
Mini Review Article | DOI: https://doi.org/10.31579/2641-0419/167
*Corresponding Author: Ehsan Khalilipur, M.D, Cardiovascular intervention research center, Rajaie cardiovascular medical and research center, Iran university of medical sciences, Tehran, Iran.
Citation: Zahra Khajali, Ata Firouzi, Zahra Hosseini, Ehsan Khalilipur (2021) The Appropriate Approach to Dual Drainage Partial Anomalous Pulmonary Venous Connection. J. Clinical Cardiology and Cardiovascular Interventions, 4(10); Doi:10.31579/2641-0419/167
Copyright: © 2021 Ehsan Khalilipur, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 April 2021 | Accepted: 10 May 2021 | Published: 14 May 2021
Keywords: partial anomalous pulmonary venous connection; vascular plug
Partial Anomalous Pulmonary Venous Connection (PAPVC) is a remarkably unusual congenital disorder in which the venous circulation is connected with one or more pulmonary veins. Approximately 90% of all PAPVCs start from the right lung, 7% start from the left lung, and 3% of patients are found to have two-side PAPVCs. Occasionally, PAPVC can be treated percutaneously employing an occlusion device, with regard that when there is a dual drainage PAPVC. Here, we want to share our experience in 5 dual drainages PAPVC patients whose 2 right-sided PAPVC's with dual drainage closure were unsuccessful. We also reviewed all published cases which were tried to treat percutaneously to build a pathway in which percutaneous closure is more feasible in addition to inhibit futile efforts.
Partial anomalous pulmonary venous connection (PAPVC) is an amazingly uncommon congenital condition where one or more of the pulmonary veins are associated with venous circulation. Its prevalence inside the common population is 0.4%–0.7% [1]. Roughly 90% of all PAPVCs begin from the right lung, 7% begin from the left lung, and 3% of patients are found to have two-sided PAPVCs beginning from both lungs interfacing to the superior vena cava (SVC), inferior vena cava (IVC), the right chamber, or the innominate vein [2,3]. PAPVCs are frequently related to the atrial septal defect and are once in a while related to other congenital anomalies [4,5].
Echocardiography is the initial methodology of choice for noninvasive detection of PAPVC but cardiac MRI or CT guides physicians for more detailed diagnosis [5–7]. For the most part, patients with a PAPVC, in case symptomatic or showing noteworthy left-to-right shunting, are treated with surgery [8]. Occasionally, it is conceivable to treat PAPVC percutaneously by implies occlusion devices, although this is feasible when there is a dual drainage pathway to both systemic veins and left atrium [9]. To our information, as it were few such cases have been depicted within the latest publications [10]. Here, we want to share our experience in 5 dual drainages PAPVC patients and we also reviewed all published cases which were tried to treat percutaneously.
Dual drainage PAPVC- types and review of literature
The regular arrangement of pulmonary veins consists of four partitioned pulmonary veins: right and left superior and inferior veins, which drain exclusively into the left atrium. This anatomical categorization is found in 60%–70% of the general population [11]. PAPVC is the abnormal connection of at least one but not all pulmonary veins into the right-sided venous system or right atrium. Right-sided atypical drainage happens into any central vein. The foremost common frame of PAPVD is the bizarre seepage of the RSPV into the superior vena cava (SVC). This anomalous drainage frequently happens at the junction of SVC and RA. Occasionally, drainage happens at a higher level at the intersection between the SVC and brachiocephalic vein over the level of the azygos vein [12].
The most common pattern on the left side is the connection of LSPV to the brachiocephalic vein [13].
The conventional classification of PAPVC does not categorize “dual drainage” independently and these variations, with a combination of supracardiac and cardiac PAPVC, are amazingly uncommon with exceptionally few previous case reports experienced [10, 14]. Moreover, the genuine rate of PAPVC cases with double drainage is troublesome to assess, since patients are regularly asymptomatic and elude detection.
