
Research Article | DOI: https://doi.org/10.31579/2690-1919/294
1 Mayo Clinic School of Graduate Medical Education, Department of Internal Medicine, Mayo Clinic, Scottsdale, AZ, USA
2 Mayo Clinic Department of Emergency Medicine, Phoenix, AZ, USA
3 Mayo Clinic Department of Health Sciences Research, Scottsdale, AZ, USA
*Corresponding Author: Douglas E. Rappaport. Mayo Clinic Department of Emergency Medicine, Phoenix, AZ, USA.
Citation: Cody A. Cunningham, Douglas E. Rappaport, Nicole R. Hodgson, Kevin M. Drechsel, Andrej Urumov et al. (2022). The effect of a ‘Covid tent’ on Emergency Department efficiency and patient satisfaction: A single site retrospective study, J. Clinical Research and Reports, 12(2) DOI:10.31579/2690-1919/294.
Copyright: © 2022 Douglas E. Rappaport. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 December 2022 | Accepted: 22 December 2022 | Published: 30 December 2022
Keywords: emergency medicine; covid-19; ed overcrowding; quality improvement
Background:Overcrowding in Emergency Departments is associated with poor patient outcomes and low patient satisfaction; overcrowding has been exacerbated by the ongoing Covid-19 pandemic. One intervention used in both the H1N1 pandemic and the current Covid-19 pandemic is the deployment of temporary structures such as surge tents. Data on the effectiveness of such interventions is currently lacking.
Methods:In this retrospective study, we assess ED length of stay (LOS), percent of patients leaving without being seen, and 72-hour return rate in the time period during tent operation with equivalent time periods before and after tent use. Differences in outcomes were modeled and tested using Generalized Estimating Equations (GEEs) methodology and controlled for emergency severity index (ESI).
Results:Deployment of a Covid tent was associated with reduced LOS (227.5 vs. 214.5 min, ESI-adjusted p = 0.02). Additionally, we observed a significantly reduced rate of patients leaving without being seen (0.8% vs. 0.2%, ESI-adjusted p < 0.001) without any increase in the 72-hour return rate (4.2% vs 4.2%, ESI-adjusted p = 0.98) during the period of Covid tent operations.
Conclusion:This data suggests that the deployment of temporary structures such as tents is an effective means of decompressing EDs in the setting of the Covid-19 pandemic.
Emergency Department (ED) overcrowding is a widespread problem and is associated with poor patient outcomes and low patient satisfaction. Critically ill patients presenting to overcrowded EDs experience a longer duration of mechanical ventilation, longer ICU stays, and higher mortality [1]. However, this problem is not restricted to the critically ill as even lower acuity patients that present to, and are discharged from, overcrowded EDs have a higher risk of death within 10 days [1]. EDs have developed several mitigation strategies to decompress overcrowding including active bed management and the development of ED-ICUs [2, 3].
During the H1N1 influenza pandemic of 2009, EDs faced a surge in patient volumes. In many cases, EDs were forced to accommodate a doubling of their average daily census [4]. Many institutions rapidly expanded ED capacity, typically by repurposing existing hospital space. Some used climate-controlled tents to expand capacity [5]. This strategy is advantageous as it allows for rapid expansion of capacity and allows for isolation of potentially contagious patients outside the main ED. One single center study during the H1N1 pandemic revealed that an outdoor tent was associated with decreased patient elopement rates and reduced ED length of stay without significant changes in ED recidivism [4].
The emergence of the SARS-CoV-2 virus and the resultant Covid-19 pandemic exacerbated ED crowding. Many EDs, particularly those located within the geographic regions that experienced surges of cases, noted a rapid and steep increase in average daily patient census. Of note, many of these census increases have occurred despite precipitous declines in patients presenting with non-Covid-19 chief complaints [6].
