
Research Article | DOI: https://doi.org/10.31579/2641-0419/118
*Corresponding Author: Ella Yahud, Assuta Ashdod University Hospital 7747629 Ha-Refua St 7, Ashdod, Israel
Citation: Ella Yahud., Avishag Laish-Farkash., Nir Shlomo., Noam Fink., Ilan Goldenberg, Eli Lev., Elad Asher., (2021) Temporal Trends in Prognosis of Patients with Acute Coronary Syndrome Complicated by Ventricular Tachyarrhythmia. J. Clinical Cardiology and Cardiovascular Interventions, 4(3); Doi:10.31579/2641-0419/118
Copyright: © 2021 Ella Yahud, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 December 2020 | Accepted: 26 January 2021 | Published: 11 February 2021
Keywords: ventricular tachyarrhythmia; all-cause mortality; acute coronary syndrome; NSTEMI; STEMI; risk-factors.
Objectives: To evaluate clinical characteristics and prognosis of patients presented with ventricular tachyarrhythmia (VTA) during the course of acute coronary syndrome (ACS) and to analyze it according to period of presentation.
Background: VTA is an infrequent yet serious complication of ACS. There is limited data regarding the incidence and prognostic implications of VTA in the last decade as compared with the previous decade.
Methods: We evaluated clinical characteristics, major adverse cardiovascular events, short and long- term mortality of patients hospitalized with ACS who were enrolled in the Acute Coronary Syndrome Israeli Survey (ACSIS) during the years 2000-2016. Patients were classified into three groups: no VTA, early VTA (≤48h of onset) and late VTA (>48h of onset). Data were analyzed according to decades of presentation (current decade vs. previous decade).
Results: The study population comprised 15,200 patients. VTA occurred in 487 (3.2%) of patients. Early VTA presented in 373/487 (77%) patients and late VTA in 114/487 (23%) patients. VTA’s, occurring in ACS patients were associated with increased risk of in-hospital, 30-days, 1-year and 5-year mortality rates during both early and late periods in compared with no VTA. Moreover, late VTA was associated with the highest mortality rate with up to 65% in 5-year follow up (p<0.001). Nevertheless, late VTA was associated with lower mortality rate in the current decade (2008-2016) compared with last decade (2000-2006).
Conclusions: Any VTA following ACS was associated with high short and long-term mortality rate. Howevr, over the past decade there has been a significant improvement in survival rates, especially in patients with late VTA. This may be attributed to early and invasive reperfusion therapy, implantable cardioverter defibrillator implantation and better medical treatment.
Ventricular tachyarrhythmia (VTA) especially sustained ventricular tachycardia and ventricular fibrillation, is an infrequent yet serious complication of acute coronary syndrome (ACS). Prior studies reported that VTA complicates 2-8% of ACS cases and has adverse implications on in-hospital and long-term mortality [1, 2]. Early VTAs occur in the first 48 hours of acute myocardial infarction (AMI) and are the most frequent cause of AMI-related death [3]. Late VTAs i.e. > 48 hours of AMI onset are usually associated with ventricular dysfunction [4]. Over the past decade, major advances in the treatment of patients with AMI have occurred and led to improved survival [5]. Currently, however, there is limited data regarding the incidence and temporal trends over recent years in the outcomes of patients presenting with VTA complicating ACS. Moreover, limited information exists regarding the association between VTA observed during ACS hospitalization to short and long-term mortality. This is despite overall enhanced therapy and improved survival among ACS patients. Therefore, the purpose of the current study was to evaluated temporal trends of clinical characteristics and outcomes over the last two decades (2000-2016) among ACS patients presenting with and without VTA who were enrolled in the Acute Coronary Syndrome Israeli Survey (ACSIS) survey.
The present study is a cohort data analysis of patients who were enrolled prospectively in the ACSIS from 2000 to 2016. Details of ACSIS have been previously reported [6]. In brief, this survey is conducted biennially over a 2-month period among ACS patients admitted to coronary care units and cardiology wards in all 27 public hospitals in Israel.
