
Research Article | DOI: https://doi.org/10.31579/2692-9759/095
Cardiology, CHU d’Ibn-Rochd, Casablanca, Morocco.
*Corresponding Author: CHARIF Hana, Cardiology, CHU d’Ibn-Rochd, Casablanca, Morocco.
Citation: Hana C., EL M. Meryem, Rachida H., MAROC C., (2023), The Consequences of Confinement on Patients Followed at The Heart Failure Treatment Unit (HFTU): Experience of The Cardiology Department – Chu Ibn Rochd-Casablanca, Cardiology Research and Reports. 5(2); DOI:10.31579/2692-9759/095
Copyright: © 2023, CHARIF Hana, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 April 2023 | Accepted: 14 April 2023 | Published: 21 April 2023
Keywords: heart failure; sanitary confinement; SARS COV-2
Introduction
In the absence of effective treatment for SARS-Cov2 (severe acute respiratory syndrome coronavirus 2), social distancing and containment measures are the most effective ways to fight the pandemic to date. Nevertheless, these latter measures may have repercussions in particular on heart failure.
Objective
To assess the impact of confinement in patients followed in the heart failure treatment unit at the cardiology department of Ibn Rochd hospital.
Method
We selected a random sample of patients followed in HFTU. We collected their demographic data as well as the evolution of their symptoms, their clinical parameters, biological, and their lifestyles at the beginning of the confinement and 1 year later.
Results
We included 100 patients at random. We found a significant increase in BMI of 6.85 kg/m2. The rate of sedentary lifestyle rose by 40% and 63.9% of patients increased their salt intake by more than 4 g/day. We noted a worsening of heart failure symptoms. Thus, 10.6% of patients with stage 2 dyspnea progressed to NYHA stage 3 (32.4 vs. 40.5%), while the percentage of patients with IMO increased by 21.5%. 11 deaths for end-stage heart failure, 38 hospitalizations for heart failure flare-ups including 12 patients following a deviation from diet and treatment, 10 to a rhythm disorder, 8 to an ischemic flare-up, 6 to a pulmonary embolism and 2 patients following a SARS COV2 infection.
Conclusion
The sanitary confinement has had a significant impact on patients followed for heart failure, from where the need to restructure our healthcare system and develop remote therapeutic education.
The SARS COV-2 (severe acute respiratory syndrome coronavirus 2) infection causing the disease covid-19 originated in December 2019 in Wuhan, China. Then it quickly spread to more than 100 countries in less than three months and evolved into a pandemic with a major impact on worldwide health [1].
To prevent the saturation of intensive care services, contagion prevention measures were quickly adopted by most affected countries, including social distancing which remains the oldest and most effective way to control the spread [2]. However, these measures generate significant health, social and economic consequences [3].
In Morocco, the first case of covid19 was confirmed on March 2, 2020. As of March 20, a state of health emergency was declared and total confinement was imposed as an inevitable and necessary public health measure in order to prevent the spread of the virus and protect the population.
According to the first epidemiological studies published, cardiac patients represent subjects at risk likely to develop the most severe forms of covid-19 [4]; cardiac involvement is described as a high-risk factor for mortality in patients with covid-19 [5], [6]. This oversaturation has led the medical authorities to recommend postponing the majority of non-urgent care activities. The aim is to limit the exposure of patients in healthcare settings deemed to be at high risk to Covid-19. In this perspective, non-urgent consultations have been postponed or carried out by telemedicine.
Nevertheless, these last measures may have repercussions in particular on patients followed for chronic diseases in particular patients followed with heart failure.
In this context, the objective of our study will be to assess the impact of the current COVID-19 pandemic and the consequent Moroccan lockdown measures on cardiovascular risk factors, eating habits, lifestyle, as well as on the evolution of symptoms and clinical signs in patients followed for chronic heart failure without COVID-19.
Study design and population
We chose a random sample of patients followed at the cardiology department of the CHU Ibn Rochd Casablanca. We collected their demographic data as well as the evolution of their symptoms, their clinical and biological parameters, and their lifestyles at the start of confinement and 1 year later.
This is a prospective study carried out on a sample of Moroccan patients followed for chronic heart failure at the heart failure treatment unit (HFTU) of the cardiology department – CHU Ibn Rochd-Casablanca.
The data was collected between July 10, 2020 and July 10, 2021.
We randomly included in this study; all the patients followed in the HFTU for chronic heart failure.
The inclusion criteria are as follows:
The follow-up period was 1year. The patients were called then by teleconsultation during the follow-up.
Data entered in Excel
An initial descriptive analysis was performed. Quantitative variables are presented as mean ± standard deviation; qualitative variables in the form of counts (percentages).
It was ethically important, from the start of the study, to obtain the voluntary and informed consent of the patients.
The investigators are committed to respecting the confidentiality of the data collected (anonymity).