Our 35-bed Emergency Department sees approximately 40,000 patients per year at a large tertiary care center and serves the Phoenix Metropolitan area with a population of 4.3 million. Arizona experienced a peak of 4,877 new cases/day (702 new cases per 1M) on July 1, 2020, and a peak hospital census for Covid-19 patients of 3,493 (503 hospitalizations per 1M) on July 15, 2020, during the “summer wave” of the Covid-19 pandemic. To rapidly expand capacity during this surge, we deployed a ‘Covid tent’ in the parking lot across from the main ED entrance that served low and moderate acuity patients with complaints consistent with Covid-19.
There is minimal existent data on the effectiveness of temporary tent structures on ED throughput and patient satisfaction in the setting of Covid-19 [7]. Many institutions deployed these structures based on data from previous pandemics such as the H1N1 influenza pandemic of 2009 [4, 5]. Given the significant differences between H1N1 and Covid-19 (including magnitude of pandemic, patient characteristics, treatment modalities and mortality) data on the effectiveness of this intervention in the setting of Covid-19 is urgently needed. The purpose of this study was to examine the effectiveness of our ‘Covid tent’ by analyzing ED patient length of stay, rate of patients leaving without being seen, and unexpected 72-hour return rate.
Study Design
We operated the tent for 40 days (July 10, 2020 to August 18, 2020) which corresponded to a surge of cases in the Phoenix, AZ metropolitan area. We selected an equivalent period before and after tent operations for comparison (June 19, 2020 to July 8, 2020 and August 19, 2020 to September 8, 2020). We retrospectively measured ED length of stay, percent of patients that left without seeing a provider, and percent of patients that returned to the ED within 72 hours (72-hour return rate) in the period before/after and during Covid tent operations. Our institutional review board identified this project as exempt from full approval process as it was conducted for quality review purposes.
Participant Selection
From July 10, 2020 (tent opening) to August 18, 2020 (tent closure), we assigned patients presenting to the ED between 9 am and 7 pm with symptoms consistent with SARS-CoV-2 infection (respiratory distress, shortness of breath, cough, sore throat, headache, loss of smell, change or loss of taste sensation, chills, body aches/myalgias, nausea, vomiting, or diarrhea) [8] to the Covid tent if they were symptomatic with heart rate < 120> 90 mmHg, respiratory rate < 30> 90%. We also assigned asymptomatic patients presenting to the ED requesting Covid testing to the tent. Patient age and the presence or absence of comorbidities were not used as triage criteria. We treated patients with suspected or confirmed SARS-CoV-2 infection
who were noted to have vital signs outside these parameters in the main
ED due to an increased likelihood of respiratory failure which would necessitate endotracheal intubation, mechanical ventilation, and other critical care interventions. The ED team saw all patients in the main ED after tent closure (7 pm) each evening.
Intervention
The Covid tent was a 2,500 square foot air-conditioned tent located in the parking lot across from the entrance of the main ED. The tent was sufficient to accommodate 5 bedded patients and 5 seated patients. We staffed the tent with 1 emergency physician, 3 RNs, 1 ED tech, and 1 radiology technician. The tent was equipped with portable x-ray capabilities, cardiac monitoring, phlebotomy, supplemental (low flow) oxygen therapy, limited oral/parenteral medications (antipyretics, antibiotics, analgesics, and antiemetics) in addition to IV fluids. If necessary, the tent team obtained additional medications and supplies from the main ED.
Measurements
We measured ED length of stay (in minutes), percentage of patients that left without being seen, and percentage of patients that returned within 72 hours (unexpected 72-hour return rate).
Setting
The Mayo Clinic Arizona Hospital is a 268-bed, urban, tertiary referral center located in Phoenix, AZ. The ED sees approximately 40,000 patients per year and can accommodate 26 roomed patients and 9 hallway patients. The ED serves patients of all ages while the hospital serves patients age ≥ 16 years old.
