
Case Report | DOI: https://doi.org/10.31579/2690-1919/246
1 Radiology Department, Usmanu Danfodiyo University, Sokoto, Nigeria.
2 Radiology Department, Usmanu Danfodiyo University Teaching Hospital Sokoto, Nigeria.
*Corresponding Author: Sule Muhammad Baba, Radiology Department, Usmanu Danfodiyo University, Sokoto, Nigeria.
Citation: Sule MB, Shamaki AMB, Dalha A, Ribah MM and Yisa CB. (2022). Tension Pneumocephalus in A Posttraumatic Patient: Computed Tomographic Findings and Case Report. J Clinical Research and Reports, 11(2); DOI:10.31579/2690-1919/246
Copyright: ©2022, Sule Muhammad Baba. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 March 2022 | Accepted: 18 April 2022 | Published: 27 April 2022
Keywords: pneumocephalus; fractures; cerebral edema; road traffic accident; posttraumatic patient; computed tomographic findings
Tension pneumocephalus is an unusual bad life-threatening neurosurgical emergency, this is the equivalent of tension pneumothorax. This often follows head trauma, epidural injections, complicating neurological spinal, craniofacial or sinus surgery.
This is a forty-five-year-old man that was involved in a road traffic accident, was referred for a computed tomography of the brain on account of altered consciousness, irrational behavior, and restlessness.
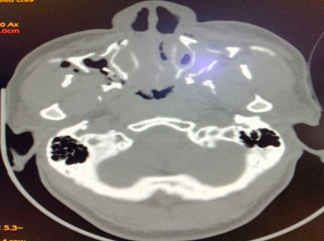
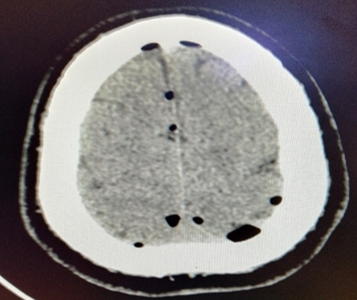
A non-contrast enhanced computed tomography of the brain was done, this demonstrated multiple areas of cortical discontinuity in the facial and skull vaults in keeping with fractures, extensive negative density (HU: -968) hypodensity in the frontal region bilaterally causing marked inferior displacement of both frontal lobes of the brain, with associated splaying of the interhemispheric fissure likened to the ‘Mount Fuji sign’ of severe/tension pneumocephalus. Pockets of negative density hypodensities are also noted in both cerebral hemispheres in keeping with pneumatoceles are also demonstrated. Generalized effacement of sulci and gyri in keeping with cerebral edema is also demonstrated.
The outcome of the patient in the peripheral center was not known as at the time of this report, because all effort to get across to the patient and relations proved abortive.
We present a case of tension pneumocephalus following road transport accident, to review the computed tomographic features due to its peculiar presentation.
Pneumocephalus is defined as the abnormal presence of air in the cranial cavity, with many etiologies, commonest of which is head trauma, tumors, infections and post-surgical procedures of the head1. Pneumocephalus is seen in about 20-30% of patients with post-traumatic cerebrospinal fluid (CSF) fistula [1].
Tension pneumocephalus (TP)refers to continuous accumulation of intracranial air most likely from a ball valve mechanism, this leads to a mass effect on the brain resulting to neurological deterioration and features of herniation [2,3].
TP is a life-threatening neurological emergency that results in intracranial hypertension and mass effect with neurological symptoms, therefore an entity different from pneumocephalus [2,4,5].
TP is believed to occur when there is accumulation of about 65mls of air, although some authors believe that volume of air is an independent determinant of occurrence of tension pneumocephalus [6,8] TP may manifest and present with varying clinical presentation, these are often severe restlessness, deteriorating level of consciousness, focal neurological deficits, and cardiac arrest [9,10].
Intracranial air often suggests an open fracture or that which extends into a sinus, the location of intracranial air could either be in the extradural, subdural, subarachnoid, intraventricular, and intracerebral spaces. The presence of air in the intracerebral and intraventricular spaces indicates tears in the dura and arachnoid layers1.
Imaging plays a vital role in the diagnosis of pneumocephalus, these are either plain radiography, computed tomography (CT) and magnetic resonance imaging, the CT been most sensitive in detecting and localizing minute volumes of intracranial air [1,16,11].
TP most often times need surgical intervention, these include closure at the causative fracture sites, the surgical intervention could either be open or endoscopic repair [1,2].
This is a forty-five-year-old man that was involved in a road traffic accident, was referred from a peripheral health facility for a computed tomography of the brain on account of altered consciousness, irrational behavior, restlessness.