Cautious investigation of the pulmonary veins is mandatory and the distinguishing proof of less than four pulmonary veins connected to the left atrium ought to alarm the clinician to a diagnosis of PAPVC. In the presence of a left-to-right shunt, enlargement of the right chambers happens due to expanded volume overload. Besides, the vessel receiving the atypical vein would be enlarged and there may be asymmetry of the pulmonary veins [15,16]. What has been reported in cases of transcatheter closure of dual drainage PAPVC and what we have experienced in our center are these anatomical variations:
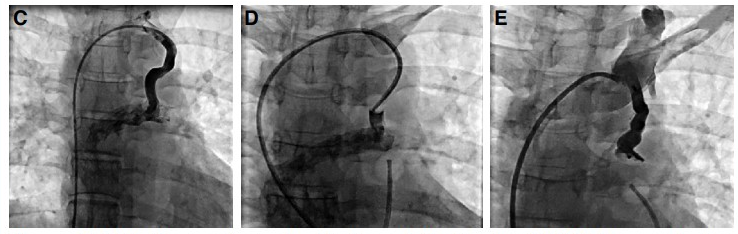
- right-sided PAPVC with connection to SVC at the level of RA junction with a distinguished connection to LA: in this rare variation in a 60-year-old lady with a complaint of dyspnea on exertion and right-sided chambers dilatation, we decided to occlude the abnormal pathway with ventricular septal occluder device but because of the very short pathway between PAPVC and SVC junction to RA release of the device was not feasible and the procedure was terminated (figure-1).

We also experienced this variation with another patient in whom he was a 70-year-old man referred for more evaluation because of RV failure symptoms. He was diagnosed with a dual drainage PAPVC at the SVC and RA junction and a closure try with a VSD device was unsuccessful. Theoretically, it was amenable to deploy a stent graft in the distal part of the SVC to occlude the ominous pathway, but the long-term patency of this graft in this scenario is vague.
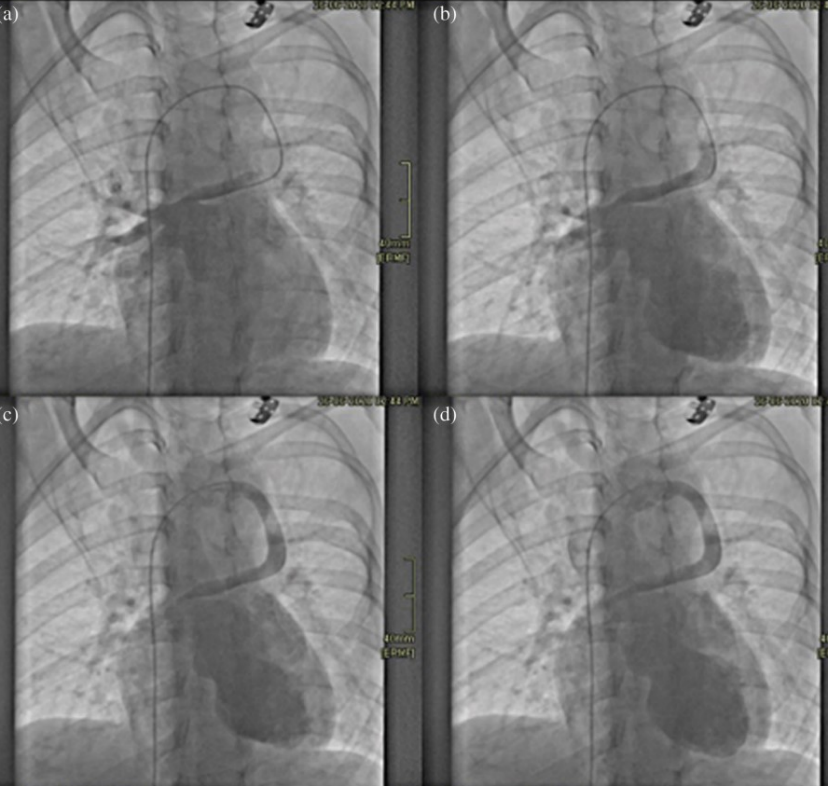
- right-sided PAPVC with a vertical vein connection to left SVC and left atrium [17]: it was reported in a 27-year-old lady with a recent DOE, which had a vertical vein PAPVC with drainage into the left SVC which was occluded percutaneously using a vascular plug without any complication (figure-2).
- right-sided PAPVC with the existence of a left vertical vein connection to the left innominate vein (20): the patient was A 43-year-old lady with a prior therapeutic history of aortic coarctation surgically repaired at the age of 3 years using an end-to-end anastomosis, displayed with 2 years complain of dyspnea and weakness with exercise and palpitations. Work-up revealed (PAPVC) with “dual drainage” with the communication of right-sided PV’s into the left innominate vein with the existence of a left vertical vein. She was effectively treated through percutaneous implantation of a vascular plug occluding the vertical connection of the innominate vein redirecting the stream to the left atrium (figure-3).