Statistics
Descriptive statistics are reported by time period (before/after tent deployment vs during tent deployment). Differences in outcomes by time period were modeled and tested using Generalized Estimating Equations (GEEs) methodology to estimate a model of the association between the outcome and time period, controlling for emergency severity index (ESI), and accounting for the association between visits from the same patient. As a secondary analysis, outcomes were compared between tent appropriate (TA) patients seen during the before/after tent time period and patients seen in the tent, also using GEE methods to control for ESI and account for within-patient association. In brief, TA patients were generated by applying the tent triage workflow (see Participant Selection above) to patients who presented to the ED during the before/after tent period. Analysis was performed using SAS 9.4. All tests were two-sided, with p < 0>
During tent operation (July 10, 2020 to August 18, 2020) the ED saw 4,209 patients (main ED + Covid tent) whereas the ED saw 4,596 patients in the equivalent time period before and after tent operation (June 19, 2020 to July 8, 2020 and August 19, 2020 to September 8, 2020). The tent inclusion criteria appropriately triaged patients as only 39 of 4,209 patients (0.92%) required transfer from the tent to the main ED. Conversely, only 3 of 4,209 patients (0.07%) were moved from the main ED to the tent. The demographics of the patients presenting to the ED before/after tent operation and during tent operation are shown in Table 1.
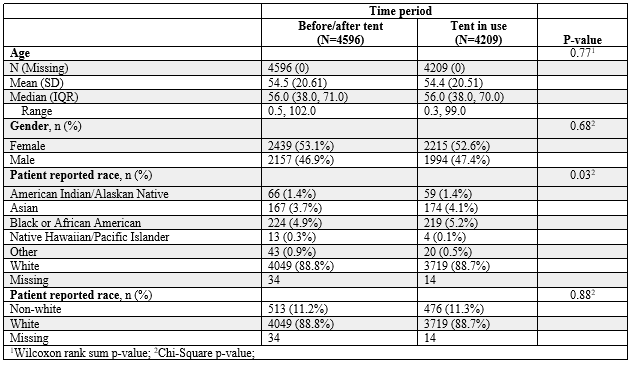
Table 1: Patient-visit demographics by time period
There were no statistical differences in patient age or gender composition between the two time periods. There was a subtle but statistically significant difference in the composition of patient reported race between the two time periods, likely due to the statistical power of the large data set. Of the 4,596 patients seen in the ED before/after tent operations, 4,348 (94.6%) were seen by a physician and 248 (5.4%) were nurse only visits (Table 2).
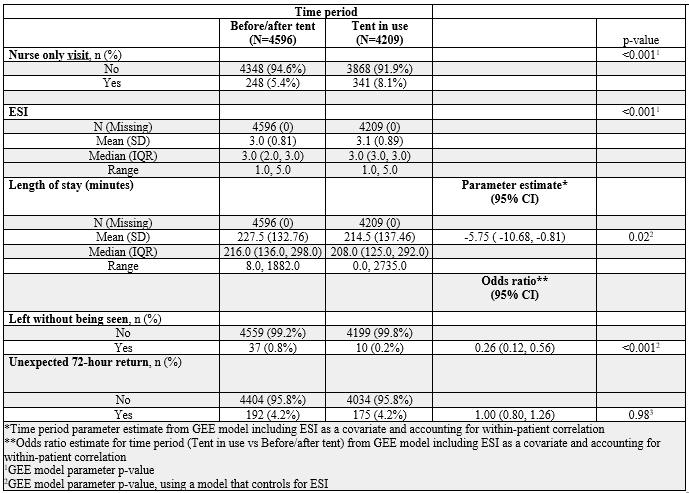
Table 2: Outcomes by time period
Nurse-only visits were asymptomatic patients presenting to the ED for SARS-CoV-2 nasopharyngeal testing. During the time period that the tent was in use, the department saw 4,209 patients, 3,868 (91.9%) of which were seen by a physician and 341 (8.1%) were nurse-only visits. The Covid tent saw 614 of those patients; 328 (53.4%) were seen by a physician and 286 (46.6%) were nurse-only visits. The acuity of patients presenting to the ED in the periods before/after and during Covid tent operations were similar as evidenced by comparable median ESI scores (3.0 vs. 3.0). Covid tent operation was associated with a shorter LOS compared to before/after tent operations (214.5 min vs. 227.5 min). After adjusting for ESI, the average LOS was 5.75 min shorter (95% CI: 0.81 –
10.68 min) during Covid tent operation (p = 0.02). Covid tent operations were also associated with a reduced rate of patients leaving without being seen (0.8% vs. 0.2%, ESI-adjusted p < 0>p = 0.98).
