
Mini-Review Article | DOI: https://doi.org/10.31579/2693-2156/089
1 Servicio de Kinesiología, Sanatorio Clínica Modelo de Morón, Morón, Buenos Aires, Argentina.
2 Servicio de paciente crítico, UCI quirúrgica, Hospital San Juan de Dios, Santiago, Chile.
3 Servicio de Medicina Física y Rehabilitación, Hospital San Juan de Dios, La Serena, Chile.
4 MoVICU Group, Mobility and Ventilation in Intensive Care Unit, La Serena, Chile.
*Corresponding Author: Adrián Gallardo, Servicio de Kinesiología, Sanatorio Clínica Modelo de Morón, Morón, Buenos Aires, Argentina.
Citation: Adrián Gallardo, Armando Díaz, and Patrick Sepúlveda, (2024), The Coin has Two Sides: Ventilation and Expiratory Muscles, J. Thoracic Disease and Cardiothoracic Surgery, 5(3); DOI:10.31579/2693-2156/089
Copyright: © 2024, Adrián Gallardo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 March 2024 | Accepted: 29 March 2024 | Published: 08 April 2024
Keywords: ventilation; expiratory muscles; respiration; quintessential physiological process; optimal diaphragmatic; PEEP; EELV
Respiration stands as a quintessential physiological process indispensable for oxygen provision and carbon dioxide elimination, thereby facilitating metabolic demands and upholding systemic biological homeostasis. At its core, respiration hinges upon the mechanical orchestration of gas exchange within the pulmonary system, governed primarily by the intricate interplay of respiratory musculature. Historically, scholarly emphasis has leaned towards the dynamic role of the diaphragm during inspiration, sidelining in-depth exploration of expiratory muscle mechanics.
Respiration stands as a quintessential physiological process indispensable for oxygen provision and carbon dioxide elimination, thereby facilitating metabolic demands and upholding systemic biological homeostasis. At its core, respiration hinges upon the mechanical orchestration of gas exchange within the pulmonary system, governed primarily by the intricate interplay of respiratory musculature. Historically, scholarly emphasis has leaned towards the dynamic role of the diaphragm during inspiration, sidelining in-depth exploration of expiratory muscle mechanics. This oversight has, arguably, curtailed comprehensive investigations into the expiratory phase, which, under normal circumstances, unfolds passively owing to the elastic properties of pulmonary parenchyma and thoracic architecture. This nuanced facet assumes critical significance within the context of mechanically ventilated patients, wherein the transition from controlled to partial ventilatory support emerges as a pivotal determinant of critical care outcomes. Hence, achieving harmonious synergy between the innate respiratory muscle dynamics of the patient and ventilator assistance constitutes the linchpin for successful weaning protocols. In this succinct discourse, we proffer a novel paradigm elucidating the nuanced intricacies of respiratory muscle function. Analogous to a coin's dual facets, ventilation embodies a dyadic interplay of processes that necessitate holistic examination: Mechanically ventilated cohorts commonly necessitate positive end-expiratory pressure (PEEP) augmentation, aimed at restoring end-expiratory lung volume (EELV), optimizing pulmonary mechanics, and enhancing gas exchange kinetics. However, this therapeutic modality harbors inherent dichotomies: while it mitigates declines in functional residual capacity (FRC) precipitated by supine positioning, abdominal surgeries, and pharmacological interventions (inclusive of neuromuscular blockade), excessive PEEP titration engenders caudal displacement of the diaphragmatic crura, surpassing its optimal equilibrium, thereby precipitating passive shortening and compromising mechanical efficacy. Furthermore, anecdotal evidence suggests expiratory muscle engagement in EELV modulation, particularly manifest in acute respiratory distress syndrome cohorts receiving fentanyl infusions. This paradigm underscores expiratory muscle dynamics' pivotal role in EELV maintenance, constituting a plausible mechanism for mitigating PEEP-induced overdistension and engendering protective ventilation strategies. It is possible that this mechanism is the product of some type of defensive vagal reflex, aimed at counteracting excessive pulmonary stress.
