
Case Report | DOI: https://doi.org/10.31579/2768-2757/151
Department GI Surgery,Vamshodaya Hospital, Kolar, India.
*Corresponding Author: Vinay H G., Department GI Surgery,Vamshodaya Hospital, Kolar, India.
Citation: Vinay H G., Naveen N., Ramprashanth., (2024), The Diagnostic Challenge of Gallbladder Volvulus: A Case Report, Journal of Clinical Surgery and Research, 5(9); DOI:10.31579/2768-2757/151
Copyright: © 2024, Vinay H G., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 November 2024 | Accepted: 02 December 2024 | Published: 23 December 2024
Keywords: young, male; acute pain abdomen; diagnostic dilemma
Background: Gall bladder volvulus is a rare intra-operative diagnosis mimicking acute cholecystitis, usually seen in elderly females.
Clinical Description: Patients usually present with acute onset, right upper quadrant pain in the abdomen. It may be associated with vomiting, jaundice or a palpable lump
Management: Though conservative percutaneous drainage is attempted as an initial procedure, the definite management includes a cholecystectomy with laparoscopic approach preferred over open surgery.
Conclusion: Diagnosis of gall bladder volvulus is challenging and often impossible pre-operatively. Delay in definite surgical management increases the mortality and morbidity of the patients.
A rare clinical entity with less than 400 reported cases in the literature, gall bladder volvulus is a disease with undetermined incidence.[1] It is most commonly seen in elderly patients, mimicking acute cholecystitis. The diagnosis is usually made intraoperatively, as most radiological diagnoses are inaccurate.[2] Here we present one such case in a young male.
A 25-year-old young gentleman presented to our outpatient department with complaints of abdominal pain for days. It was associated with vomiting and fever for the same duration. The pain was more in the right upper quadrant and was progressive. The patient was admitted for further management. The vitals were stable on admission. On further evaluation, the tenderness was present in the right hypochondriac region with localized guarding. There was no rigidity. Bowel sounds were present in all quadrants. The rest of the systemic examination was normal. The ultrasonogram of the abdomen and pelvis was reported to have distended with diffuse edematous wall thickening of the gall bladder measuring 1.5cm and was associated with pericholecystic fluid and intraluminal sludge. Consent was taken for operative procedure and the patient underwent laparoscopic cholecystectomy on the next day. Intraoperatively, a floating gallbladder twisted along the axis of cystic pedicle with a gangrenous wall was visualized. Early mass formation with adhesions between the gall bladder, duodenum and omentum was also noted.
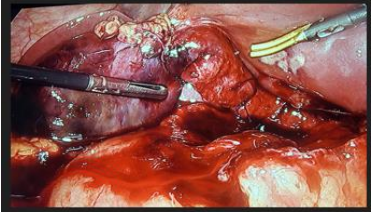
Figure 1: The entire gall bladder was excised.

Figure 2: and sent for HPE for confirmation. It revealed gangrenous gall bladder with ulcerated mucosa.
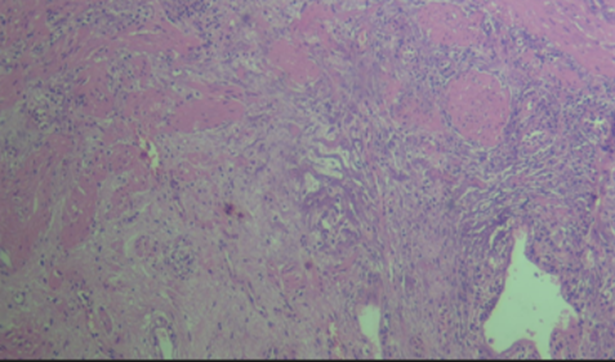
Figure 3: The patient was discharged after 3 days with stable vitals and no post-operative complications were present.
The gallbladder volvulus is a rare entity with approximately 500 documented cases in literature. The exact reason for the volvulus is not established, however many risk factors have been documented. The lack of visceral peritoneum to support the gall bladder due to embryological variation, results in a congenital floating gall bladder, susceptible to volvulus. Two anatomical variants are described [3] with
The patients present with abdominal pain with a palpable lump, fever or jaundice. A triad was described by Lau et. al. An elderly thin patient with sudden onset right upper quadrant pain with emesis, and a palpable right upper quadrant mass with a non-toxic presentation. [6] Serologic tests are non-specific and mimic any other inflammatory illness, with raised white cell counts. An ultrasonogram of the abdomen and pelvis cannot distinguish between acute cholecystitis and torsion. A contrast-enhanced computed tomography of the abdomen reveals a gall bladder fossa collection with twisting of the gall bladder at the pedicle. Magnetic resonance imaging and Magnetic Resonance Cholangiopancreatography is an excellent tool for detecting gall bladder volvulus. [7] Medical management is not recommended as the volvulus has to be released. Percutaneous drainage of the gall bladder could be attempted as initial management of the torsion but is associated with an increased risk of bile leak and bile peritonitis. Cholecystectomy is the best treatment modality for gall bladder torsion with laparoscopic a preferred over laparotomy, due to lesser post-operative pain and shorter duration of stay. The principles associated with gall bladder torsion is decompression, detorsion and gall bladder removal. [8] Delayed surgery is associated with poorer outcomes.
Gallbladder volvulus is a rare but critical condition requiring urgent medical intervention. Ultrasonography is typically the first imaging technique for diagnosis, and Doppler ultrasound should be utilized if gallbladder volvulus is strongly suspected. Early surgical intervention is crucial once the condition is identified to prevent complications such as gangrene, gallbladder rupture, and biliary peritonitis, all of which can significantly reduce survival rates.
Nil
No.
NA, Patient identity not revealed.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
