). The univariate linear regression models also did not show statistical significance between groups (Table 5).
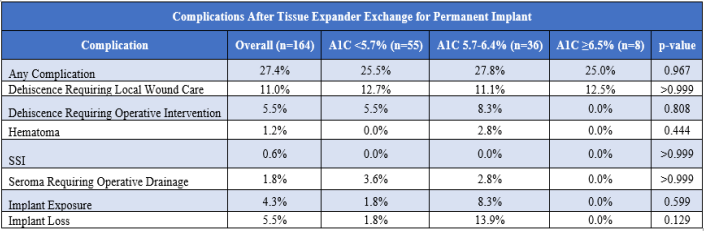
Table 4: Complications by A1C Category After Tissue Expander Exchange for Permanent Implant.
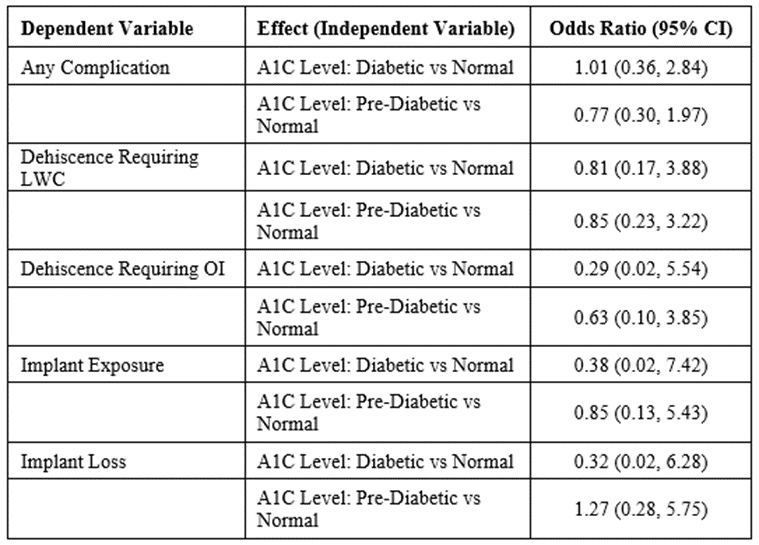
Table 5: Linear Regression Model After Tissue Expander Exchange for Permanent Implant.
Implant-based breast reconstruction is the most common form of reconstruction for patients having undergone mastectomy for breast cancer2. Wound healing complications such as dehiscence, seroma, hematoma, and infection, remain common causes of reconstructive failure19-20. As the incidence of diabetes continues to rise in the United States, poor glycemic control is an important factor to consider preoperatively5. While plastic surgeons may counsel patients to achieve adequate control of their diabetes in order to optimize wound healing, currently, there is no clear consensus on whether preoperative blood glucose or hemoglobin A1C is definitively associated with increased complication rates in implant-based breast reconstruction patients. This retrospective review of 203 patients found a higher rate of total complications after the initial surgery in both the pre-diabetic and diabetic groups that was statistically significant. There was a trend of higher rates of dehiscence requiring local wound care, dehiscence requiring operative intervention, hematoma formation, surgical site infection, seroma requiring operative drainage, seroma requiring in office percutaneous drainage, tissue expander exposure, and tissue expander rupture without statistical significance. In addition, diabetic patients were 4.5 times more likely to experience tissue expander loss than non-diabetic patients. A statistically significant increase in the overall rate of complication and in the rate of tissue expander loss may lead to overall delays in reconstruction, asymmetries, an increased psychological burden on the patient, and an increased cost to the healthcare system [2,3,17]. Therefore, our results suggest that prediabetic and diabetic patients should be appropriately counseled about the risks of tissue expander loss and their increased overall complication risk when considering implant-based reconstruction. During tissue expander exchange for permanent implant, we found that elevated A1C did not increase the risk of complications or implant loss. These findings suggest that complications associated with poor glycemic control should be focused on the tissue expander phase of implant-based reconstruction. We postulate that the breast skin flaps have undergone a surgical delay phenomenon from the initial expander placement making them more robust. There is also less dissection required involving the skin likely diminishing wound healing complications. Both factors likely contribute to the lower complication rate during the implant exchange mitigating any effects of the glycemic levels in these patients. This study is not without limitations. Notably, this was a single institution retrospective investigation and may not be generalizable. This study had a relatively small sample size of 203 total patients. An area of improvement for this study would be to assess a larger number of patients. This would make the overall study more powerful and help account for confounding elements. There was a higher percentage of patients in the prediabetic group with pre-operative radiation which may have contributed to the overall complication rate. There was also selection bias for patients who underwent surgery. Patients may have had extremely elevated A1C values and elected not to have surgery until this was more controlled. Our study was not designed to capture these patients. Based on the data obtained, routine A1C screening prior to the initial tissue expander placement could be beneficial for patient counseling. The ultimate decision to delay surgery should be a conversation between the surgeon and patient. Each patient should be approached individually, and their cancer treatment may take precedent. An option would be to proceed with their cancer treatment and then delay their reconstruction until an appropriate A1C could be obtained. This would, however, add additional cost and an additional procedure for the patient. Consideration should be taken to delay any prophylactic mastectomy cases as there is no urgency and medical optimization of glycemic control makes sense to lessen the risks of reconstructive complications.
This study found that patients with elevated A1C defined as prediabetic (5.7-6.4%) or diabetic (≥6.5%) are at an increased risk for overall complications and diabetic patients are at increased risk for tissue expander loss during the first stage of implant-based breast reconstruction. There were no associated risks for the second stage implant exchange procedure. A preoperative hemoglobin A1C may aid plastic surgeons when counseling patients seeking implant-based tissue expander breast reconstruction.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
