
Research | DOI: https://doi.org/10.31579/2578-8949/079
1 Department of Dermatology, Venereology, and Andrology, Faculty of Medicine, Assiut University, Assiut, Egypt
2 Department of Public Health and Community Medicine, Faculty of Medicine, Assiut University, Assiut, Egypt
*Corresponding Author: Abou-Taleb DAE, Department of Dermatology, Venereology, and Andrology, Assiut University Hospital, 71515 Assiut, Arab Republic of Egypt.
Citation: Abou-Taleb DAE, Moubasher AEA, Ibrahim AK, Youssef EMK. (2021) The Arabic Version of MELASQoL Scale: Translation, Cultural Adaptation, with Assessment of Reliability and Validity. Dermatology and Dermatitis. 6(2); Doi:10.31579/2578-8949/079
Copyright: ©2021 Abou-Taleb DAE, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 June 2021 | Accepted: 09 July 2021 | Published: 13 July 2021
Keywords: melasma; quality of life; questionnaire; reliability; validity
Background: Melasma has significant emotional and psychological effects and significant negative impact on patients’ quality of life (QoL). Melasma QoL Scale (MELASQoL) is a specific questionnaire that has been developed to assess the effect of melasma on patient’s QoL.
Objective: Translation, cultural adaptation, reliability and validation of melasma specific QoL sale (MELASQoL) into Arabic.
Patients and Methods: A total of 65 adult Egyptian female patients with melasma aged ≥18 years old with skin phototypes type III-V were enrolled in this study. Wood’s light was used for determination of the type of melasma either epidermal, dermal or mixed. Melasma severity was assessed by using the melasma area and severity index (MASI) score and the new modified score (mMASI). The impact of melasma on QoL was evaluated using the Arabic version of MELASQoL scale after translation and cultural adaptation according to the WHO guidelines. The questionnaire’s reliability and validity was assessed.
Results: The internal consistency for the 10-item of the MELASQoL-A scale was excellent; Intra-class Correlation Coefficient (ICC) = 0.914 and Cronbach’s alpha coefficient (Cronbach α = 0.944) indicating high reliability of the developed Arabic version. There was significant positive correlation between the MELASQoL-A scale and the MASI score (r= 0.41; p= 0.0027), and the mMASI score (r = 0.36; p= 0.0032).
Conclusion: The Arabic version of the MELASQoL scale was found to be a reliable and valid measure for evaluating the QoL among Egyptian melasma patients, supporting its use in Arab communities.
Quality of life (QoL) is a term which involves many items, including social well-being, psychosocial and family relationships [1, 2].
Many dermatological diseases are characterized by compromising patients’ physical and relational well-being. For this reason, the assessment of QoL is of great importance [3, 4].
Most questionnaires used to assess the QoL were developed for English speaking populations. So, they are not adequate in terms of correct translation to the reality of other countries. These questionnaires have to be translated and culturally adapted in order to be applied for each specific community [5, 6].
Melasma is a common cosmetic problem. It is an acquired, chronic, recurrent hyperpigmentary disorder, which is characterized by brown patches of variable darkness on sun exposed areas of the body, typically occurs on the face. It is more common in women, and appears in all racial types. It is found mostly in women with Fitzpatrick skin photo-types IV and V living in areas of marked ultraviolet ray’s exposure [7, 8].
It has a significant emotional and psychological effects and highly compromises patients’ QoL. It is usually psychologically distressing and affects patients’ social interactions [9].
A new health-related quality of life (HRQoL) questionnaire for melasma, a melasma specific scale which is Melasma Quality of Life Scale (MELASQoL) has been developed (English version) [10].
The Dermatology Life Quality Index (DLQI) and SKINDEX-16 are general questionnaires of the impact of skin disease on the HRQoL of patients with different skin diseases; they put equal weight on the psychological and physical effects of a dermatological condition. The developed MELASQoL scale uses items from the SKINDEX-16 and the skin discoloration questionnaire, which focus on items that would be more relevant to melisma [10].
MELASQoL is a 10 question scale, which asks patients to rate how they feel about each issue on a scale from 1 (not bothered at all) to 7 (bothered all the time). The score obtained in the answers ranges from 10 to 70 with the higher scores indicating the worst QoL [10, 11]. This questionnaire has been translated into Spanish [11], Brazilian Portuguese [12, 13], French [14] and Turkish [15] languages. However, there is no available Arabic version of that questionnaire to assess the melasma patients’ QoL in Arab communities where melasma is a common distressing disease.
The objectives of this study were to translate and to adapt the MELASQoL scale to Arabic language, and to assess the reliability and validity of the Arabic version of the (MELASQoL-A) scale.
