
Research Article | DOI: https://doi.org/10.31579/2690-4861/656
Jingchu University of Technology,448000, No.33, Xiangshan Avenue, Dongbao District, Jingmen City, Hubei Province, China.
*Corresponding Author: David Vinyes, Jingchu University of Technology,448000, No.33, Xiangshan Avenue, Dongbao District, Jingmen City, Hubei Province, China.
Citation: Qin Hui, (2025), The Current Situation and Influencing Factors of Presenteeism among Clinical nurses in Jingmen City China: A Cross-Sectional study, International Journal of Clinical Case Reports and Reviews, 22(2); DOI: 10.31579/2690-4861/656
Copyright: © 2025, Qin Hui. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 December 2024 | Accepted: 03 January 2025 | Published: 13 January 2025
Keywords: boreda; cattle; economic loss; fasciolosis; prevalence; risk factor
Aim: This research investigates presenteeism among clinical nurses in Jingmen City, China, and identifies its influencing factors.
Design: A cross-sectional study design was employed.
Methods: A total of 2,222 clinical nurses in Jingmen City were surveyed from June to July 2024. The level of presenteeism was assessed using the Stanford Presenteeism Scale. Socio-demographic data, inclusive leadership, and organizational support were measured through a self-developed structured questionnaire, the Inclusive Leadership Scale, and the Organizational Support Scale. Descriptive statistics, univariate analysis, correlation analysis, and stepwise multiple linear regression analysis were utilized to evaluate the factors influencing presenteeism among clinical nurses.
Results: The mean scores for presenteeism, inclusive leadership, and organizational support among clinical nurses were 16.95 ± 3.27, 36.14 ± 5.02, and 50.17 ± 7.64, respectively. Variations in presenteeism were observed based on age, educational background, marital status, childlessness status, establishment type, professional title, position, length of service, and department category. However, no significant differences were found concerning gender, exercise frequency, physical condition, and religious beliefs. Correlation analysis revealed a negative relationship between perceived inclusive leadership and organizational support and presenteeism. Stepwise multiple linear regression identified marital status, employment method, professional title, number of night shifts, inclusive leadership, and organizational support as significant influencing factors of presenteeism among clinical nurses.
Presenteeism refers to a variety of issues encountered by staff within a unit, including psychological or physical health problems that arise from diminished attention during work. Employees experiencing presenteeism are unable to fully engage both their body and mind in the tasks at hand, which results in decreased focus, a lack of dedication to their work, reduced efficiency, and diminished accountability for their responsibilities (Chapman 2005).
Research relevant to this issue indicates that presenteeism is prevalent among domestic medical staff, with nurses being particularly susceptible to this behavior. In one study, the proportion of nurses exhibiting high rates of presenteeism in their departments exceeded 50%, with pediatric nurses showing an even higher prevalence of 58.3% (MIKOS et al. 2020). Another survey revealed that 62 percent of the 1,171 nurses surveyed in a state reported experiencing presenteeism at least once in the past year, with the phenomenon being more pronounced in larger hospitals compared to small and medium-sized facilities (Aronsson and Dallner 2000).
Clinical nurses face heavy workloads, manage complex patient needs, and operate in unique working environments. Consequently, their physical and mental health is often adversely affected, contributing to the occurrence of presenteeism (Rainbow 2019, Freeling et al. 2020). Nurses represent the primary force in providing hospital care for patients. When presenteeism behavior occurs, the quality of nursing services declines. The severity of presenteeism is directly correlated with an increased likelihood of adverse effects on patient safety and the quality of medical treatment (Rainbow and Steege, 2020). Furthermore, presenteeism among nurses can result in decreased work efficiency, a heightened risk of nursing errors, and increased medical costs (Margadant et al., 2020). A significant correlation exists between nurse presenteeism and an increase in patient falls, dosing errors, and a decline in the overall quality of care. Researchers have estimated that the economic loss associated with patient falls and medication errors due to nurse presenteeism exceeds $1,346 per year, leading to total economic losses of over $2 billion annually, which includes substantially increased medical and economic costs (Letvak and Gupta, 2012).
