
Case Report | DOI: https://doi.org/10.31579/2692-9759/055
Department of Cardiology, Bay Care Clinic Green Bay, Wisconsin, USA
*Corresponding Author: Timothy E Paterick, Department of Cardiology, and Bay Care Clinic Green Bay, Wisconsin, USA
Citation: Timothy E Paterick (2022) The Bicuspid Aortic Valve – Various Phenotypic Expressions J. Cardiology Research and Reports 4(5); DOI: 10.31579/2692-9759/055
Copyright: © 2022 Timothy E Paterick, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 April 2022 | Accepted: 26 April 2022 | Published: 31 May 2022
Keywords: bicuspid aortic valve; aortopathy; coarctation; heterogeneity; genotype; phenotype
The phenotypic expressions of the bicuspid aortic valve (BAV) are unpredictable, and difficult to compartmentalize. In current times the BAV is noted to represent approximately 50% of isolated severe aortic stenosis cases requiring surgery, and has been associated with aortic regurgitation, bacterial endocarditis and aortic dissection. Echocardiography is the diagnostic test to identify BAV. The clinical associations coupled with the high prevalence of BAV have made this an important area of clinical inquiry. We will explore the vast horizons and multifaceted challenges of the bicuspid aortic valve and our current understanding of this complex entity.
The phenotypic expressions of the bicuspid aortic valve (BAV) are unpredictable, and challenging to compartmentalize. In contemporary times the BAV is noted to represent approximately 50% of isolated severe aortic stenosis cases requiring surgery, and has been associated with aortic regurgitation, bacterial endocarditis and aortic dissection [1, 2]. Echocardiography is the diagnostic test to identify BAV. [3] The clinical associations coupled with the high prevalence of BAV have made this an important area of clinical inquiry.
The heterogeneous clinical presentations, varied valvuloaortopathies with wide-ranging phenotypes and unpredictable outcomes, uncertain natural history, and ambiguity as to whether it is an innocent bystander or a primary disease make the bicuspid valve an enigmatic clinical challenge to even the expert clinician [2]. We will present five cases that attempt to explore the multifaceted faces of the bicuspid aortic valve and our current understanding of this complex entity.
The clinical presentations and effects of BAV are diverse with few clinical or genetic indicators to predict outcomes or associated complications. BAV can be diagnosed at any stage of life from newborn to octogenarian and may be related to inconstant clinical circumstances [4]. The spectrum of identification is vast ranging from a heart murmur in an asymptomatic patient to severe aortic valve disease manifesting as heart failure. Life threatening associations include bacterial endocarditis and thoracic aortic aneurysm dissection [5, 6]. The variable clinical presentations and the various phenotypic expressions make the diagnosis and management of BAV a challenge for physicians.
Bav Is a Valvuloaortopathy with Diverse Phenotypic Expressions and Arbitrary Outcomes
The high incidence and prevalence of BAV requiring surgical intervention and the high incidence of associated thoracic aortic aneurysm formation mandates that it be viewed as a valvuloaortopathy for an orderly relationship among phenotypic disease expressions.
The BAV has various phenotypic expressions (7), which are classified as:
The two cusps of most BAVs exhibit asymmetrical systolic excursion and eccentric systolic flow pattern.
The ascending aorta displays a spectrum of aneurysmal phenotypes, tubular ascending aorta dilatation being the most common (60-70%) and exhibiting the fastest growing rate (.4-.6 mm/year). There is also a sinus of Valsalva dilatation phenotype (approximately 25% of dilated aortas) and it associated with Type 1 BAV and male sex [8,9,19,11]. Aortic phenotypes encountered in BAV include:
The underlying mechanisms responsible for such varied BAV associated valvuloaortic phenotypes remains enigmatic. There is a major knowledge deficit and it remains a mystery as to why a BAV becomes stenotic, another regurgitant, another associated with a TAA, and yet another remains functional. Most perplexing is the lack of insight into why a few BAV patients will incur aortic dissection and that aortic diameters are modestly predictive at best [12].