On examination, the patient appeared restless, with labored breathing, decreased level of consciousness, irrational talks, with swellings and open injuries on the face and scalp region,
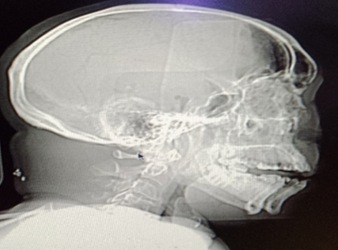
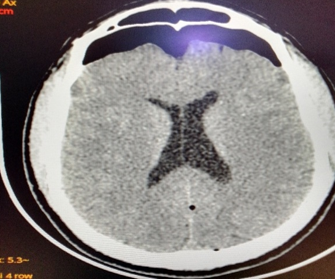
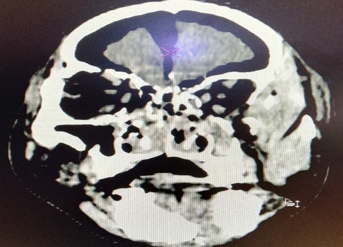
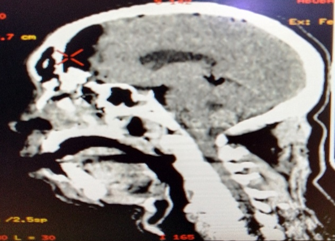
A non-contrast enhanced computed tomography of the brain was done, this demonstrated marked lucency posterior to the frontal bone in keeping with intracranial pneumatocele on the scout image (figure 1), the serial images demonstrated multiple areas of cortical discontinuity in the facial and skull vaults in keeping with fractures (figure 5), extensive negative density (HU: -968) hypodensity in the frontal region bilaterally causing marked inferior displacement of both frontal lobes of the brain, with associated splaying of the interhemispheric fissure likened to the ‘Mount Fuji sign’ of severe/tension pneumocephalus (figures 2-5). Pockets of negative density hypodensities were also noted in both cerebral hemispheres in keeping with pneumatoceles (figure 6). Generalized effacement of sulci and gyri in keeping with cerebral edema is also demonstrated (figures 2,4,6).
The outcome of the patient in the peripheral center was not known as at the time of this report, because all effort to get across to the patient and relations proved abortive.
Pneumocephalus is defined as the abnormal presence of air in the cranial cavity, with many etiologies, commonest of which is head trauma, tumors, infections and post-surgical procedures of the head1. Pneumocephalus is seen in about 20-30% of patients with post-traumatic cerebrospinal fluid (CSF) fistulas1. The case under study had enormous amount of air within the intracranial cavity and was involved in a road traffic accident that lead to multiple fractures and injuries, thereby conforming to this literature.
Tension pneumocephalus (TP)refers to continuous accumulation of intracranial air most likely from a ball valve mechanism, this leads to a mass effect on the brain resulting to neurological deterioration and features of herniation [2,3]. The index case had multiple open skull fractures, and fractures involving the sinuses causing continuous movement of air into the cranial cavity without a route of escaping out of the cranium likened to the ball-valve mechanism, the case also had marked downward compression of the frontal lobes and he also presented with features of neurological deterioration, thereby conforming to these literatures.
TP is believed to occur when there is accumulation of about 65mls of air, although some authors believe that volume of air is an independent determinant of occurrence of tension pneumocephalus [6-8]. The case under review had more than 250mls of intracranial air, he also had clinical and imaging features to suggest tension pneumocephalus, thereby conforming to these literatures.
TP may manifest and present with varying clinical presentation, these are often severe restlessness, deteriorating level of consciousness, focal neurological deficits, and cardiac arrest9,10. The index case presented with most of these symptoms and signs, among which are CSF rhinorrhea, bleeding from orifices, deteriorating Glasgow coma scale, irrational talks, and facial with skull injuries. These are also in conformity to these literatures.
Imaging plays a vital role in the diagnosis of pneumocephalus, these are either plain radiography, computed tomography (CT) and magnetic resonance imaging, the CT been most sensitive in detecting and localizing minute volumes of intracranial air1,6,11. The index case had CT scan of the head and brain where intracranial air was detected, thereby conforming to these literatures.
The main CT finding in a patient with TP are presence of negative density hypodensity in the region causing downward compression of the frontal lobes likened to the ‘Mount Fuji sign’ is considered a critical finding in TP6-8,13. This feature was also demonstrated in the index case, thereby conforming to these literatures. Other CT findings may include pneumatoceles, features of coning, skull bone and air containing spaces fractures to mention but a few1,6,8, these features were also demonstrated in the index case.
TP most often times need surgical intervention and maybe lifesaving if instituted early[1,6,12,14]. As at the time of the report no information from the peripheral facility as whether such treatment was done for the index case.
Computed tomographic imaging should be promptly instituted on most cases of head trauma with deteriorating clinical and neurological features to rule out tension pneumocephalus for prompt institution of management to save the lives of these patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
