
Research Article | DOI: https://doi.org/10.31579/2641-0419/470
1Internal Medicine/Cardiology, Wayne state University School of Medicine USA.
2Department of Emergency Medicine, Yaounde emergency Center Cameroon.
*Corresponding Author: Aubin Sandio, Internal Medicine/Cardiology, Wayne state University School of Medicine USA.
Citation: Aubin Sandio, Fleury Bolla, Murielle Guimbang, Dangpa Nana, Ludovic Tchounja, et al, (2025), The Concomitant Risk of Percutaneous Coronary Intervention before or after Transcatheter Aortic Valve Replacement: What comes First?, J Clinical Cardiology and Cardiovascular Interventions, 8(8); DOI: 10.31579/2641-0419/470
Copyright: © 2025, Aubin Sandio. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 April 2025 | Accepted: 27 May 2025 | Published: 10 June 2025
Keywords: transcatheter aortic valve implantation; coronary artery disease; PCI; aortic stenosis
The optimal Timing for percutaneous coronary intervention (PCI) in patients undergoing transcatheter aortic valve replacement (TAVR) remains uncertain. This research aims to evaluate the risk of patients diagnosed with severe aortic valve stenosis and coronary artery disease who undergo simultaneous PCI therapy during TAVR procedures. For quite a while now, Transcatheter Aortic Valve Replacement (TAVR) has established itself as a solid therapeutic approach for patients with severe symptomatic Aortic Stenosis (AS) (1, chrome last). A notable prevalence of concurrent coronary artery disease (CAD) has been observed among population undergoing TAVR, with approximately 40–75% of patients undergoing TAVR also receiving percutaneous coronary intervention (PCI) either during preoperative assessment or TAVR surgery [3] (Chrome last).
The current international guidelines recommend angiographic evaluation for patients with CAD exhibiting >70% stenosis in the proximal segment (or >50% stenosis in the left main artery) with planned PCI based on angiography findings (class II a, class C) [4]. Several studies on the treatment of patients with aortic stenosis and CAD [5–7] have indicated that PCI before or during TAVR does not significantly increase all-cause mortality and cardiovascular mortality compared to TAVR alone. However, we are still yet to understand the risk of concomitant PCI plus TAVR on short and long-term outcome in mortality. The appropriate time to undergo percutaneous coronary interventions (PCI) in patients undergoing transcatheter aortic valve replacement (TAVR) is not standard. In this analysis, we are looking at the timeline and the outcomes of patients who have received PCI before undergoing TAVR.
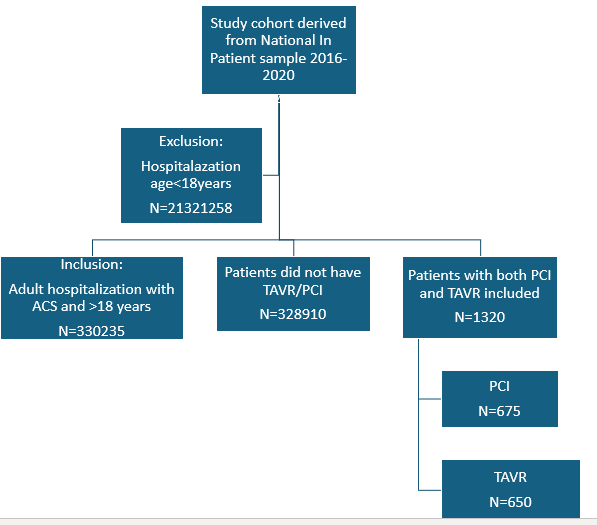
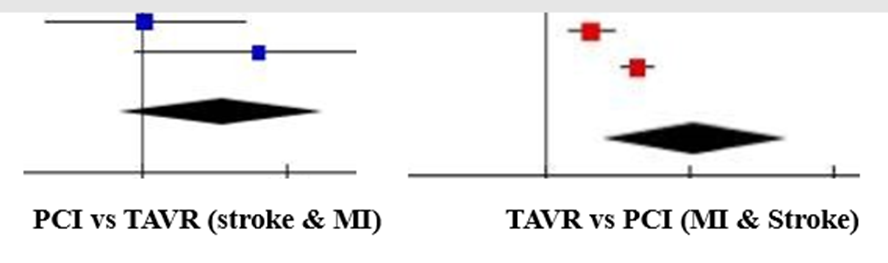
A comprehensive review articles search was conducted including the NIH database, Medline and HRSA for studies that compared two main procedures, the case of PCI before and after TAVR showing the impact of an outcome between the two procedures. The studied mainly focus on myocardial infraction, stroke and sudden cardiac death. The 3 studies included 1623 patients (pre-TAVR PCI n = 1445; post-TAVR PCI n = 178) were included in this study following our inclusion and exclusion criteria. The mortality rate was very high in patients within the pre-TAVR PCI group (OR: 2.37; 95% CI: 1.19–5.20; p = 0.02). No significant difference detected between PCI before and after TAVR for the risk of myocardial infraction, stroke (OR: 3.26; 95% CI: 0.70–17.22; p = 0.13) and Stroke (OR: 0.11; 95% CI: 0.29–1.21; p = 0.25). Patients with coronary arterial disease (CAD) undergoing PCI after TAVR is therefore associated with lower mortality as compared to patients undergoing PCI before TAVR.