BAV is associated with congenital and genetic syndromes with cardiovascular manifestations such as ShoNes complex, coarctation, ventricular septal defect, anomalous pulmonary veins, and syndromic conditions such as familial TAA, Loeys- Dietz, Turner’s and aortic dissection due to smooth muscle alpha actin (ACTA2) gene mutation. There has been identification of Notch1 and GATA5 gene in families with BAV [13, 14, 15, 16]. But the genomic causes and their clinical manifestations remain largely unknown. There may be very different genomic substrates that lead to more complex conditions in children and isolated BAV, or BAV associated aortopathy in adults. It is a mystery why some children have severe BAV dysfunction, an adult may have moderate BAV disease and develop aortic dissection, and a 91-year-old is incidentally found to have a BAV that functions essentially normal. It is clear that genetic and environmental factors play a role and that pathogenetic economy is not occurring.
Expert consensus opinion suggests that the following management principles are the best available evidence - based medicine for BAV.
Herein we present six cases of BAV with a succinct history, physical examination, multi-modality imaging and clinical decision making elucidating the points outlined above.
Clinical presentation:
43-year-old male presented for evaluation of fatigue. He denied chest pain, dyspnea, palpitation or syncope. The patient was referred for aortic valve replacement for severe aortic stenosis.
Examination:
Blood pressure 130/80 Pulse 80 bpm
Normal JVP, normal carotid upstroke, and normal S1 and S2, 2/6 systolic ejection murmur at the base.
Echocardiography:
Normal LV size and systolic function
Bicuspid aortic valve
Peak AV velocity = 4.6 m/sec
AV mean gradient = 43 mm Hg
LVOT-tvi = 23 cm
Calculated AVA (continuity equation) = 1 cm2
Genetics: Negative for NOTCH1, ACTA2, KCNJ2, and GATTA5
Clinical Decision-making:
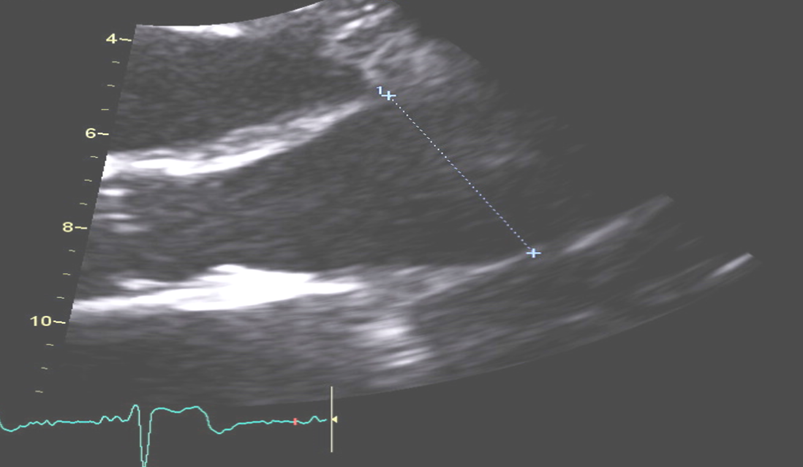
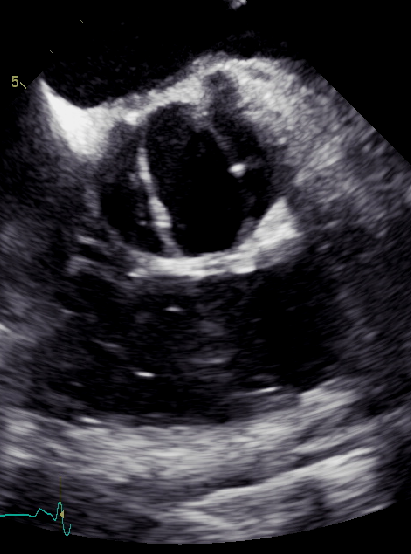
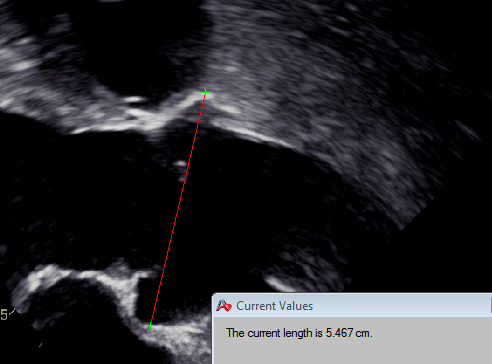
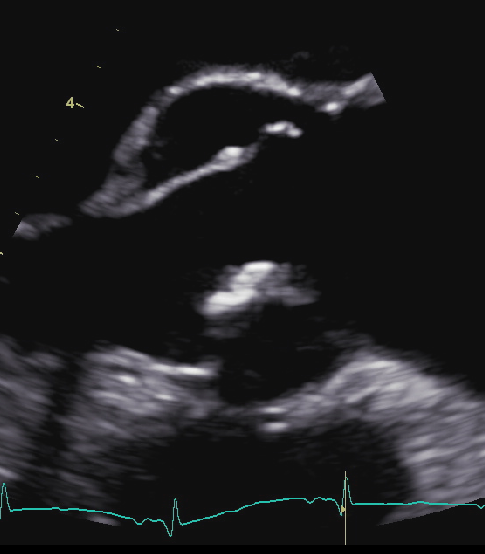
The echo revealed a type 2 bicuspid AV (Figure 1) and the ascending aorta revealed a tubular phenotype that measured 38 mm (Figure 2).

Type 2 bicuspid aortic demonstrating the right and left coronary cusps
Ascending aorta measuring 38 mm
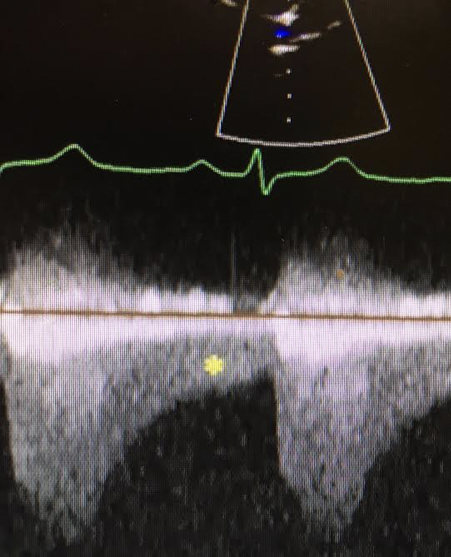
Doppler data revealed a peak velocity of 4.6 m/sec (Figure 3). The calculated valve area using the continuity equation was 1 cm2. The planimetry of the AV revealed a normal valve area. (Figure 3) and visualization revealed a normal valve excursion. (Cine 1) The calculated valve area and the visual appearance were discordant.
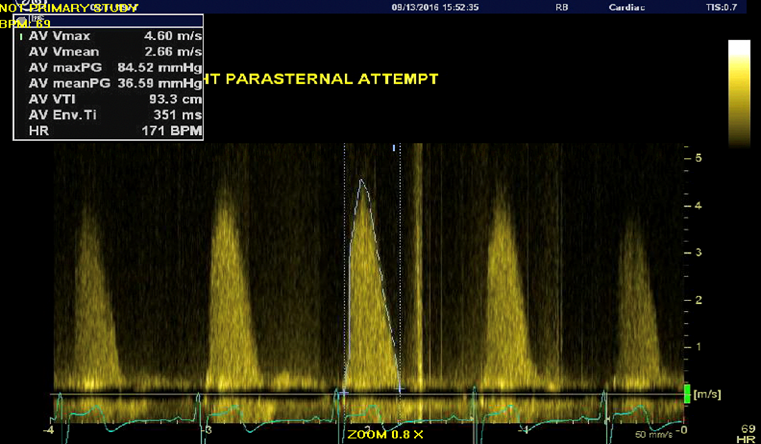
Continuous wave Doppler from the suprasternal notch across the AV
The visualization of the AV reveals there is no aortic stenosis. So why is the gradient elevated?