2.1 Design
For data collection, a cross-sectional questionnaire survey was carried out during June and July 2024. The manuscript was formulated in accordance with the STROBE checklist for cross-sectional studies.
2.2 Participants
A total of 2222 nurses from 4 tertiary hospitals in Jingmen citywere recruited as participants in this study. The inclusion criteria were as follows: (1) Possession of a nurse practice certificate; (2) At least one year of working experience; (3) Currently employed in nursing work within the hospital; (4) Informed consent and willingness to participate in this study. The exclusion criteria were: rotation or leave, interns, and refresher clinical nurses.
2.3 Assessment instruments
The survey encompasses four components: demographic characteristics, The Stanford Presenteeism Scale, The Inclusive Leadership Scale, and the Organizational Support Scale.
2.3.1 Demographic characteristics
We employed a self-developed demographic questionnaire to gather the information of participants, encompassing gender, age, educational attainment, marital status, whether having children or not, employment mode, professional title, position, nursing work experience, department, night shift, physical exercise after work, history of underlying diseases, health status and religious belief, etc. These factors were selected in accordance with previous research.
2.3.2 The Stanford Presenteeism Scale (SPS-6)
SPS-6 was originally compiled by Koopman and subsequently revised by the Chinese scholar Zhao Fang (Zhao et al 2010) in 2010. Consisting of 6 items, responses are scored on a five-point Likert scale, with items 1-4 being assigned positive scores and items 5 and 6 being designated as negative scores. The total score of the scale is the accumulation of the scores of the 6 items, and the total score ranges from 6 to 30 points. The higher the score, the more pronounced the presenteeism. The Cronbach's α coefficient of this scale fluctuated between 0.760 and 0.912, indicating excellent reliability and validity, and it is extensively employed in the nursing domain. The Cronbach's α coefficient of the SPS-6 in this study was 0.886.
2.3.3 The Inclusive Leadership Scale
The Inclusive Leadership Scale was initially developed by Carmeli et al. and was subsequently revised by the Chinese scholar Peng Wei (Peng et al 2016) in 2016. This scale encompasses three dimensions and nine items, specifically openness (3 items), availability (4 items), and accessibility (2 items). Each item is evaluated on a five-point Likert-type scale ranging from 1 (‘not at all’) to 5 (‘very much’), where higher scores imply more conspicuous inclusive leadership styles for nurse managers. The scale demonstrates excellent reliability and validity, with a Cronbach's α coefficient of 0.90. The Cronbach's α coefficient of this scale in the present study was 0.842.
2.3.4 The Organizational Support Scale
The Organizational Support Scale, revised by Zuo Hongmei (Zuo et al 2009), is grounded on Chen ZX's scale. It combines the characteristics of the nursing profession and undergoes extensive consultation with experts. Some items have been appropriately modified, encompassing 2 dimensions and a total of 13 items. Among them, items 1-10 pertain to emotional support, and items 11-13 relate to instrumental support. The Likert 5-level scale is employed to assign values ranging from 1 to 5, with scores ranging from "completely disagree" to "completely agree". The higher the score, the more intense the sense of organizational support. This scale demonstrates good reliability and validity, with the Cronbach's α coefficient being 0.90 and is widely utilized in the nursing field. The Cronbach's α coefficient of this scale in the study was 0.897.
2.4 Data collection
The study was conducted anonymously using an electronic questionnaire utilizing the Questionnaire Star platform. Prior to the survey, informed consent was obtained from the relevant head of the nursing department in each hospital. The researchers obtained the contact information of the head nurses of each department through the nursing department managers of the four hospitals, and sent the e-questionnaire to the head nurses through the WeChat APP, which was then forwarded by the head nurses to the departmental workgroups for the clinical nurses to fill in the questionnaire. In order to ensure the completeness and validity of the recovered questionnaires, a unified filling guide was adopted, and all questions were required. Each IP address could only fill in the questionnaire once, and the cumulative time for answering the questionnaire was set at not less than 180 seconds. A total of 2294 questionnaires were distributed, 2253 questionnaires were collected, and 31 questionnaires with logical errors were excluded. Finally, 2222 questionnaires were effectively collected, with an effective recovery rate of 98.81%.