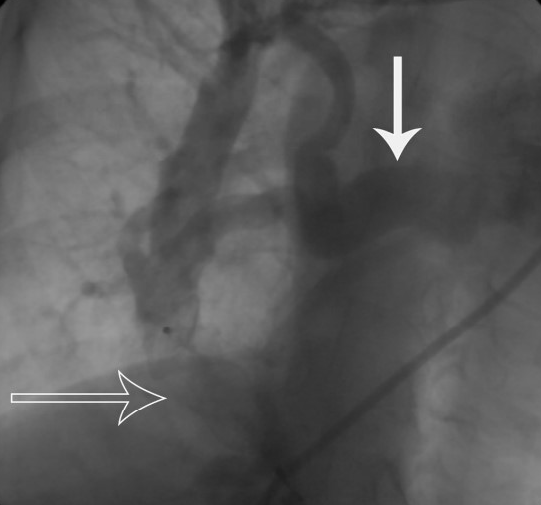
- right pulmonary vein anomalous connection to IVC and LA [9]: in this case-report in a 43-year-old lady with paroxysmal AF and recent DOE, there was a right-sided PAPVC with scimitar vein, which had some collaterals into the LA. Here, the anomalous connection was occluded using a vascular plug without any complication (figure-4).
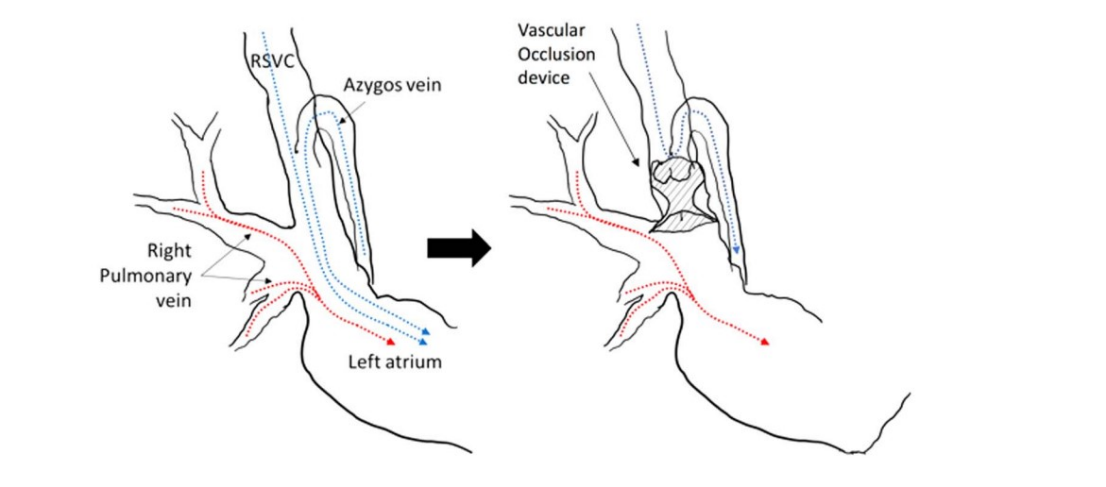
- right-sided PV connection to SVC within 25mm from SVC junction to RA with the existence of left SVC and a connection to LA [19]: in this case-report in a 32-year-old man with a presenting symptom of brain abscess, right upper pulmonary vein, and right middle pulmonary vein connected to SVC; and there was left SVC with drainage into the right atrium. The right SVC was occluded with a Ventricular Septal Defect occluder inferior to the azygous vein, but superior to right-sided abnormal right pulmonary vein drainage. This redirected the right superior caval vein stream to the IVC system through the azygos vein in a retrograde way and permitted the right upper pulmonary vein and right middle pulmonary vein stream to deplete into the left chamber ordinarily, accomplishing the avoidance of right-to-left shunting and permitting ordinary seepage of pulmonary veins into the left chamber (figure-5).