Clinical presentation:
47-year-old male presents with exertional dyspnea and fatigue for approximately one year.
Examination:
Blood pressure 140/60 Pulse 75 bpm
Carotid: rapid upstroke with rapid collapse Normal JVP
3/4 blowing holodiastolic diastolic murmur
Brisk femoral pulses with systolic and diastolic sounds
Echocardiography:
Mild LV dilation with preserved LV systolic function Type 2 bicuspid AV with leaflet prolapse and severe eccentric AV regurgitation and enlarged aorta involving the sinus of Valsalva and tubular aorta with effacement of the Sino tubular junction measuring 43 mm.
Cardiac catheterization:
Normal coronary arteries
Genetics: Positive for G4.5 (Tafazzin) Negative for NOTCH1, ACTA2, KCNJ2, and GATTA5
Clinical Decision-making:
47-year-old with type 2 BAV (Figure 4) and dilated ascending aorta involving the sinus of Valsalva and tubular aorta with sinotubular junction effacement and measuring 44 mm.
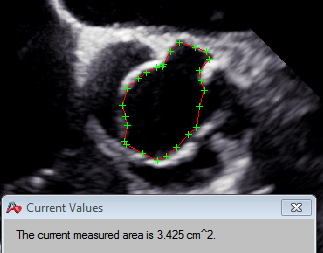
Planimetry of the AV with AVA ~ 3.4 cm2
(Figure 5) The patient had LVNC with normal systolic function. (Cine 2) The BAV prolapsed (cine 3) and revealed severe eccentric aortic regurgitation.

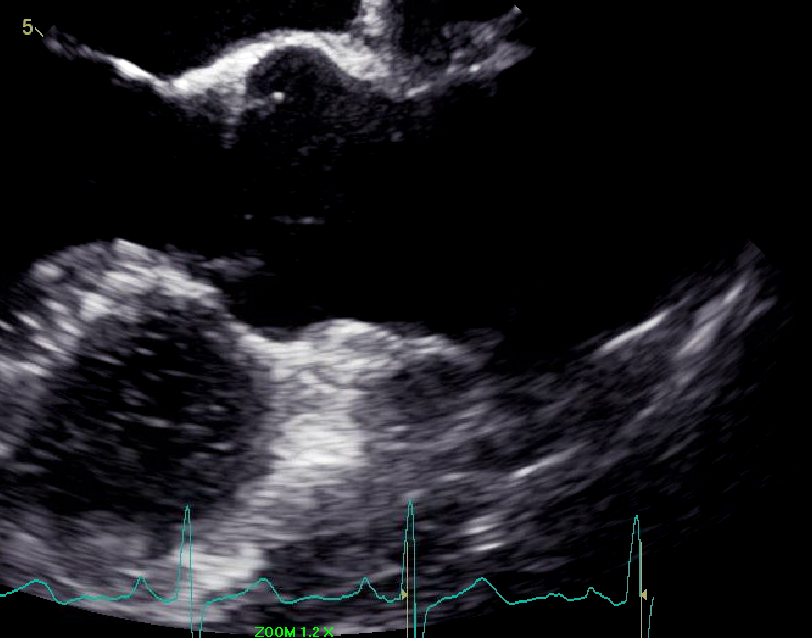
Phenotype: Type 2 bicuspid AV still frame in systole demonstrating right and non-coronary cusp fusion
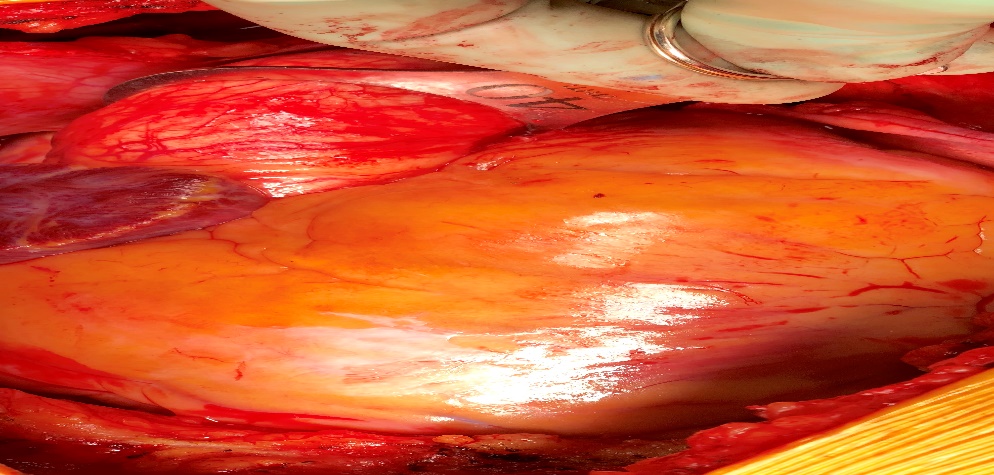
(Cine 4,5) The debate was whether to proceed with a Bentall operation or AVR with aortic wrapping. The TEE suggested a maximum aortic dimension of 44 mm. A CT scan was obtained and measured 43 mm as the maximum dimension of the ascending aorta. (Figure 6).
Dilated ascending aorta measuring 44 mm with a phenotype involving the entire ascending aorta: involving the sinus of Valsalva