2.5 Data analysis
The data collected for the study were analyzed using SPSS version 26.0 statistical analysis software. 2 researchers rechecked the data and questionnaires that did not meet the inclusion criteria were excluded from the analysis. Normality test was used to see if the data conformed to normal distribution. Median (interquartile range) was used to describe the data. Categorical data were calculated by frequencies and proportions. Independent samples t-test and one-way ANOVA were used to compare differences in attendance scores of nurses with different characteristics, Pearson's correlation analysis was used to analyze the correlation between inclusive leadership of nurses, organizational support, and nurses' attendance, and multivariate linear regression was used to analyze the factors influencing attendance. The significance level for all statistical tests was set at 0.05.
2.6 Research ethics committee approval
This study was approved by the Ethics Review Committee of the Jingmen cityCity People's Hospital. Participation in this study was completely voluntary and anonymous. Prior to the commencement of the trial, all participants completed a permission form authorizing data collection. All procedures were carried out in conformity with the applicable norms and regulations. They were also told of the study's goal and the option to participate or quit at any time.
3.1 Participant characteristics
The characteristics of the Participants are presented in Table 1. Approximately 98.2% (n= 2182) of the participants were women, and most of the nurses were aged 20-30 years (n= 957, 43.1%). Most nurses have undergraduate degree (n= 1807, 81.3%) and only a few have a master's degree or above (n=42, 1.9%). 1631 nurses were married and 1628 nurses have children. The majority of nurses are contracted (n=1025, 46.1%). More than half of the nurses have primary professional titles (n= 1200, 54.0%). Nurses working for 1-10 years comprised the largest group (n= 1336, 60.1%) and 1177 nurses have 1–5-night shifts per month. Nurses mainly come from internal medicine department (n=729, 32.8%) and surgery department (n=592,26.6%). More than half of the nurses do 1-2 physical exercises per month (n= 1316, 59.2%) and most nurses are in good physical condition. Only 28 nurses have religious beliefs.
| Variable | n | % | Presenteeism Score | t/F | P |
| Gender | t=1.536 | 0.125 | |||
| Male | 94 | 4.2Z | 17.46±2.50 | ||
| Female | 2128 | 98.20 | 16.93±3.30 | ||
| Age | F=15.462 | 0.000 | |||
| 20-30 | 957 | 43.07 | 17.78±2.37 | ||
| 31-40 | 863 | 38.84 | 17.55±3.09 | ||
| 41-50 | 304 | 13.68 | 14.41±3.62 | ||
| 51-60 | 95 | 4.28 | 11.46±1.87 | ||
| >61 | 3 | 0.14 | 11.00±1.00 | ||
| Educational background | F=15.624 | 0.000 | |||
| polytechnic school | 21 | 0.95 | 13.09±3.37 | ||
| Junior college | 352 | 15.84 | 17.61±2.83 | ||
| Undergraduate degree | 1807 | 81.32 | 16.88±3.31 | ||
| Master degree or above | 42 | 1.89 | 16.29±3.36 | ||
| Marital status | F=25.437 | 0.000 | |||
| unmarried | 502 | 22.59 | 17.85±2.64 | ||
| married | 1631 | 73.40 | 16.71±3.36 | ||
| Divorce or Widow | 89 | 4.01 | 16.33±4.03 | ||
| Have children or not | t=8.827 | 0.000 | |||
| Yes | 1628 | 73.27 | 16.61±3.44 | ||
| No | 594 | 26.73 | 17.88±2.57 | ||
| Employment method | |||||
| Formal preparation | 517 | 23.27 | 14.94±4.11 | F=169.07 | 0.000 |
| Contract system | 1025 | 46.13 | 17.15±2.83 | ||
| Personnel Agency | 680 | 30.60 | 18.17±2.34 | ||
| Professional title | F=309.33 | 0.000 | |||
| Nurse | 218 | 9.81 | 17.71±2.53 | ||
| Junior title | 1200 | 54.01 | 17.58±2.81 | ||
| Intermediate title | 598 | 26.91 | 17.33±3.04 | ||
| Senior title | 206 | 9.27 | 11.39±1.35 | ||