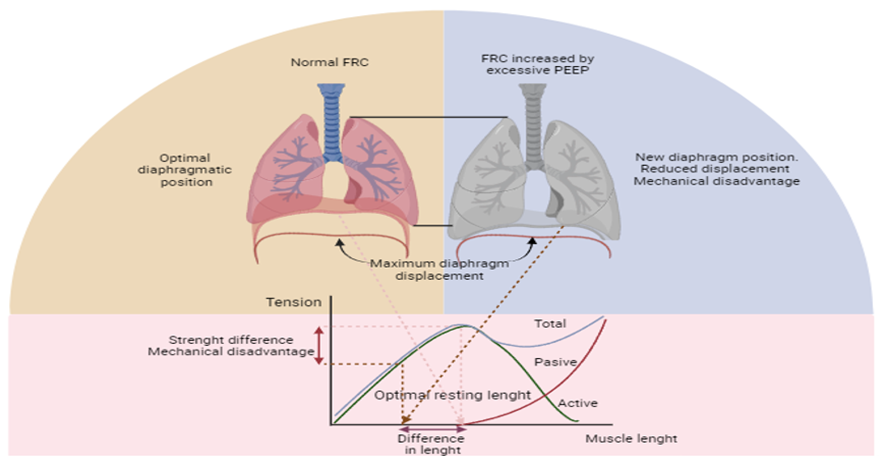
Figure 1: Diaphragmatic Displacement in Response to Excessive PEEP Application.
The new starting point determines a reduced capacity to exert force due to its shortened state. FRC: functional residual capacity; PEEP: positive end-expiratory pressure. The action of expiratory muscles can also be analyzed from a synergistic functional perspective with inspiratory muscles. Abdominal muscles are recruited for inspiratory function when the diaphragm is unable to generate sufficient force. In this scenario, this muscle group is recruited in an orderly and hierarchical manner to orient the diaphragm towards a more cephalic position, reducing its radius of curvature; thereby, according to Laplace's law, enhancing the ability to exert tension (i.e., positioning the diaphragm at a mechanical advantage to generate force). This ordered recruitment pattern is initially observed with the action of the transversus abdominis muscle, followed by the internal and external oblique muscles, and finally, the rectus abdominis muscle. Although the action of this muscle group assists in lung deflation, when a "forced expiration" is evidenced, and in the absence of obstructive events, the clinical picture may be interpreted as an increase in respiratory work secondary to diaphragmatic positional dysfunction. The elastic energy accumulated by the contraction of this muscle group will result in a decrease in EELV below the CRF, thus, returning to the physiological equilibrium point will lead to a decrease in pleural pressure that aids in initiating the subsequent inspiration. The foregoing highlights the intimate relationship between the diaphragm and abdominal muscles. This close link can also be observed during normal spontaneous ventilation, where, upon diaphragmatic contraction, visceral contents tend to move caudally and forward, being restrained by the "containment barrier" offered by the abdominal musculature. Thus, the diaphragm gains support from the abdominal viscera and can activate the more peripheral fibers, allowing for the "bucket-handle" movement of the lower ribs, thereby increasing the transverse and anteroposterior diameter of the thoracic cage. The consequences of expiratory muscle activation are not always beneficial. There are several unfavorable circumstances (which should be avoided), such as increased pleural pressure, decreased EELV, atelectasis formation, increased CO2 production, and energy expenditure. The correct balance between respiratory center activity and mechanical ventilatory assistance will be crucial to counteract deleterious effects and optimize the benefits of expiratory muscle action. Expiratory muscles are frequently recruited in critically ill patients requiring mechanical ventilatory assistance, where there is a discrepancy between ventilatory demands and the programmed settings on the ventilator. This text aims to arouse specific interest in the action of expiratory muscles, although the physiological and pathophysiological analysis of the harmonious interplay between respiratory muscles (inspiratory and expiratory) and the ventilator should be part of daily clinical practice. The clinical implications arising from the imbalance between the load and the capacity of respiratory muscles to work can be potentially detrimental. It is the responsibility of critical care professionals to understand the two sides of the coin derived from mechanical ventilation, always seeking to maximize benefits, minimize deleterious effects, and optimize outcomes for their patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
