
Research Article | DOI: https://doi.org/10.31579/2641-5194/018
1 Assistant Professor, Department of Gastroenterology, Sheikh Russel National Gastroliver Institute & Hospital, Mohakhali, Dhaka, Bangladesh
2 Assistant Professor, Department of Gastroenterology, Shahid Syed Nazrul Islam Medical College, Kishoreganj, Bangladesh
3 Professor, Department of gastroenterology, BSMMU, Dhaka, Bangladesh
4 Assistant professor, Department of Gastroenterology, Sheikh Russel National Gastroliver Institute & Hospital, Mohakhali, Dhaka, Bangladesh
*Corresponding Author: Farid Ahmed, Assistant Professor, Department of Gastroenterology, Sheikh Russel National Gastroliver Institute & Hospital, Mohakhali, Dhaka, Bangladesh
Citation: Ahmed F., Pinaki Paul, Kabi A. and Hasan R. (2021) The Concentration of 25-Hydroxy Vitamin D in Chronic Liver Disease and Its Correlation with Severity J. Gastroenterology Pancreatology and Hepatobilary Disorders 5(1) DOI:10.31579/2641-5194/018
Copyright: © 2021, Farid Ahmed,This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 January 2021 | Accepted: 19 March 2021 | Published: 22 March 2021
Keywords: avitaminosis; parathyroid hormone; p ortal hypertension; gastric varices; child-pugh A; child-pugh B; child-pugh C; 25(OH) D; HCV; CLD
Background: Chronic liver disease (CLD is a common disease all over the world and the major cliological factors for the causation of disease are HBV and HCV in this country and Alcoholic liver disease in the western world. With the availability of the modern treatment, the life expectancy is increased now a days. But the long term complications are now evident. One of the complications is hepatic osteodystrophy which is associated with deficiency of vitamin D. Vitamin D undergoes hepatic 25-hydroxylation, but as the hepatic parenchyma is jeopardized so the metabolic activation of this vitamin is impaired. Vitamin D deficiency is highly prevalent in CLD patients and vitamin D level is inversely related to the severity of the disease.
Objective: To assess the concentration of 25-hydroxy vitamin D in chronic liver disease patient in different etiology and to study the relationship of level of 25(OH) D in different stages of the disease according to Child-Pugh classification.
Methods: This cross sectional study was carried out in the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University, Dhaka during the period of April 2015 to March 2016. Patient attending the Gastroenterology Department who fulfill the inclusion criteria with cirrhosis of liver were initially be enrolled for the study. Their clinical history, examination and initial investigation report were noted in the standard data sheet. After explaining the study objective, informed consent was taken. The diagnosis of liver cirrhosis was made by combination of clinical features, blood profile and transabdominal ultrasound. Endoscopy of the upper GIT was done to see the presence of oesophageal or gastric varices which is a sign of increase portal pressure. Transabdominal ultrasound demonstrated a shrunken liver with increase echogenicity, with or without splenomegally and presence or absence of ascites. Stages of liver disease were assessed by Child-Pugh scoring system. Level of 25(OH) D was measured from blood with the permission of the Department of Bio-chemistry. Data was collected using a structered data sheet.
Results: Out of 85 patients, male were 61 (71.8%) and female were 24 (28.2%). Mean age was 53.0 ± 10.7 years within tin- range of 25-70 years. More than 90.0% patient* had abates and anorexia. Eighty percent patients had weight loss and 71.8% patients had Jaundice. More than 40.0% patients had abdominal pain and melaena. Sixty (77.9%) patients had history of blood transfusion and 73 (94.8%) patients had previous hospitalization, Most of the patients had anaemia (97.6%) and Splenomegaly (92.9%). More than 50.0% patients had jaundice (61.2%), Leukonychia (61.2%) and hone pain (52.9%). Mean s, vitamin 25(OH) D was 16.29 ± 7.96 in 69 HBV patients and 20.14 ± 9.76 in 16 HCV patients. In this study, 28.2% patients were in child Pugh A, 36.4% in child Pugh B and 32.9% in child Pugh C stages. Mean s. vitamin 25(OH) D were 27.12 ± 6.11, 15.97 ± 5.40 and 9.57 ± J.I5 in Child-pugh A, Child-pugh B and Child-pugh C stages respectively. Mean s. vitamin 25(OH) D was gradually decreased as the changes of stage from lower to higher. Conclusion: Vitamin D deficiency is highly prevalent in patients with CLD and inversely correlated with disease severity. In the case of chronic liver diseases, vitamin D seems to modulate the innate and adaptive immune system, which explains the association. In fact, clinical studies suggest that these parameters may improve with vitamin D supplementation. So, monitoring of S. 25(OH) D is reasonable in CLD patient.