| Nursing work experience (years) | F=169.13 | 0.000 | |||
| <10 | 1336 | 60.13 | 17.72±2.75 | ||
| 10~20 | 563 | 25.34 | 17.02±2.83 | ||
| 21~30 | 184 | 8.28 | 15.35±4.23 | ||
| 31~40 | 135 | 6.08 | 11.41±1.59 | ||
| >40 | 4 | 0.18 | 10.75±0.96 | ||
| How many nights shifts every month | F=214.10 | 0.000 | |||
| No | 384 | 17.28 | 13.66±2.57 | ||
| 1~5 | 1177 | 52.97 | 17.35±2.92 | ||
| 6~10 | 608 | 27.36 | 18.06±2.36 | ||
| >10 | 53 | 2.39 | 19.19±1.97 | ||
| Department | F=3.64 | 0.000 | |||
| Surgery | 729 | 32.81 | 16.94±3.09 | ||
| Medicine | 592 | 26.64 | 17.43±3.23 | ||
| Oncology | 72 | 3.24 | 16.94±3.06 | ||
| ICU | 148 | 6.66 | 17.59±2.72 | ||
| operating room | 139 | 6.26 | 16.19±3.23 | ||
| outpatient service | 145 | 6.53 | 14.79±3.75 | ||
| emergency room | 119 | 5.36 | 17.57±3.07 | ||
| Other | 278 | 12.51 | 16.83±3.49 | ||
| Weekly physical exercise frequency (after work) | F=1.852 | 0.136 | |||
| No | 336 | 15.12 | 17.21±3.26 | ||
| 1~2 | 1316 | 59.23 | 16.97±3.27 | ||
| 1~2 | 350 | 15.75 | 16.63±3.22 | ||
| >2 | 220 | 9.90 | 16.96±3.39 | ||
| Health status | t=0.681 | 0.496 | |||
| Good | 1859 | 83.66 | 16.97±3.30 | ||
| Bad | 363 | 16.34 | 16.84±3.14 | ||
| Religious belief | t=0.964 | 0.335 | |||
| No | 2194 | 98.74 | 16.96±3.28 | ||
| Yes | 28 | 1.26 | 16.36±2.89 | ||
Table 1: Demographic characteristics of participants (n=2222).
3.2 Score of Presenteeism of Nurses (Table 2)
Table 2 shows that the total score of the Stanford Presenteeism Scale nurses is high,which indicates that although nurses are working, their work efficiency is very low.
| Variate | Score range | Score(x±s) |
| In the past month, due to health issues, my work pressure has become even more difficult to regulate. | 1~5 | 3.48±1.07 |
| In the past month, due to health issues, I have been unable to complete difficult tasks in my work. | 1~5 | 2.96±1.02 |
| In the past month, due to health issues, I have been unable to enjoy my work. | 1~5 | 3.13±1.18 |
| In the past month, due to health issues, I feel it is impossible to carry out certain work tasks. | 1~5 | 3.29±1.07 |
| In the past month, despite health issues, I have been able to concentrate and complete my work. | 1~5 | 1.99±0.71 |
| In the past month, despite health issues, I still feel energized and able to complete all work. | 1~5 | 2.09±0.79 |
| Total | 6~30 | 16.95±3.27 |
Table 2: Items and total scores of nurses' Stanford Presenteeism Scale
3.3 Score of The Inclusive Leadership Scale of nurses(Table 3)
| Dimension | Items(n) | Score range | Score(x±s) |
| Openness | 3 | 3~15 | 12.23±2.00 |
| Availability | 4 | 4~20 | 15.59±2.59 |
| Accessibility | 2 | 2~10 | 8.32±5.02 |
| Total | 9 | 9~45 | 36.14±5.02 |
Table 3: Score of The Inclusive Leadership Scale of nurses
3.4 Score of The Organizational Support Scale Table 4)
| Dimension | Items(n) | Score range | 得分(x±s) |
| Emotional support | 10 | 12~50 | 36.70±6.14 |
| Instrumental support | 3 | 4~15 | 11.48±7.64 |
| Total | 13 | 18~65 | 50.17±7.64 |
Table 4: Score of The Organizational Support Scale
3.5 Correlation of nurse inclusive leadership, organizational support and Presenteeism(Table 5)
| Variate | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Presenteeism |
| Openness | -0.260** | -0.215** | -0.159** | -0.117** | -0.138** | -0.013** | -0.280** |
| Availability | -0.256** | -0.219** | -0.180** | -0.132** | -0.081** | -0.056** | -0.291** |
| Accessibility | -0.242** | -0.215** | -0.220** | -0.198** | -0.082** | -0.031** | -0.315** |
| Inclusive leadership | -0.290** | -0.247** | -0.206** | -0.159** | -0.115** | -0.041** | -0.333** |
| Emotional support | -0.134** | -0.102** | -0.143** | 0.023** | -0.279** | -0.394** | -0.275** |