Next, we assessed the effectiveness of the Covid tent by comparing patients seen within the tent (see participant selection above) with patients who presented in the period before/after the tent was operational but would have been triaged to the tent had it been operational (tent appropriate) (Table 3).
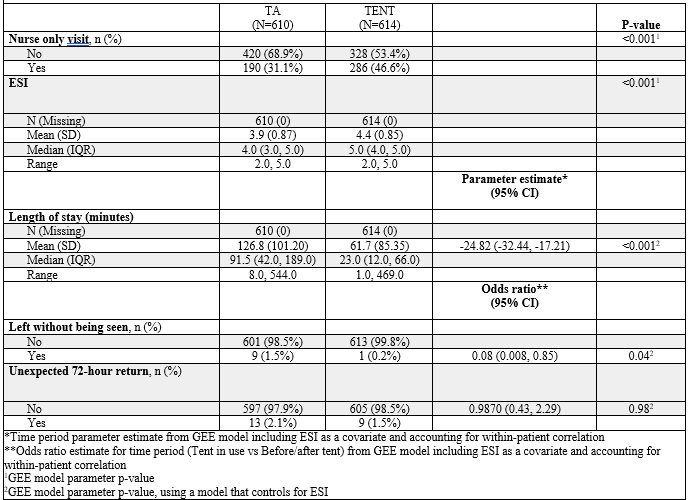
Table 3: Outcomes among Tent Appropriate (TA) vs Tent patients
The average LOS was shorter for patients assigned to the Covid tent compared to tent appropriate patients seen in the period before/after tent deployment (61.7 min vs. 126.8 min). After adjusting for ESI, LOS among tent patients was 24.82 min shorter on average (95% CI: 17.21 – 32.44 min) compared to the LOS of tent appropriate patients (p < 0 xss=removed>
The use of temporary structures such as tents in accommodating the surge of Covid-19 patients is largely predicated on past experiences, such as the H1N1 influenza pandemic. However, Covid-19 poses challenges to the health care system that are unique such as more rapid community spread, and a higher burden of morbidity and mortality compared to influenza [9]. As such, it is critically important to assess the effectiveness of this intervention in the setting of Covid-19. Our single center retrospective study shows that the deployment of a ‘Covid tent’ was associated with a decreased length of stay and a decreased rate of patients leaving without being seen. These outcomes indicate that Covid tents are effective in decompressing crowded emergency departments. Importantly, the increased patient throughput was not associated with an increase in 72-hour return indicating that patients continued to receive appropriate emergency care. Lastly, we have shown that care is delivered faster in the Covid tent compared to “tent appropriate” patients seen in the main ED, likely due to a streamlined workflow. These results are in line with a recent study which found chest radiographs are obtained more expeditiously in a dedicated ‘fever tent’ compared to the usual radiography facilities in the setting of the Covid-19 pandemic [10]. An ED with a shorter length of stay and a decreased rate of patients leaving without being seen could impact patient satisfaction. Indeed, our internal patient satisfaction surveys showed a significant increase in patient satisfaction when comparing the time period when the tent was operational to equivalent time periods before/after tent operations (data not shown). While not assessed in this study, the deployment of surge tents like the one described in this study likely has the additional benefit of separating infectious Covid-19 patients from other susceptible patients thus reducing the likelihood of nosocomial infection.
This study does have several important limitations. This study is retrospective in nature and is single center. Additionally, our institution does not have an inpatient pediatric service and therefore pediatric ED visits are infrequent. As pediatric patients have differential rates of mild vs. severe disease compared to adult patients [11], these results may not be generalizable to pediatric emergency departments.
In this single-center retrospective study, the deployment of a ‘Covid tent’ was associated with a reduced patient LOS and rate of patients leaving without being seen. Additionally, no significant changes in 72-hour return rate were observed. Taken together, these data show that the deployment of temporary structures such as tents are an effective means to decompress EDs in the setting of the current Covid-19 pandemic.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