The guidelines recommend aortic root replacement at 45 mm or greater. These guidelines are non-evidenced based and extrapolated from the Marfan guidelines. In type 1 BAV there is data suggesting it is associated with rapid aortic root dilation. Since the valve was type 2 the debate persisted and it was decided the decision would be made at surgery. (Figure 7) The maximum dimension was 40 mm at surgery and according to guidelines an AVR with aortic root wrap was performed. The guidelines for post -operative imaging of the aortic root were recommended.
Cardiac tomography of the ascending aorta measuring 43 mm
Clinical presentation:
57-year-old female presented with six-month history of dyspnea. She also had a history of vasodepressor syncope, diabetes and pulmonary sarcoidosis. Her father had a bicuspid valve.
Examination:
Blood pressure 150/50 Pulse 76 bpm
Carotid upstroke is bounding with rapid collapse
S1 S2 RRR with water hammer pulses
2/4 diastolic murmur
Echocardiography:
Mildly dilated LV cavity
LVEF = 50%
Elevated LV filling pressure manifest as early closure of the mitral valve
Bicuspid AV with eccentric aortic regurgitation
Genetics: Negative for NOTCH1, ACTA2, KCNJ2, and GATTA5
Cardiac catheterization:
Normal coronary arteries
Aortography: Severe aortic regurgitation
Clinical Decision-making:
57-year-old female with type 2 bicuspid aortic valve (Figure 8) and tubular ascending aorta measuring 45 mm
Intraoperative assessment of the ascending aorta measuring 40 mm
(Figure 9) and prolapsing AV (Cine 6) with eccentric AR. (Cine 7,8) There was a difference of opinion regarding the severity of the AR from echocardiographic imaging.
The clinical examination suggested severe AR and that was confirmed by aortography. (Cine9). The constellation of finding of severe aortic regurgitation and an ascending aorta measuring 45 mm led to a recommendation for a Bentall procedure.

Phenotype: Type 2 bicuspid AV still frame in systole demonstrating right and noncoronary cusp fusion.
Clinical presentation:
62-year-old male presented with increasing fatigue and shortness of breath and a heart murmur. He had a brother with an aortic valve replacement for bicuspid valve.