Patient management was at the discretion of the attending physicians. The diagnosis of AMI and ST-segment elevation MI (STEMI) or non- ST-segment elevation MI (NSTEMI), was made by the attending cardiologist according to pre-specified survey criteria based on accepted guidelines. In total 15,200 patients were enrolled in our study. The patients were grouped according to the occurrence of ventricular arrhythmias during the course of index AMI. Data included baseline demographics, medical history, hospital course, procedures, complications, and outcome based on hospital’s charts. Additional data regarding health status, adverse events and medication adherence were collected from the patients via follow-up calls and from outpatients’ medical records one month after hospital discharge. Mortality rates were determined for all patients from hospital and out-patient charts and by matching their identification numbers with the Israeli National Population Register. In- hospital, one year, and five-year all-cause mortality was assessed for the absence of VTA, early VTA and late VTA according to the periods of presentation.
The diagnosis of VTA, sustained ventricular tachycardia or ventricular fibrillation was based on electrocardiogram (ECG) or continuous monitor strips. Sustained ventricular tachycardia was defined as a series of abnormally shaped QRS complexes longer than 120 milliseconds, with a rate 100-250 beats/minute, lasting longer than 30 seconds or requiring electrical cardioversion due to hemodynamic collapse. Ventricular fibrillation was defined as rapid, very irregular rhythm with indiscernible P waves or QRS. Patients were classified into three groups: no VTA; early VTA (≤48h of onset) and late VTA (>48h of onset). Survey periods were divided to early decade (2000-2006) vs. late decade (2008-2016). Primary endpoints were 30-day, 1-year and 5-year mortality rate. Secondary endpoints included 30-day major adverse cardiac events (MACE) (all-cause mortality rate, re-infarction, stent thrombosis and urgent revascularization). Left ventricular ejection fraction (LVEF) was graded according to echocardiography performed at admission in each center.
Demographic, clinical features and the use of in-hospital therapies were reported for all study participants. Multiple logistic regression adjustments for age, gender, diabetes mellitus, chronic renal failure and heart failure and for survey periods was performed to assess the adjusted odds ratio (OR) and 95% confidence interval (CI) of in and out of hospital complications and 30-day, 1 and 5-year mortality rate associated with VTA at any time during and after the admission for ACS. The cumulative probability of all-cause mortality rate was graphically displayed using the Kaplan–Meier method and compared using the log-rank test. In order to evaluate the independent association of VTA with the 5-year all-cause mortality rate outcome, a Cox proportional hazards model was constructed adjusting for survey period. We employed an interaction-term analysis to examine whether the risk of 5-year mortality rate associated with VTA was different in the early period as compared with the late period. Statistical significance was accepted for a 2-sided p<0.05. Statistical analysis was performed using the R Statistical Package (R Foundation for Statistical Computing, Vienna, Austria).
Baseline characteristics
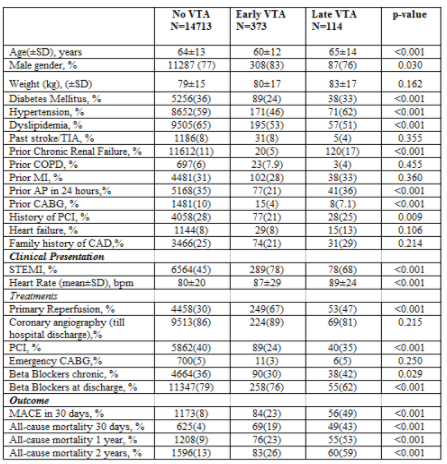
The study population comprised of 15,200 patients with ACS. Of them 11682 (77%) were males, 5383 (35%) suffered from diabetes mellitus 8894 (59%) had a history of arterial hypertension, 9757 (64%) had dyslipidemia and 6931 (46%) presented with STEMI. Patient's baseline characteristics are presented in Table 1.
Table 1: Baseline characteristics by VTA presence
Ventricular tachyarrhythmia characteristics
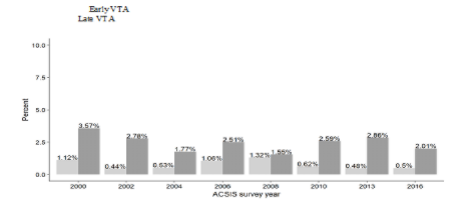
Four hundred eighty seven patients (3.2 %) had VTA during their hospitalization. Among those patients, 373/487 (77%) had early VTA and 114/487 (23%) had late VTA. The incidence of both types of VTA's remained the same in the past 15 years as shown in Figure 1.