Cirrhosis may be defined us a phase of chronic liver disease or insult leads to the diffuse destruction of hepatic parenchymal cell by fibrosis and the formation of nodules, which results in disorganization of the liver’s lobular and vascular architecture. In western countries, common causes are alcohol. Where as in developing countries, common CHUM'S arc chronic hepatitis B or C virus infection [1]. Cirrhosis may be compensated or decompensated when complicated by jaundice, ascites, and hepatic encephalopathy or raised prothrombin time. It is insidious. Initially asymptomatic later present \\iih over! Complication [2]. The final stage of chronic inflammation in the liver is cirrhosis. Liver cirrhosis gives rise to portal hypertension and complications such as bleeding esophageal varices, ascites and encephalopathy. Hepato-cellular failure results in hyperbilirubinemia, hypoalbuminemia and prolonged prothrombin time. Child's grade is used to assess hepato-cellular function in cirrhosis based on these factors [3]. Though the disease is progressive, indolent and having many complications, but with the development of modern treatment modalities of cirrhosis of liver life span is increased. With the effective treatment long term complications are now commonly encountered. Metabolic bone disease occuring in patients with cirrhosis, known as hepatic osteodystrophy, covers both osteomalacia and osteoporosis [4]. It is a common complication among individuals with long standing hepatic disease. Various studies were conducted in different countries in the world to assess the prevalence of vitamin D deficiency in cirrhosis patient. One study was conducted in the University of Tennessee Hepatology clinic. Where one hundred and eighteen cirrhosis patients with different aetiology were included and their 25-hydroxy vitamin D level were measured. Severity was graded as mild (20-32 ng/ml), moderate (7-19 ng/ml) or severe (<7> 32 ng/ml [5]. Of patients one hundred eighteen, one hundred and nine had some degree of vitamin D deficiency. The result showed vitamin D deficiency is universal (92 %) among patients with cirrhosis and at least one third of them suffered from severe vitamin D deficiency [6]. Miroliace el al. of Iran, works with CLD patient where HBV (n=26), HCV (n=28), AIH (n=19), Cryptogenic (n=17) with 40 healthy controls [9]. Among the study population CM) group 56% male and Control group 60% male. The main outcome is significantly higher prevalence of vitamin D deficiency in cirrhotic versus non-cirrhotic patient (76% vs 17.9%, P < 0 xss=removed xss=removed xss=removed>
Specific Objectives:
Material and Methods
This cross sectional study was carried out in the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University, Dhaka during the period of April 2015 to March 2016. 85 patients attending the Gastroenterology Department who fulfill the inclusion criteria with cirrhosis of liver were initially be enrolled for the study. Their clinical history, examination and initial investigation report were noted in the standard data sheet. After explaining the study objective, informed consent was taken. The diagnosis of liver cirrhosis was made by combination of clinical features, blood profile and transabdominal ultrasound. Endoscopy of the upper GIT was done to see the presence of oesophageal or gastric varices which is a sign of increase portal pressure. Transabdominal ultrasound demonstrated a shrunken liver with increase echogenicity, with or without splenomegally and presence or absence of ascites. Stages of liver disease were assessed by Child-Pugh scoring system. Level of 25(OH) D was measured from blood with the permission of the Department of Bio-chemistry. Data was collected using a structered data sheet.