We included 100 patients. The average age of our population is 57 years ± 13.22. The average BMI (body mass index) is 28.36 kg/m2 ± 7.14. Coronary pathology is present in 42% of patients, valvular in 36 %. Finally, arrhythmias appear in 22% and more than half of our sample (64%) is hypertensive. We found a significant average weight gain of 9 kg after 1 year of confinement with an increase in BMI of 6.85 kg/m2 (p < 0>
The sedentary rate shows an increase of 40 % (p < 0>
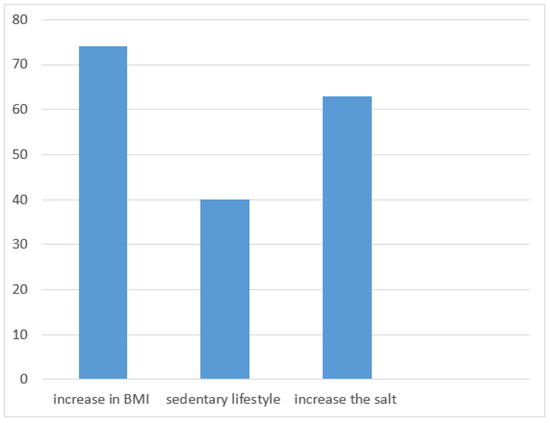
We included 100 patients at random. We found a significant increase in BMI of 6.85 kg/m2. The rate of sedentary lifestyle rose by 40% and 63.9% of patients increased their salt intake by more than 4 g/day. We noted a worsening of heart failure symptoms. Thus, 10.6% of patients with stage 2 dyspnea progressed to NYHA stage 3 (32.4 vs. 40.5%), while the percentage of patients with IMO increased by 21.5%. 11 deaths for end-stage heart failure, 38 hospitalizations for acute heart failure including 12 patients following a deviation from diet and treatment, 10 to a rhythm disorder, 8 to an ischemic flare-up, 6 to a pulmonary embolism and 2 patients following a SARS COV2 infection
Thus, 10.6% of patients with stage 2 dyspnea progressed to NYHA stage 3 (32.4 vs. 40.5%), while the percentage of patients with IMO increased by 21.5%. 11 deaths for end-stage heart failure, 38 hospitalizations for acute heart failure including 12 patients following a deviation from diet and treatment, 10 to a rhythm disorder, 8 to an ischemic flare-up, 6 to a pulmonary embolism and 2 patients following a SARS COV2 infection.
We noted an aggravation of heart failure symptoms. Thus, 10.6 % of patients with stage 2 dyspnea progressed to NYHA stage 3 (32.4 vs 40.5%), while the percentage of patients with lower limb edema increased by 21.5 %. We noticed a diet gap with an increase in salt intake (more than 4 g per day) in more than half of this subpopulation (63.9%) during the confinement period. In the subpopulation with valvular disease, we found worsening dyspnea in 10.5% of patients; this went from NYHA stage 2 to stage 3 with an increase in the percentage of patients with OMI from 7.5% to 25% 1 year later (p = 0.065). In addition, we observed 11 deaths for end-stage heart failure, 38 hospitalizations for acute heart failure including 12 patients following a deviation from diet and treatment, 10 to a rhythm disorder, 8 to an ischemic flare-up, 6 to a pulmonary embolism and 2 patients following a SARS COV2 infection.
Our prospective study included a total of 100 patients followed in the heart failure treatment unit (HFTU)of the CHU of Casablanca, confined and not suffering from Covid-19, with evaluation of the impact of confinement on cardiovascular risk factors, eating habits, mode of life, as well as on the evolution of symptoms and clinical signs in patients followed for chronic heart failure.
Thus, we noted an increase in BMI after 1 year of confinement. Similar results were described in an American study; Weight gain greater than 2.26 kg was observed in 22% of the population studied [10].
Regarding physical activity, our cardiac patients practicing low physical activity increased from 43 to 65 patients with a p < 0>
In our study, we noted a significant drop in tobacco consumption in cardiac patients (22% vs 12%) after 1 year of confinement. Probably related to the closure of cafes and open spaces, and awareness campaigns against covid-19 carried out by the Ministry of Health.
12 patients showed decompensation due to a deviation from the low-sodium diet, poor therapeutic compliance and non-use of care. This last notion was reported by a study carried out in an emergency department in Italy which underlined a reduction in the number of patients consulting for heart failure flare-ups of 49%, contrasting with an observed rise in all-cause mortality at the hospital [8]. The same finding was observed in an English study [9].
Finally, we will cite a study carried out in Paris during the pandemic period. This objectified an increase in the incidence of cardiac arrests occurring outside hospital with a rapid return to normal in the last weeks of the pandemic thanks to the development of teleconsultations and the launch of public campaigns to encourage the use of medical care for symptoms unrelated to COVID-19 [10].
Strengths and limitations of our study
To our knowledge, our study would be the first research on the impact of confinement on patients followed with chronic heart failure. Nevertheless, we are aware of its limitations, due to the lack of comparison of biological parameters.
Our recommendations
Favor a balanced diet based on fruits, fresh vegetables, soybeans and nuts which are sources of antioxidants and omega-3s with the avoidance of foods rich in sugar, saturated fatty acids and animal proteins.
Practice adequate physical activity, especially during the current pandemic. (Walking at home, dancing, online courses, etc.).
Develop awareness-raising and therapeutic education actions (encourage subjects to seek care, therapeutic and low-sodium diet compliance, the use of telemedicine, etc.).
According to the results of this study, sanitary confinement has had significant repercussions on patients followed for chronic heart failure. The need to raise awareness among these patients, and above all to restructure our highly disrupted healthcare system by COVID-19.
Sanitary confinement has had significant repercussions on the state of health of cardiac patients, hence the importance of raising patients' awareness of maintaining physical activity in accordance with international recommendations, but also of a balanced diet, smoking cessation on the one hand, and on the other hand, not to hesitate to seek care as soon as symptoms appear or worsen.
None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