Patients with late VTA were older (65±14 vs. 64±13, p<0.001) and had significantly higher incidence of co-morbidities and coronary risk factors such as diabetes mellitus, arterial hypertension, as well as known coronary artery disease, and chronic renal failure as shown in Table 1.
Outcome
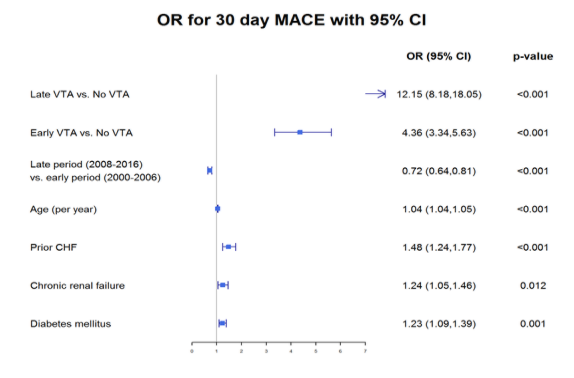
Rate of MACE was higher in late VTA then in early and non-VTA (49% vs. 23% vs. 8%, respectively, p<0.001). As shown with logistic regression model the presence of late VTA was associated with three folds’ higher ratios for 30 days MACE (p<0.001), Figure 2.
In- hospital and 1-year mortality rate were also higher in the presence of late VTA as compared with no VTA [HR 27.44 (95% CI 17.56- 42.49) and 9.78 (95% CI 6.57- 11.18), respectively, p<0.001]. Even after multivariate logistic regression for confounders the presence of early VTA and late VTA, were independently associated with increased risk of in-hospital mortality rate [OR 9.65 (95% CI 7.0-13.13) and 27.64 (95% CI 17.56-42.49), respectively, p<0.001], and early post- discharge mortality rate [OR 8.75 (95% CI 5.98-12.24) and 22.6 (95% CI 14.5-35.62), respectively, p<0.001]. Moreover, multivariable Cox proportional hazard analysis including baseline potential confounders confirmed that 5-year mortality rate was also higher in late VTA then in early and non-VTA (HR 8.27 vs. 2.65, for late and early VTA, respectively 95% CI 2.05-3.42).
Late vs. Early period
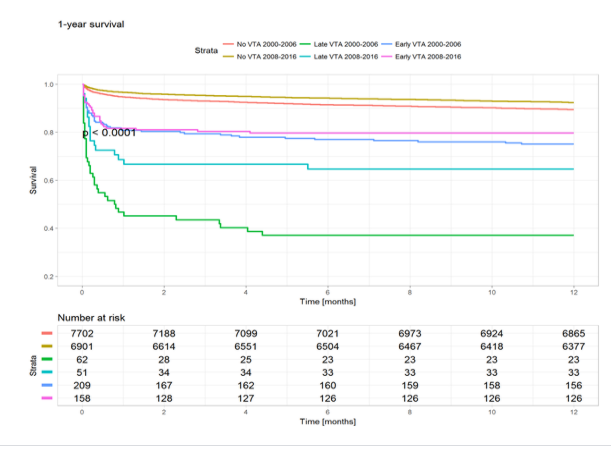
The 1 and 5-year all-cause mortality rate was lower during the late period as compared with the early period for patients with no VTA, early VTA and late VTA (8% vs 10%, 20% vs 25% and 37% vs 65%, all log-rank p <0.001, respectively for 1 year) and (20% vs 23%, 26% vs 29% and 45% vs 75%, all log-rank p <0.001, respectively for 5 years) as shown in Figure 3 and 4. Moreover, the late period was associated with lower all-cause mortality rates for in-hospital, 1 year and 5 years mortality rate (OR 0.56, 0.66 and 0.82, p<0.001, respectively).

In the early period ICD was implanted during hospitalization in 15 (0.2%) patients with no VTA, 3 (1.4%) patients with early VTA and 5 (8%) with late VTA (p<0.001). In the late period in hospital implantation of ICD was performed in 25 (0.4%), 8 (5%) and 0 patients, respectively (p<0.001).