This cross-sectional study was conducted at the department of Dermatology, Venereology and Andrology, Assiut University Hospital (AUH), Assiut, Egypt. The study design was approved by the Institutional Ethics and Research Committee of the Faculty of Medicine, Assiut University and was carried out in accordance with the guidelines of the Helsinki Declaration.
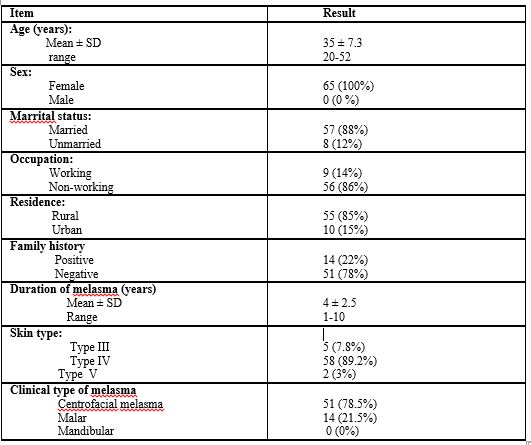
A total of 65 adult female Egyptian patients with melasma aged ≥18 years old, with Fitzpatrick skin photo-types III-V were randomly recruited from dermatology outpatient clinic of AUH. They were included in the study after signing the informed consent form. A detailed history regarding age, occupation, marital status, residence, duration of complaints, precipitating, exacerbating factors and family history were taken. A dermatologic examination was performed to clinically classify the type of melasma into centrofacial, malar, or mandibular patterns. The severity of melasma was determined for each patient using Melasma Area and Severity Index (MASI) score16 and the modified (mMASI) score [8, 17].
The impact of melasma on QoL was assessed using the Arabic version of the questionnaire (MELASQoL-A) after translation and cultural adaptation.
Development of the Arabic version of the MELASQoL followed the World Health Organization (WHO) guidelines for scale development as follows [5,6,11]: Forward translation, expert panel back-translation, pre-testing and cognitive interviewing, development of the final version.
1) Forward translation
Two translators produced independent Arabic-language translations of the English version of MELASQoL questionnaire, the translated version has been reviewed by a committee of experts who developed a unique Arabic language translation and modified some items to make them more culturally appropriate. Some changes were made, for example, “melasma” was substituted for “skin condition” because the latter term might be interpreted as meaning another skin disease. Finally, the face validity of the questionnaire was confirmed by its application on a sample of patients using an interview technique. The patients who were interviewed, expressed their well-understanding for the each item of the MELASQoL questionnaire.
2) Expert panel back-translation
A back-translation (from Arabic to English) was performed by other two translators, to verify that the original questionnaire could be reinstated without any major modification and without alteration of the original items and few changes were made, for example, “Frustration and affection” were back translated to “Disappointment and emotion” respectively. This back-translation was submitted to the developer of the original questionnaire (Balkrishnan, R) [10] for review and comments and he agreed and approved the back translation.
3) Pre-testing and cognitive interviewing
Qualitative pre-testing of the revised Arabic version of the MELASQoL was carried out with 20 Egyptians female patients with melasma to determine whether each question was correctly understood, patients were asked to justify their answers and explain what the questions meant in their own words.
4) Final Arabic version
Reliability and validity of the final Arabic version (MELASQoL-A) scale have been conducted.
Finally, the Arabic version of the MELASQoL questionnaire (as shown in the appendix) was distributed to a total of 65 female patients with melasma. On a 7-point Likert scale; 1 (not bothered at all) to 7 (bothered all the time). Each patient rates how she feels about each item. The total MELASQoL-A score ranges from 10 to 70 with higher score indicating worse QoL related to melasma.
All analyses were carried out using using SPSS version 21. Internal consistency of the scale was assessed using Cronbach’s alpha coefficient. Item analysis was performed, and Cronbach α [18, 19] was calculated for the total MELASQoL-A scale and for separate domains. Confirmatory Factor Analysis (CFA) was conducted to confirm the separate factors within the scale. Each item within a factor was judged to be worthy of retention in a scale according to its power to explain variation between subjects. To study the construct validity of the scale, Spearman’s Rank Correlation coefficient was used to test for any association between MELASQoL-A score, MASI score and mMASI score with age, marital status, occupation, residence and clinical type of melasma. As regards p-value; p<0>
A 65 adult Egyptian female patients with melasma participated in the study. The age of these patients ranged from 20 to 52 years old with a mean + SD of (35 ± 7.3). The proportion of women ≤ 40 years old was 53 patients (81.5%), and those > 40 years old 12 patients (18.5%). The duration of melasma ranged from 1-10 years with a mean ± SD of (4 ± 2.5). The demographic data of the study is shown in (Table 1).