Exclusion criteria:
Operational Definition:
Cirrhosis of Liver: Cirrhosis is a diffuse process characterized by replacement of normal liver tissue by fibrosis and regenerative nodule formation [1]. The development of cirrhosis is usually an irreversible process. The term cirrhosis is a histologic diagnosis and has its own unique constellation of clinical manifestations such that a clinical diagnosis of cirrhosis can be made with confidence most of the time. The diagnosis of cirrhosis in clinical practice is based on risk factors, history and clinical findings, biochemical tests, imaging, endoscopic and histologic findings. The diagnosis of cirrhosis is not based on a single clinical parameter but a combination of above parameters and the identification and interpretation of these findings. The most common complication of cirrhosis of liver is ascites, hepatic encephalopathy, esophageal varices, splenomegaly, hematemesis and melaena.
Vitamin D: This is a water soluble vitamin which main function is to maintain the normal skeletal architecture and also plays an important role in cardiovascular and nervous system, cellular proliferation and differentiation. Vitamin D3 is primarily acquired through the photochemical conversion of 7- dehydrocholesterol to provitamin D3 in the skin. Vitamin D2 differs in that it is incorporated into micelle then further amalgamated into chylomicron via enterocyte absorption and reaches the liver from the venous circulation for hydroxylation. The serum concentration of 25(OH)D is the most commonly used biomarker for vitamin D status.
Endoscopy: Upper gastrointestinal endoscopy will be done using a standard forward viewing endoscope. In order to prevent contamination from another patient, after each procedure endoscope and biopsy forceps will be disinfected using glutaraldehyde 2% (CIDEX) solution. Instruments will be immersed in solution and kept for 15 minutes. Side channels will also be rinsed.
Data Collect Ion Method: Prior to data collection both verbal and written consent was taken from the respondents. Data ^recollected using a preformed data collection sheet (questionnaire). Base line information was collected from the patient after exploration of different complaints. All information regarding clinical features were recorded in a data collection sheet. S. 25-hydroxy vitamin D wow done in the Department of Bio-chemistry, Bangabandhu Sheikh Mujib Medical University Dhaka Bangladesh.
Data processing and analysis: After collection of data, all data will be checked and cleaned. After cleaning, the data will be entered into computer and statistical analysis of the results being obtained by using windows based computer software devised with Statistical Packages for Social Sciences. Numerical variables will be expressed as mean and standard deviation, whereas categorical variables are count with percentage. Continuous variables will be compared using Student's t test; categorical variables will be analyzed by Chi-square test. A p-value <0>
Liver failure and the Child-Pugh classification: The final stage of chronic inflammation in the liver is cirrhosis. Liver cirrhosis gives rise to portal hypertension and complications such as bleeding esophageal varices, ascites and encephalopathy. Hepato-cellular failure results in hyperbilirubinemia, hypoalbuminemia and prolonged prothrombin time. The Child-Pugh classification is a scoring system used to assess the prognosis of cirrhosis.

Although it was originally used to predict mortality during surgery, it is now used to determine the prognosis, as well as the required strength of treatment and the necessity of liver transplantation. Scoring is based upon several factors: albumin, ascites, total bilirubin, prothrombin time, and encephalopathy.

This cross sectional study was carried out in the Department of Gastroenterology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka from April 2015 to March 2016 for a period of 1 year. A total of 85 patients with chronic liver disease were included in this study. The results were as follows:
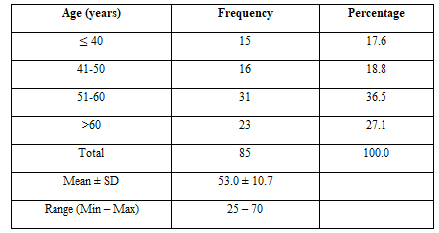
Table-1 Distribution of patients with CLD according to age. Maximum 36.5% patients were in age group 51-60 years followed by 23(27.1%), 16(18.8%) and 15 (17.6%) in >60, 41-50 and ≤ 40 years age group respectively. Mean age was 53.0 ± 10.7 years within the range of 25-70 years.