- left-sided PAPVC with the existence of a left vertical vein connection to the left innominate vein and LA [10]:
In this case report in a 67-year-old lady with symptoms of dyspnea and right-sided heart failure, there was a PAPVC with the connection of right PV’s into the left innominate vein. She was managed percutaneously using simultaneous vascular plug and coils. During embolizing the coils, a balloon was inflated as a safety backstop device to deliver the coils in the right place (figure-6).

We experienced three cases in this category in which patients were tried occluding the vertical vein with a VSD occluder device in one and duct occluder device in the other two patients with successful results.
PAPVC is the abnormal connection of at least one but not all pulmonary veins into the right-sided venous system or right atrium. PAPVC from the right lung is twice as frequent as PAPVC from the left lung. The foremost common form of PAPVC is one in which a right upper pulmonary vein connects to the right atrium or the superior vena cava. This shape is almost always related to a sinus venosus type of atrial septal defect (ASD). The right pulmonary veins can moreover deplete into the inferior vena cava. The left pulmonary veins can drain into the innominate vein, the coronary sinus, and, seldom, the cavae, right atrium, or left subclavian vein [2,3,21].
There is some categorization of PAPVC and most anomalous connections are coexistent with secondum type ASD. In case there is an isolated PAPVC, it is most prevalent as a PAPVC of right upper PV which drains into the SVC (22). Left-sided PAPVC has been more reported in adults than children, which might be due to more symptomatic manifestation of the right-sided PAPVC with earlier detection in children [23].
The routine classification of PAPVC does not categorize “dual drainage” freely and these varieties, with a combination of supracardiac and cardiac PAPVC, are incredibly exceptional especially since few past case reports have been published. Besides, the genuine rate of PAPVC cases with double drainage is troublesome to evaluate, since patients are routinely asymptomatic and may escape discovery [10,14,24]. In these anomalies, because of bizarre systemic venous associations, left-to-right shunting is subtle in most cases and if it is hemodynamically significant might lead to right-sided volume overload and longer-term duration would result in right-sided heart failure. The possibility of right-to-left shunting in these patients is scarce and when patients are symptomatic, anatomical correction of this anomaly is, for the most part, recommended at the time of determination. Surgical rectification is the standard choice of treatment [25].
We reviewed all published dual drainage PAPVC cases so far which were tried to manage transcutaneously. Primarily, we decided to categorize these patients into the left or right-sided PAPVC, and second, we defined the feasible anatomical feature of the dual drainage PAPVC. There were a total of five groups of patients in which we could summarize them into the following categories (table-1):
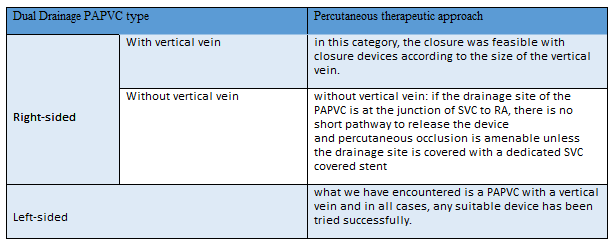
Recently, the three-dimensional printed model is progressively used for the care of patients with congenital heart disease. The 3D printed model permits clinicians to understand the complexity of the anatomy and figure out how to treat these anomalies. It is vital to note that on a 3D-printed model vascular versatility could not be considered and ought to be translated carefully [26,27].
After affirmation of dual drainage PAPVC, transcatheter occlusion may be considered. The world experience detailed by Luciano et al. shows with a satisfactory choice of patients, the interventional methods to divert the anomalous stream only to the left atrium have been successful in embedding both different coils and self-expandable devices [28]. As it has been depicted in this review, vascular plug, VSD occluder, duct occluder, and coils have been the devices to divert the anomalous drainage with the selection depending on the size and type of the dual drainage PAPVC’s. Despite some case reports recommendations to monitor pulmonary pressure increment with balloon inflation, since there is only one anomalous pulmonary venous connection that has a dual drainage pathway, we believe this “balloon inflation” evaluation is not mandatory [9]. Other considerations are detailed device size selection to prevent device embolization and there might be a low risk of thrombotic events related to the device thrombus formation following device deployment [29].
Dual drainage PAPVC is a rare anomaly that is an orphan topic in adult congenital heart disease. With a detailed assessment of this anomaly and selection of left PAPVC with a vertical vein, transcatheter closure is more likely and it flawlessly obviates surgical repair.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