| Instrumental support | -0.228** | -0.208** | -0.196** | -0.144** | -0.147** | -0.111** | -0.316** |
| Organizational support | -0.172** | -0,140** | -0.170** | -0.022** | -0.266** | -0.348** | -0.310** |
Table 5: Correlation of nurse inclusive leadership, organizational support and Presenteeism
Notes:** Level 0.01 (double tail) with significant correlation
3.6 Results of multiple linear regression analysis of nurses’ presenteeism influencing factors(Table 6)
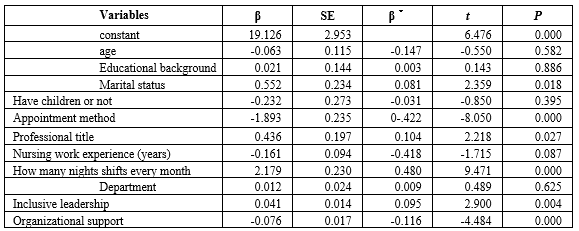
Table 6: Multiple linear regression analysis of nurses’ presenteeism influencing factors
Notes:F=69.913,R2=0.258,△R2=0.254,P<0.001.
The results of this study show that the presenteeism score of nurses in tertiary hospitals in Jingmen cityis 16.95 ±3.27, which is higher than the survey results of clinical nurses in tertiary hospitals by Ding Hui (Ding et al 2021), Wu Yue (Wu et al 2021), and Chen Rose (Chen et al2021). Compared with the median score of 15 points in the scale, it is at a moderate to high level. The analysis of the reasons may be related to the city's large demand for medical treatment, the shortage of nursing human resources, specific performance in the (1) workload: The high turnover of outpatients and inpatients in tertiary general hospitals and the prevalent need for surgery and resuscitation make the nurses' workload very heavy. (2) High pressure of nursing management environment: Quality of care management in tertiary general hospitals is higher than in other grades and other types of hospitals, which puts pressure on nursing staff while promoting the effective implementation of nursing norms (Shi et al 2019). (3) High social expectations: As healthcare reforms continue to advance, people are increasingly demanding higher standards of medical care and quality of nursing services. Nurses have to spend more time and energy to improve their operational capabilities, which leads to greater physical and mental stress. (4) Low professional security: the incidence of workplace violence among nurses in Jingmen city hospitals is high, and the tertiary hospitals is higher than that of secondary hospitals (Zhao et al 2022). Nurses' sense of professional safety has declined in the face of ongoing exposure to medical disputes and medical injuries. Therefore, hospital administrators should pay high attention to the phenomenon of nurse attendance, emphasize the physical and mental health of clinical nurses and the implementation of humanistic care, increase the intensity and depth of nursing professional investment and management, and provide targeted violence-responsive resources in order to increase nurses' motivation, creativity, and productivity and reduce the loss of productivity caused by attendance behaviors.
The results of this study showed that the nurses' perceived inclusive leadership score was 36.13 ±5.02, which was at a higher level compared with the median of the total score of 22 points. Leadership style will affect the work quality of clinical nurses, patients and working environment (Specchia et al 2021). Inclusive managers are more willing to listen to different points of view of employees, enhance employees' self-knowledge, encourage employees to put forward bold suggestions, and give employees effective and efficient help and support in a timely manner (Abraham and Zivc 2010). Research has shown that inclusive leadership styles of nursing managers are negatively correlated with nurses' attendance. Nurses under inclusive leadership feel respected, cared for, supported, and understood, resulting in better performance and more favorable team diversity diversification (Zhu et al 2021).