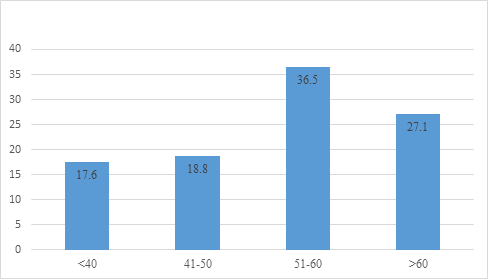
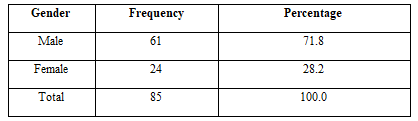
Table-2 shows distribution of patients according to gender. Male was predominant in this study. Male female ratio was 2.54:1
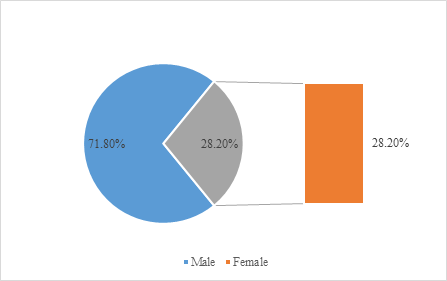

Table 3 show presenting complains of the CLD patients. More than 90.0% patients had ascites and anorexia. Eighty percent patients had weight loss and 71.8% patients had Jaundice. More than 40.0% patients had abdominal pain and melaena.
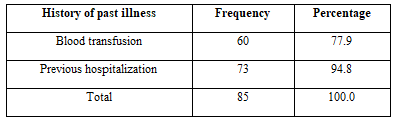
Table-4 shows history of past illness. Sixty (77.9%) patients had history of blood transfusion and 73 (94.8%) patients had previous hospitalization.
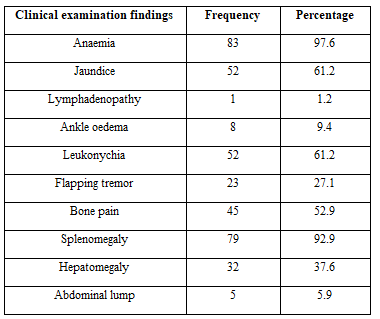
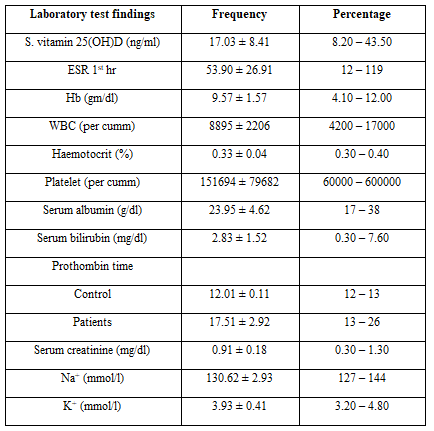


Table 7 shows level of s. vitamin 25(OH)D in different stages of CLD. Mean s. vitamin 25(OH)D was gradually decreased as the changes of stage from lower to higher. There was statistical significant difference in s. vitamin 25(OH)D among the different stages of CLD.
Vitamin D has pleiotropic functions. It is widely recognized to have a central role in calcium metabolism and bone mineralization. A vitamin D deficiency is causally related to rickets in children and osteomalacia in adults, but vitamin D is also physiologically important for the proper function of other organs such as skeletal muscle, heart, brain, and pancreas. Vitamin D deficiency is extremely common in chronic liver disease patients. Up to 93% of these patients have some degree of vitamin insufficiency [6, 19]. Even patients with mild liver disease are affected, although liver cirrhosis patients more commonly suffer from severe deficiency. In this study, males were predominant. Male female ratio was 2.54:1. Males were predominant and male female ratio was 2.70:1 [20]. The male female ratio was in the range of 2.3:1 to 2.6:1 among the patients with cirrhosis and HCC [21]. All these results are similar to this study result. Male female ratio of patients with CLD in Malayasia was 4.4:1 [22]. Maximum 36.5% patients were in age group 51-60 years followed by 23(27.1%), 16(18.8%) and 15(17.6%) in >60, 41-50 and <40>
In this study, 85 patients were enrolled and the mean S. 25(OH)D was 17.03 which was in the lower limit. The patient was also categorized according to severity with Child-Pugh classification and showed the level of vitamin D is inversely related to the severity of the disease.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