Examination:
Blood pressure 130/85 Pulse 85 bpm
JVP normal Carotid upstroke normal
S1 S2 RRR with normal pulse
1/4 diastolic murmur with the patient leaning forward from a sitting position
Echocardiogram:
Normal LV size and systolic function
Type 1 bicuspid AV with trivial to mild aortic regurgitation
Dilated sinus of Valsalva measuring 53 m
Genetics:
Negative for NOTCH1, ACTA2, KCNJ2, and GATTA5
Clinical Decision-making:
62-year-old male with type 1 bicuspid aortic valve (Figure 10) and isolated dilation of the sinus of Valsalva measuring 53 mm (Figure 11) and mild aortic regurgitation. (Cine 10,11,12,13). The recommendation was repeat echocardiogram in 6 months because predominant sinus of Valsalva dilatation phenotype is associated with type 1 bicuspid aortic valves and male sex. This root phenotype has been associated with faster tubular ascending root dilation.

Ascending aorta is tubular phenotype with maximum dimension measuring 45 mm
Phenotype: Type 1 bicuspid AV still frame in systole demonstrating right and left cusp fusion
Clinical presentation:
65-year-old male presented for evaluation of recalcitrant hypertension and exertional shortness of breath. His blood pressure was 160 systolic despite treatment with Dilacor XR 240 mg/day, Toprol XL 100 mg/day, Lisinopril 40 mg/day and Hydrodiuril 25 mg/day.
Examination:
Blood pressure 170/88 Pulse 75 bpm
Normal JVP Normal carotid upstroke
S1 S2 S4 2/4 SEM
Pulses revealed brachial femoral delay
Echocardiogram:
Normal LV size and systolic function
Increased LV wall thickness: septum and posterior wall measure 15 mm
Bicuspid aortic valve with mild aortic regurgitation
Dilated sinus of Valsalva and ascending aorta with effacement of the sinotubular junction – maximum dimension of the aorta is 45 mm
The aortic arch is poorly visualized
PW Doppler of the abdominal aorta revealed decreased pulsatile flow and continuous flow in diastole
Cardiac catheterization:
Mild coronary artery disease
Genetics:
Negative for NOTCH1, ACTA2, KCNJ2, and GATTA5
Clinical Decision – making
65-year-old male with type 3 bicuspid aortic valve (Figure 12) and dilated sinus of Valsalva with tubular ascending aorta and effacement of the sinotubular junction (Figure 13).
Ascending aorta phenotype isolated dilation of the Sinus of Valsalva

Phenotype: Type 3 bicuspid AV still frame in systole demonstrating left and noncoronary cusp fusion
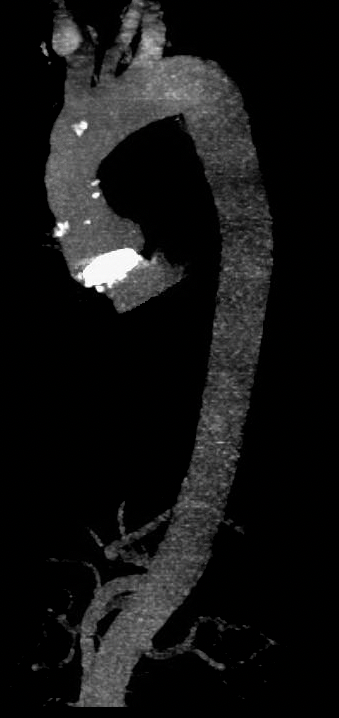
He had resistant to medical therapy hypertension propting a concern for a secondary etiology. Transesophageal short axis and long axis imaging revealed mild, eccentric aortic regurgitation. (Cine 14, 15) PW Doppler in the abdominal aorta raised a suspicion of coarctation of the aorta. (Figure 14) MRI imaging revealed a coarctation. (Figure 15)
The recommendation was an evaluation by the interventional and surgical team for repair of the coarctation.
Phenotype of the dilated ascending aorta measuring 45 mm with a phenotype involving the entire ascending aorta: involving the sinus of Valsalva and tubular aort
PW Doppler of PW Doppler of the abdominal aorta limited pulsatile flow a continuous flow in diastole

MRI of the thoracic aorta demonstrating coarctation
The presented case explores the various phenotypic expressions of the bicuspid aortic valve, The cases identify how the clinical presentation, physical examination and multi-modality imaging allow the clinician to make the diagnosis and enlightened clinical decisions regarding surgical treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