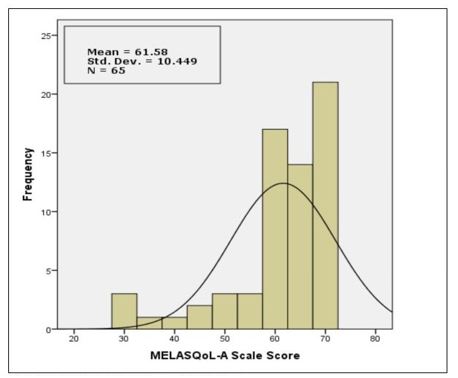
The distribution of the MELASQoL-A scale among all patients
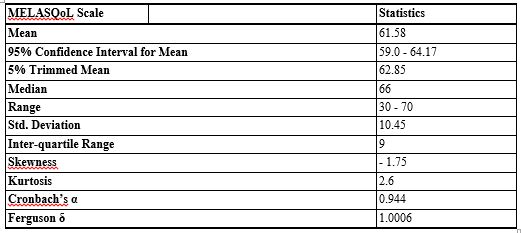
The distribution of the MELASQoL-A for the 65 patients is shown in (Table 2 and Fig. 1). The mean was 61.58 (SD= 10.45), 95% Confidence Interval for Mean (59.0 - 64.17) and ranged from 30 to 70. The spread of scores was not normally distributed (skewness = - 1.75 and kurtosis = 2.6).
Scale reliability
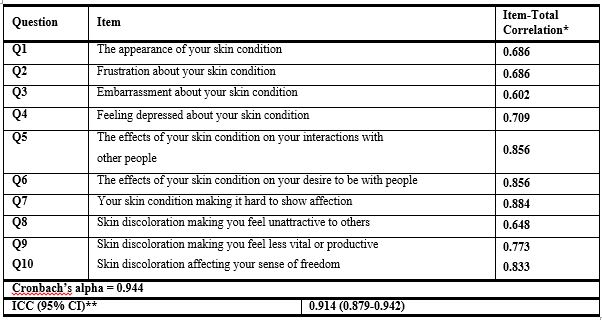
The internal consistency for the 10-item of the Arabic version of the questionnaire MELASQoL-A was excellent; Intra-class Correlation Coefficient (ICC) = 0.914 and Cronbach’s alpha coefficient (Cronbach α = 0.944) indicating high reliability of the developed Arabic version. The 10 items of the MELASQoL-A scale showed high item-total correlations (>0.3) and high Cronbach α (> 0.6). Reliability statistics for the main domains of the 10 items of MELASQoL-A scale were satisfactory, ranging from acceptable (> 0.5) to very good (between 0.8 and 0.9) as expressed by (Table 3). However, Cronbach α for the total scale = 0.944 was not improved by removal of any of the items [20].
*< 0>
** ICC (95% CI) **=Intra-class Correlation Coefficient (95% Confidence Interval)
For the first scale domain (emotional well-being), that contained 4 items, Cronbach α =0.930 and ICC = 0.915. While the second domain (social life), that had 3 items, had Cronbach α = 0.971 and ICC = 0.971. The last domain (Recreation & leisure), that contained 3 items had Cronbach α = 0.800 and ICC = 0.834, as shown in (Table 4).
The original MELASQoL scale (English version) proposed that melasma
affects mainly three domains of QoL; emotional well-beings, social life and recreation and leisure [10].
The Arabic version (MELASQoL-A) was similarly found that melasma mostly affected patients’ emotional well-beings (Cronbach α = 0.930) and social life (Cronbach α = 0.971) and to lower extent recreation and leisure (Cronbach α = 0.800) as shown in (Table 4).

*<0>
Factor analysis
Factor analysis was therefore conducted with all 10 items. The first factor (factor I) (4 items, corresponding to emotional well-being) explained 66.4% of the variance, the second factor (factor II) (3 items, corresponding to social life) explained 14.9% of the variance, the third factor (factor III) (3 items, corresponding to recreation & leisure) accounted for 7.9% of the variance, as shown in (Table 5). The results of Confirmatory Factor Analysis Scree Plot using Principle Component Analysis, confirmed that the main scale domain has a “leveling off” of eigenvalues after the first factor (factor I) (Fig. 2).