In our study during early period chronic treatment with beta blockers was administered to 34%, 24% and 42.5% of patients with no VTA, early VTA and late VTA respectively, p= 0.018; beta blockers at discharge were prescribed to 78%, 72% and 51% of patients respectively, p<0.001
During the late period 38.5%, 35% and 42% of patients with no VTA, early VTA and late VTA, respectively, used beta blockers chronically, p=0.6 and 80.5%, 81.5%, 73% of patients, respectively, were discharged with beta blockers, p=0.4 Chronic angiotensin-converting-enzyme inhibitor (ACEI) treatment in early period was used in 26%, 31% and 22% of patients with no VTA, early VTA and late VTA p=0.8; ACEI after discharge were prescribed to 61%, 61.5% and 57%, respectively, p=0.9
During the late period chronic ACEI treatment was administered to 32%, 32%, 24% of patients with no VTA, early VTA and late VTA respectively, p=0.08; ACEI in discharge were prescribed to 67%, 66%, 47% of patients respectively, p=0.018
In the current study, VTA occurred in roughly 3% of ACS patients admitted to the hospital with the majority (77%) of those arrhythmias occurred during the first 48 hours of ACS. Moreover, the incidence of both early and late VTA did not change significantly during the years 2000-2016, suggesting it was not related to medical treatment.
Previous data on prognostic significance of VTA is controversial. In the HORIZONS-AMI Trial [7] there was no significant difference in MACE and 3-year mortality rate in patients with or without VTA that occurred after primary percutaneous coronary intervention (PCI). Another recent study, found that in patients with STEMI that survived out of hospital cardiac arrest due to VTA and underwent primary PCI, the 1-year mortality was equal to those without out of hospital cardiac arrest [8]. On the other hand, in the MILIS study [9] the in hospital mortality rate was significantly increased by VTA, especially late VTA, causing cardiac arrest during ACS hospitalization, although there was no difference in mortality rate in the 32-month follow up as compared with patients with no VTA. In APEX AMI trial [10], pre and post primary PCI VTA were also shown to be associated with significantly increased 90 days mortality. Piccini et al. [11] studied a large population of 9000 patients with STEMI and NSTEMI undergoing PCI. In their study, the rate of early VTA was 5.2% and it was also related to increase mortality risk by 4.4 folds as compared with no VTA. Our data is in accord to the aforementioned trials suggesting that VTA occurrence during the course of ACS is not benign. Short and long-term mortality rate was increased dramatically by the presence of early and especially late VTA as compared with no VTA. This was consistent even after adjustment for multiple confounders. In the logistic regression analysis model the presence of late VTA wass associated with 27 folds’ increase of in hospital mortality, 10 folds increased one-year mortality and 8 folds increased 5 years mortality rate. The proposed reason why late VTA carries an increased risk of death might be its association with pump failure and hemodynamic deterioration rather than arrhythmic death [12, 13].
Interestingly, although the overall prognosis of ACS patients improved in the last decade [14] as well as in our study, the most prominent improvement in our study was seen in those who had late VTA, as shown in Figures 3 and 4. Wider use of ACE inhibitors and beta blockers at discharge in the late VTA group, early reperfusion strategy, [15, 16], as well as wider use of implantable and wearable cardioverter defibrillators could explain our findings.
Limitations
Due to its observational non-randomized design, the current study is subject to limitations as described in detail previously [17]. Thus, despite efforts to control for confounding factors by applying multivariate analysis, we cannot exclude unmeasured factors, which could have biased the results. Moreover, data regarding 5 years survival rate is limited in the late period with no long term data since the year 2016. Nevertheless, in spite of these limitations, the study in a multicenter nationwide survey with large study population and long term outcomes.
Conclusions
In summary, in this national, multicenter, contemporary “real life” setting, we did not observe any change in the rate of VTA. Nevertheless, any VTA following AMI was associated with high short and long-term mortality rate. However, over the past decade there has been a significant improvement in survival rates, especially in patients with late VTA that may be attributed to early and invasive reperfusion therapy, implantable cardioverter defibrillator implantation and better medical treatment.
No conflict of interest and no relationship with industry exists
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