TAVR era has given rise to new challenges in the management of CAD in patients with severe AS. Multiple questions arise regarding the safety and feasibility of PCI in patients with severe AS, the timing of revascularization, and the need of complete revascularization or not. The feasibility and safety of revascularization for patients undergoing TAVR. Total revascularization was achieved in 44% of patients with severe AS and CAD undergoing SAVR, whereas only 23% of patients with severe AS and CAD who underwent TAVR had total revascularization by PCI. This partially depicts the different management strategies. Coronary lesions that are accessed angiographically as ≥50% are almost always bypassed at the time of SAVR; however, PCI is indicated only for physiologically significant lesions of 50–70% as determined by FFR or of angiographically severe lesions of 90%. In multivariate analysis, total revascularization was not significantly associated with worse outcomes in either of the subgroup. The option of concomitant PCI and femoral TAVR seems to be enticing as it allows for treatment of both pathologies with a single arterial access. Potential advantages of this approach include reducing the time delay in performing both definitive procedures, decrease in the vascular and bleeding complications by avoiding separate vascular access for each procedure and avoiding the impact of myocardial ischemia and associated hemodynamic consequences of CAD during TAVR [4]. Furthermore, improved patient comfort and reduced costs associated with the pre-TAVI workup maybe also achieved with the combination of the two procedures in a single session. Despite the promising benefits, combining the two procedures comes with important considerations. Concomitant PCI and TAVR leads to increased procedure time, increased radiation exposure, and increased contrast exposure. This translates into augmented risk for stroke, cardiovascular complications, and kidney injury [32, 33]. Patients undergoing TAVR and PCI in the same session had similar rate of the composite of sudden death, disabling stroke, and myocardial infarction when compared with patients without CAD, and patients with severe CAD left untreated (TAVR + PCI 10.4%; severe CAD left untreated 15.4%; no-CAD 14.8%; p=0.72). Transcatheter aortic valve replacement (TAVR) is a major transformation for the treatment of severe aortic valve stenosis (AS), providing a minimal invasive option to surgical aortic valve replacement (SAVR) for geriatric patients with high surgical risk [1,2,3]. TAVR has become a preferred option due to its minimally invasive treatment, shorter recovery time, and reduced perioperative risks compared to the normal conventional aortic valve surgery. Percutaneous coronary intervention (PCI) prior to TAVR has been traditionally encouraged to optimize coronary perfusion and minimize the risk of ischemic events during the hemodynamic stress associated with transcatheter heart valve (THV) implantation [5]. This change in strategy aims to minimize the potential risks associated with PCI, such as bleeding complications and the need for dual antiplatelet therapy (DAPT) during the periprocedural phase of TAVR. Reducing the duration or need for DAPT is particularly beneficial in geriatric and patient with increased risk of fall, who are more prone to bleeding and other severe complications [7]. In addition, recent advances in imaging techniques and hemodynamic assessment tools have made it possible to better identify which coronary lesions effectively require intervention. While TAVR has significantly modified the treatment of severe AS, the management of concomitant CAD remains a critical aspect of patient care. The aim of this study is to investigate and provide a tentative recommendation for the optimal window of PCI in patients undergoing TAVR. The choice of THV type plays an important role in the decision to perform PCI before or after TAVR.
Although the current patients with concomitant CAD and AS are managed with SAVR and CABG, the data indicate that PCI can also be automatically process in the majority of patients with severe AS and concomitant obstructive CAD detected for TAVR. There is no obvious definitive recommendation on the timing of PCI in patients with obstructive CAD undergoing TAVR [21]. We can conclude that revascularization should be considered for severe coronary stenosis in proximal epicardial coronary vessels that supply a large area of myocardium at risk. This study includes many limitations. We were able to include only a small number of observational studies, therefore increasing the risk of bias in the results. To overcome the possibility of unexpected confounding factors, we performed a pooled analysis of adjusted HR, which confirmed that pre-TAVR-PCI was associated with an increased risk of mortality at follow-up when compared to post-TAVR-PCI. Furthermore, the result for adjusted HR was affected by high heterogeneity
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