The study found that the nurses' organizational support was 50.17 ± 7.64, which was at a high level compared with the median value of the total scale score of 65 points. It has been found that when hospital organizations provide visible support and assistance to clinical nurses, it stimulates good working conditions and psychological outlook of the nurses, which in turn improves the efficiency and productivity of the organization and creates a virtuous circle (Huang et al 2021). In addition, organizational support can enhance nurses 'professional identity and sense of professional value, and improve job satisfaction (Assiri et al 2020), which is conducive to nurses' work input and reduce the occurrence of presenteeism behavior. We suggest that nursing administrators should give nursing staff full understanding and respect, evaluate the comprehensive performance of hospital clinical nursing staff objectively, comprehensively and fairly, give more praise and less punishment, and calm negative work emotions. In addition, they should pay active attention to the life of nursing staff and the professional development of nursing staff, provide fair promotion opportunities, conduct career development training, encourage participation in continuing education programs, etc., and establish a harmonious relationship with them.
Correlation analysis showed that nurses' perceived inclusive leadership and organizational support are negatively correlated with presenteeism, Stepwise multiple linear regression showed that marital status、employment method、professional title、number of night shifts、inclusive leadership and organizational support are the influencing factors of presenteeism among clinical nurses. Nursing managers should pay attention to establish and improve the management system, explore the evaluation and employment system of professional and technical titles, innovating a reasonable salary assessment and incentive system, and strengthening the humanistic care of recruiting nurses. The one-way variance results showed that the presenteeism scores of nurses with junior, intermediate and senior professional titles decreased successively, that is, the lower the title of the nurse, the higher the presenteeism rate, which is consistent with Zhu Yan's findings (Zhu et al 2021) study. The reason for this may be that senior nurses generally undertake management or teaching work that is relatively stable, while junior and intermediate nurses generally undertake clinical frontline work, with high pressure for title promotion, high consumption of time and energy, and declining work engagement and efficiency, which to a certain extent impairs their physical and mental health and leads to absenteeism. The results showed that nurses with more night shifts had higher absenteeism scores than those with fewer night shifts, which is consistent with Ren Yuexia's study (Ren et al 2022). Nursing managers should conduct flexible scheduling according to the actual situation of the department, establish a more flexible nursing team (Bagheri et al 2019, Virkstis et al 2021), maximize the potential of nurses, improve the work input of nurses. Inclusive leadership can influence the nurses presenteeism behavior, the reason may be nursing managers inclusive leadership style can enhance the level of subordinate nurse’s insider identity perception, and effectively promote subordinate nurses’ psychological authorization perception, nurses can feel the support and help from the organization, will be more actively into the nursing work.
The study is of great significance in improving the quality of nursing care, stabilizing the nursing workforce, reducing healthcare costs, promoting nurses' health, responding to societal expectations, coping with the shortage of nurses, facilitating the development of healthcare policies, and enhancing international competitiveness. Healthcare organizations and policy makers should pay attention to this issue to take effective measures to ensure that nurses can provide quality nursing services to patients in a healthy state.
The results of this regional survey should be interpreted with caution due to the following limitations. This study was conducted only in the Jingmen region, with no additional data from other regions, so the results cannot be generalized to all Chinese nurses. Second, this study utilized a self-report survey method, which may have resulted in exaggerated or underestimated scores on the measurement scales, and possible inherent bias cannot be ruled out.
The current situation of presenteeism of nurses in the tertiary hospitals in Jingmen city is relatively serious, among which different marital status、employment method professional title number of night shifts inclusive leadership and organizational support are the main influencing factors of nurses' presenteeism behavior. Nursing managers should formulate scientific and effective management system, make rational use of nursing human resources, implement humanistic care for nurses, adopt inclusive leadership, so as to improve the work enthusiasm and efficiency of nurses, so as to reduce the incidence of presenteeism.
The authors would like to thank Professor Zeng Tao of the Department of Medicine, Jingchu university of Technology for his guidance on this manuscript, and are very grateful to the Directors of the Nursing Departments of Jingmen People's Hospital and Jingmen Central Hospital for their help!
Ethical issues are not involved in this paper.
All contributing authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