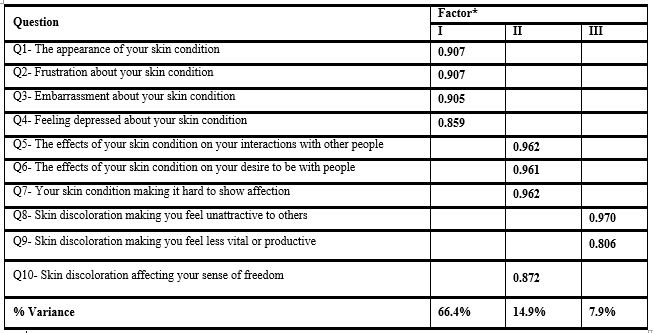
*Factor loadings < 0>

Construct validity of the MELASQoL-A scale
The construct validity of the Arabic version of the questionnaire (MELASQoL-A) showed that higher MELASQoL-A scale scores was significantly correlated to rural residence (correlation coefficient; r= 0.31), non-working patients (r= 0.32) and those with centrofacial melasma (r= 0.43). There was significant positive correlation between the MELASQoL-A scale and the MASI score (r =0.41; p= 0.0027), and the mMASI score (r = 0.36; p= 0.0032), as shown in (Table 6).
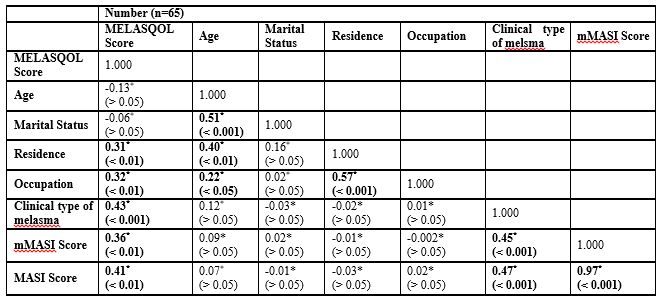
*Spearman Correlation is significant at the 0.05 level (2-tailed).
Melasma is a common disorder of hyper-pigmentation affecting millions of people worldwide [7, 8] It may cause significant psychological distress and has a significant impact on the QoL [13].
This study discussed the Arabic version of the MELASQoL scale and evaluated its reliability and validity among Egyptian melasma patients. It was found that it is a reliable and valid measure for evaluating the QoL among Egyptian melasma patients, supporting its use in Arab communities. The Arabic version of the questionnaire was developed using a sample of patients mostly with skin type IV, so it provides information related mostly to this skin photo-type and to lower extent on the other skin phototypes.
The Arabic version of the MELASQoL questionnaire was easily understood and answered by the patients. The mean of MELASQoL-A score in this current study was 61.58 (Standard deviation = 10.45), higher than that measured in an English speaking patients in a previous USA study was 36 [10], Brazilian patients was 37.5 [13], French patients was 20.9 [14] and Turkish patients was 29.9 [15] suggesting that Egyptian patients are at higher risk to suffer from negative emotional well-being and impaired social functions because of melasma.
The internal consistency for the 10 items of the developed Arabic version (MELASQoL–A) was excellent (ICC= 0.914 and Cronbach α = 0.944). This reflects its usefulness and its high internal consistency to discriminate different domains of the patient’s QoL. Our findings regarding the internal consistency and the scale reliability were approximate to those reported by Cestari et al. (2006) (Cronbach α = 0.919) of the Brazilian Portuguese version [12], by Misery et al. (2010) (Cronbach α = 0.95) and (ICC= 0.88) of the French Version of MELASQOL [14], and that reported by Dogramaci et al. (2009) (Cronbach α = 0.88) of the Turkish version [15].
Our results of the excellent internal consistency for the 10-item of the Arabic version of the questionnaire (MELASQoL-A); (ICC = 0.914 and Cronbach α = 0.944) and the results of Confirmatory Factor Analysis Scree Plot using Principle Component Analysis, confirmed that the main scale domain has a “leveling off” of eigenvalues after the first factor (factor I), suggesting that the questionnaire should be of a single domain instead of the three domains more likely to be affected by melasma suggested by Balkrishnan et al. (2003), regarding emotional well-beings, social life and recreation and leisure [10].
There was significant positive correlation between the MELASQoL-A scale and the MASI score (r =0.41; p= 0.0027) and the (mMASI) score (r = 0.36; p= 0.0032). This suggests that patients with severe degree of melasma were more likely to have poorer QoL. This was in contrast to the results of other studies reported that the effect of melasma on QoL was not correlated with the severity of melasma. The authors explained that even a small amount of pigmentation can cause a significant emotional effect [12, 13].
The Arabic version of the MELASQoL scale was found to be a reliable and valid measure for evaluating the QoL for Egyptian melasma patients. The evaluation of the QoL in melasma patients, by means of a dermatosis specific instrument, could bring a new comprehension of the results of different treatment modalities aimed to improve the severity of melasma and thus improve the patients’ QoL.
Conflicts of interest:
The authors report no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
